
Abstract
Abstract
Background:
Little is known about the existing barriers to cooperation among health professionals in basic level palliative care for terminally ill patients with cancer in primary health care.
Objective:
The aim of this study was to analyze health professionals' views on interprofessional cooperation in basic level palliative home care for terminally ill cancer patients.
Method:
This study was a qualitative, descriptive study based on 7 semistructured group interviews conducted in the former Aarhus County, Denmark. Forty-three health professionals (23 family physicians, 5 chief physicians, and 15 home care nurses) were interviewed.
Results:
Two main categories of problems were identified: (1) the organization of palliative home care (need for proactive planning from the start of the palliative trajectory, clear distribution of tasks, advancement of more efficient communication pathways, and improved accessibility to all health professionals) and (2) interaction between health professionals (increased knowledge of and respect for the competencies of other health occupations and individuals).
Conclusion:
The study indicates problems with respect to both the organization of the basic level palliative home care and the working culture among health professionals. The main issues: distribution of tasks, information exchange, availability, respect, and personal acquaintance are pivotal to improve the delivery of palliative home care, to training in palliative care and warrant future research.
Introduction
FP, family physician.
In a recent study, we found that relatives of deceased cancer patients feel a need for strengthened interprofessional cooperation or shared care in basic level palliative care. 4 Lack of cooperation caused feelings of insecurity regarding the quality of care and often forced the relatives to take on the role as coordinators.
Shared care necessitates cooperation between health professionals and is evident: “ … when the responsibility for the healthcare of the patient is shared between individuals or teams who are part of separate organizations, or where substantial organizational boundaries exist.” 5 It demands knowledge and acceptance of each other's abilities, qualities, and roles in the delivery of care. 3
This study aimed to describe health professionals' experiences with and views on interprofessional cooperation in basic level palliative home care.
Material and Methods
This study was a qualitative study based on seven semi-structured group interviews with 43 health professionals conducted from May to November 2005.
Setting
The Danish health care system is financed through taxes and provides free and equal access to health care services for Danish citizens. More than 98% of Danish citizens have a registered FP. 6 Danish FPs are gatekeepers for access to specialist treatment and are responsible for providing frontline care 24 hours per day, except for services related to emergency calls.
Palliative specialist teams with physicians, nurses, and other health care workers are available during business hours in major hospitals in Denmark. The FPs can refer patients to these teams or ask them for advice. Palliative home care is divided into a basic and a specialist level of care (Table 1).2,7 The primary care sector comprises the basic level. The palliative specialist team comprises specialist level, and the team works either as consultants or as active professionals in the patient's home, with or without the FPs and the HCNs.
The interviews were conducted in the former Aarhus County (640,000 inhabitants), Denmark (5.5 million inhabitants).
Sample
The informants included FPs, chief physicians (not palliative specialists), and HCNs because they are the professionals primarily involved in basic level palliative home care. They were all contacted by mail and invited to participate. The leading nurses in the local home care services in the 26 municipalities of the former Aarhus County were asked to identify HCNs as possible informants. The FPs and the chief physicians were found in the database of the Danish Medical Association. In all three groups we used a purposeful sampling procedure choosing the informants strategically in order to ensure a wide range of demographic characteristics, i.e. gender, age, geographical location, and specialty of the chief physicians (Table 2). 8 We invited 74 FPs, 17 chief physicians, and 21 HCNs, and 23 (31%), 5 (29%), and 15 (71%) agreed to be interviewed, respectively. The main reason given for not participating was lack of time.
IQR, interquartile range.
Group interviews
All interviews were conducted by M.A.N. at The Research Unit for General Practice, University of Aarhus, and were supervised by J.S. or F.O. All three are FPs. MAN has completed courses in qualitative methods, and J.S. and F.O. are experienced in qualitative research.
The groups interviewed can be seen in Table 3. The interviews lasted from 108 to 138 minutes and were guided by a topic guide designed on the basis of clinical experience, consensus discussions among the authors, and extensive literature studies. The main themes covered in the interviews and examples of questions can be seen in Table 4. The topic guides were revised after each group interview to allow new themes to be included. The interview began with an introduction of the interviewers and the participants, and information about anonymity and publication was given and accepted. Open-ended questions were used. 9 A summary was given at the end of each group interview to obtain an immediate validation of the issues raised.
FPs, family physicians.
Adding the questions: What was good/bad? How could it be improved?
FP, family physician; HCN, home care nurse.
Analysis
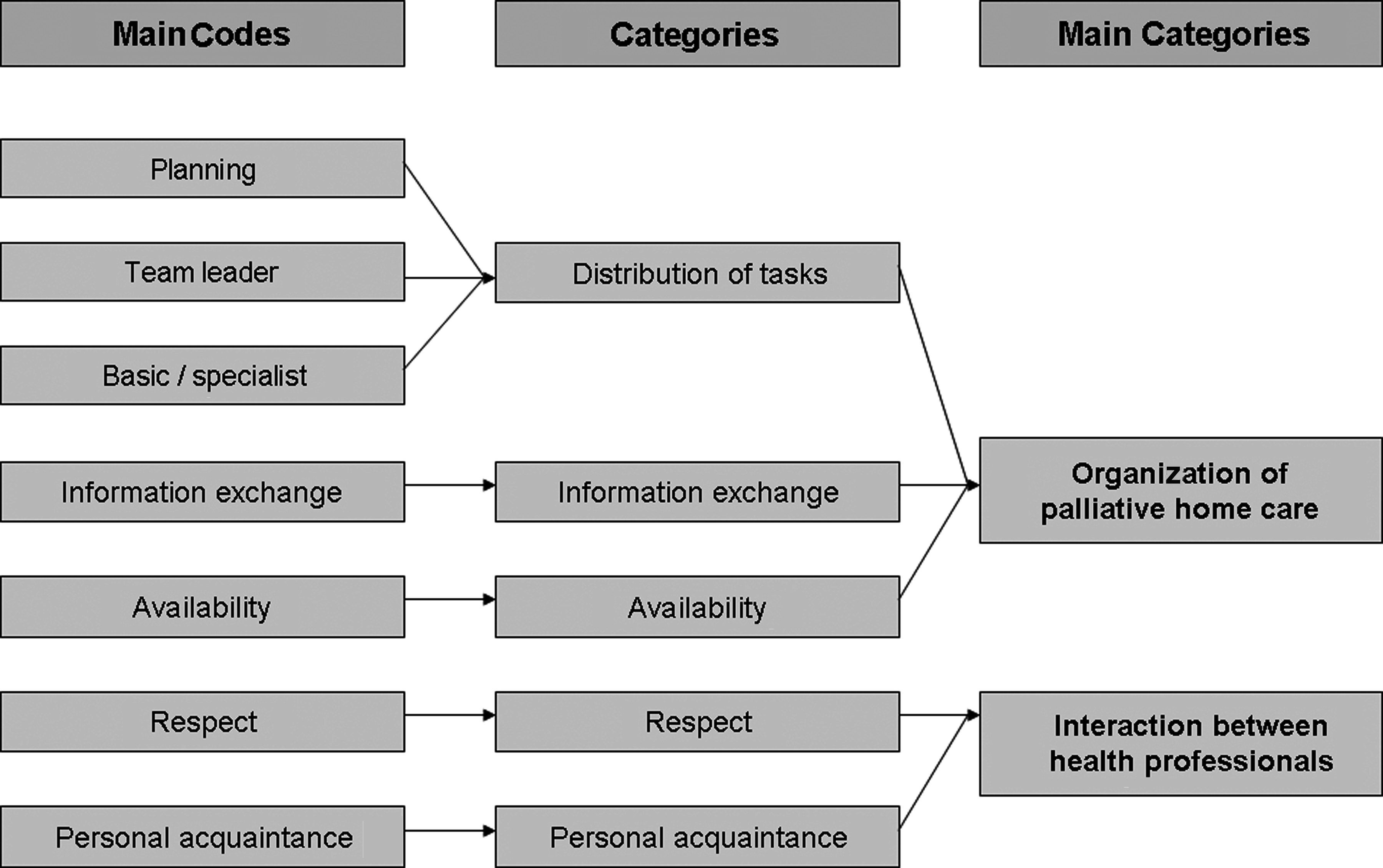
The research approach chosen was qualitative description because we pursued presentation of the facts from the informants' point of view and wanted to stay close to the data.10–12 The group interviews were transcribed verbatim by a trained secretary, and all transcripts were read repeatedly to gain an overall impression before initial coding. 9 All meaningful text units were identified and coded. Subsequently, we examined all the text units again and grouped them into seven groups of main codes that were labeled with a name (Fig. 1). Again, the information in each main code was examined, and they were grouped into five categories, and subsequently into two main categories. In this way we allowed the main categories to evolve from the data instead of imposing a framework a priori. 13 No new categories emerged from the analysis of the last group interview. Because the information in the group interview with just one professional group did not differ from the information in the other groups, data from all of the groups were analyzed together. Agreement on the analysis was reached among the authors after thorough discussion. Software package NVivo (QSR International, Cambridge, MA) was used to assist in the coding, sorting, and retrieval of data.
Categories.
Results
In the group interviews, there was overall agreement on the lack of cooperation among health professionals in palliative care.
Two main categories were identified: organization of palliative home care and interaction between health professionals (Fig. 1). Specific actions proposed by participants to improve both organization of palliative home care and the interaction between health professionals are listed in Table 5.
FP, family physicians.
Organization of Palliative Home Care
Analyses revealed three important aspects of the organization of palliative home care: distribution of tasks, information exchange, and availability (Fig. 1).
Distribution of tasks
The informants' experiences showed that palliative care needs a special focus on careful planning, the team leader role, and separation into basic and specialist levels (Fig. 1).
Planning
The importance of a clear distribution of tasks from the beginning of care was pointed out by the informants. The responsibilities of the health professionals ought to be clear to everyone, including the patient and the relatives.
That is, that one knew who carried the baton at the moment. Right? It should be clear, crystal clear, and be stated in the record who is responsible. We need to communicate and to determine who is responsible for the patient. (FP)
During the interviews, the need in the discharge process for well-defined areas of responsibility for the health professionals was emphasized and some chief physicians admitted that this was not always done.
We do some very good discharges in close and quick contact with the home care services when planning the discharge … I admit that we don't have much contact with the FP concerning this. (Chief physician)
Furthermore, FPs requested that the hospital doctors inform the patient and the relatives that the FP would take over after discharge. The FPs and the HCNs experienced that whenever this information was given, the families did not feel left in limbo, and it helped the FP to reestablish the contact with the family after discharge.
Patients would also feel better about the transfer if they could see that now the hospital doctor is handing over to the FP, who is ready to take over. Many patients feel insecure. They have been discharged, and then what happens? And the patient calls me, maybe, before I have received the letter, and then the handing over has not been successful. (FP)
Team leader
All informants suggested that a well-defined, coordinating person be appointed as the team leader.
In any case, it's very important that someone is aware that they are responsible for coordination. This stops everything from falling apart because everyone believes that someone else is probably taking care of things (FP)
The informants described that the team leader role requires a person who has knowledge of the actual situation at home, the history of the patient, and the disease as well as an ability to facilitate the cooperation between the health care professionals involved. Informants from all three professional groups thought that the team leader ought to be the FP.
When we have discharged a patient, we actually expect the FP to take charge. We should approach patients and ask about their relationship with their FP as he or she becomes a central figure. You need to be realistic in secondary health care—well, we can't be there for the patients like the FP can. (Chief physician)
The FPs in the group interviews were willing to undertake the role as team leaders.
I believe we have a much more natural and central part to play. If we have known the patient for many years, I believe it's absolutely natural that we assume the responsibility. (FP)
Basic or specialist level
The informants described the division into basic and specialist level palliative care as inappropriately blurred and it was not apparent whether the discharging hospital staff considered if the patient's symptoms and situation were a basic or a specialist palliative care task before deciding to involve the specialist palliative team.… then we have simply referred to the palliative specialist team, exactly like we refer to neurologists or prescribe thorax x-rays. (Chief physician)
Information exchange
Informants from all three professional groups described poor information exchange between professionals. FPs and HCNs wanted information about diagnosis, treatment, side effects, prognosis, plan, and especially information about what had been said to the patient and the relatives, and they wanted the information on the day of discharge. These requests for timely information were rarely met.
If the FP is advised concurrently with the discharge of the patient, then that's a totally different situation. We sometimes see that they are advised more than a week after discharge …. (HCN)
All informants welcome a Web page with shared patient-related disease information, professional contact information, and practical information about palliative care in general.
It's possible to communicate with people in Australia in a matter of split seconds. But our two systems cannot see each other … Why can't I enter the hospital's system and see what they wrote when the patient was discharged? (FP)
Availability
The informants pointed out the necessity of cooperating partners being available.
Yes, when a colleague from the hospital calls, I always think it's important. It's no use for us standing with our arms crossed with no will to move, because then we will never have a chance to talk with each other, will we? (FP)
Many informants reported spending a great deal of time getting in touch with each other. They asked for facilitated communication between the health professionals, direct telephone numbers, and regular telephone hours.
Unfortunately, I mostly find that doctors aren't there and that we need to spend an hour on the phone waiting just to get through … I think the odds are against us at times. (HCN)
FPs often felt alone in the treatment of terminally ill patients. They called for easier access to specialist advice and supervision.
I believe the palliative team can do things that I can't … I've had contact with them several times concerning pain therapy. It's made me feel more secure. (FP)
Interaction between Health Professionals
Analyses revealed two important aspects of the interaction between health professionals: Respect and personal acquaintance.
Respect
Everyone agreed that trust and mutual respect, both personally and professionally, were a prerequisite for successful cooperation.
I very much agree that mutual trust makes you feel secure. (HCN)
Informants were aware that prejudice and lack of respect were barriers to cooperation and could cause distress among patients and relatives.
At the hospitals we try hard not to hold others responsible for what has happened. We may internally criticize each other, but we never criticize a FP when communicating with patients. If a colleague does so, we address him or her directly, because it is unacceptable. (Chief physician)
Several FPs and HCNs expressed great respect for each other's work.
We've got a bunch of brilliant home nurses. And I agree with them on most issues. I really haven't got anything negative to say about any of the contacts I've had. Because things have actually worked out well. (FP)
However, some informants were disrespectful of other health professionals, especially when they met other professionals who were not as enthusiastic about palliative care. Several FPs revealed disrespect for hospital doctors, especially their unwillingness to establish teamwork with FPs. Some HCNs and chief physicians, on the other hand, revealed disrespect for FPs, primarily regarding the FPs' competencies and personal merits. Chief physicians stated that they sometimes referred directly to the specialist palliative team because of uncertainty about FPs' competencies and interest in palliative care.
The solution proposed by participants to improve respect among different health professionals was a higher degree of personal acquaintance and contact among them.
Personal acquaintance
Informants in all professional groups concurrently called for personal acquaintance with each other as a method to facilitate cooperation.
Yes, personal contact, I believe, is still preferable to electronic contact. And you may get totally different information” (Chief physician)
They had all experienced personal acquaintance breaking down prejudices and disrespect and causing better cooperation.
Being able to put a face on the people you work with is immensely important. You get a much better understanding of who they are. (HCN)
FPs and HCNs said that personal acquaintance promotes team spirit and increases mutual responsibility.
How would I ever be able to do my job if I didn't have a close relation to the HCNs?—If we didn't know each other really well. (FP)
Discussion
Our findings suggest a need for improved cooperation between the health professionals when delivering palliative home care. Improved cooperation requires proactive planning from the start of the palliative course, clear distribution of tasks, better and easier communication pathways, and improved accessibility to all health professionals. Possibly, the most important finding was the need for a better working culture and a willingness to be equal team partners with mutual respect and better knowledge of each other's professional competencies and personal merits.
Another important issue is that the hospital doctors did not always seem to be aware of the division into basic and specialist level palliative care. This could be due to the fact that palliative care and palliative education have been given low priority in Denmark. 14
Interviews are an appropriate method for exploring the informants' perspectives and experiences concerning a specific topic. The advantage of group interviews is the interaction in the group which can facilitate the emergence of new themes. 15
Being aware of the fact that the interviewers (M.A.N., J.S., and F.O.) were all FPs, we tried to minimize the influence this fact could have on the interviews and the analysis. 9
In relation to the informants, we used a purposeful sampling procedure choosing the informants strategically in order to ensure a wide range of demographic characteristics. In that way we minimized the bias that can result from interviewing a certain group of health care providers, e.g., health professionals from the same small area of the county. The number of participating chief physicians was sparse, but the five physicians worked in five different fields and still had similar opinions on the important issues.
With respect to generalizability of the study, the low-inference analytic approach “qualitative description” reduces the possibility of making generalizations. Furthermore, health services and the delivery of palliative care vary considerably between countries, and the findings of this study seem most relevant to countries with a primary health care sector as frontline service. However, our rich descriptive summary yielded working hypotheses for future theory-based research in cooperation among professionals in palliative care.
In line with findings from other studies, we found that FPs find coordination of palliative care an essential task,16,17 but they request easier access to specialist backup. 18
Also in line with other studies, we found problems with the organization of palliative care, feelings of “struggling with the system,” 19 and an agreement on the importance of naming a team leader in palliative home care.20,21 Similar to other studies, we found insufficient information exchange between hospitals and community-based services as well as inadequate availability of health professionals.18,19
A systematic review concluded that professionals must acknowledge the strengths of other health professionals, 3 and this corresponds with the importance of respect found in the present study. It is thought-provoking that even bereaved relatives see this as a barrier to successful palliative care. 4 We and others have found that whenever the health professionals met each another in person, the chance of mutual respect was increased. 22 In our study, health professionals experienced that personal acquaintance among health professionals also engenders team spirit and responsibility. The role of health professionals' trust and respect for each other in the delivery of care needs further exploration because it would be peculiar if these problems only exist in palliative care.
Improving shared care in palliative home care and creating a system based on cooperation and mutual respect are major challenges that require further research. Finally, our research showed a need for improved communication, indicating that better IT systems and common Web-based information may be important tools to overcome some of the communication difficulties. The issues about shared care pointed out in Table 5 are important issues to consider, optimizing and training in palliative care in all countries with a primary and a secondary health care sector.
Conclusion
The study indicates problems with respect to both the organization of the basic level palliative home care and the working culture among health professionals. The main issues: distribution of tasks, information exchange, availability, respect, and personal acquaintance are pivotal to improve the delivery of palliative home care, to training in palliative care and warrant future research.
Footnotes
Acknowledgments
Profound gratitude is extended to participating informants.
This work was supported by the Aarhus County Research Fund for the Clinical Development and Research in General Practice and across the Primary and Secondary Health Care Sectors [4-01-3-04] and the Danish National Research Foundation for Primary Care [585-457808].
According to the Scientific Committee for the County of Aarhus, Denmark, the Biomedical Research Ethics Committee System Act does not apply to this study.
Author Disclosure Statement
No competing financial interests exist.