
Abstract
Abstract
Purpose:
Most Canadians die in inpatient settings. Our aim was to determine the availability of medical services, programs, and care for common palliative procedures, in hospices, palliative care units (PCUs), and hospital medical wards (MWs) providing inpatient palliative care in Ontario, Canada.
Methods:
We identified facilities providing inpatient palliative care using the Ontario Hospital Association (OHA) and Hospice Association of Ontario (HAO) websites. An electronic survey was sent to the person responsible for palliative care at each facility. We compared services available among the three types of units, using Fisher's exact and Kruskal-Wallis tests.
Results:
Of 128 surveys sent, 102 (80%) were completed and returned, from 58 MWs, 31 PCUs, and 13 hospices. MWs were the most common location of palliative care overall, particularly in rural areas. PCUs were most likely to provide care for common procedures (e.g., tracheostomy, nephrostomy; p<0.01); methadone for pain management (p<0.0001); and palliative radiation (p<0.01). MWs were most likely to offer intravenous chemotherapy and antibiotics (p<0.01). Transfusions were available in most PCUs and MWs, but only in one hospice (p<0.0001). Hospices were most likely to provide complementary therapies. Lack of financial support and human resources were the most frequent perceived barriers to providing quality palliative care.
Conclusions:
There is considerable variability of available services depending on the setting where inpatient palliative care is provided. Further financial support and resources are required to ensure consistent high quality of care in both urban and rural areas.
Introduction
Although an increasing number of Canadians are dying at home, more than 60% of deaths occur in inpatient settings. 1 Reasons for this continued high prevalence of hospital deaths may include insufficient health care resources for home care, lack of availability of family members to provide care, or the need for specialized nursing or procedures that cannot be provided in the home.1,2 Patients with advanced illness and their families are encouraged to plan for the end of life by completing advance directives and discussing their end-of-life preferences, including their preferred place of death, with health care providers and family members. 3 Previous publications have described the prevalence and structure of palliative care programs in U.S. cancer centers 4 and general hospitals,5,6 and academic palliative care programs have published information regarding their palliative care units (PCUs).7-11 As well, individual units often provide pamphlets and information about the general nature of the care provided. However, there has been no systematic investigation of the specific medical services and treatments offered in various inpatient settings and the differences that may exist among them.
Inpatient palliative care in Canada is provided in residential hospices or in hospitals, where care is provided either on specialized PCUs or on general or subspecialty (usually oncology) medical wards (MWs). Unlike the United States, Canada does not have a separate hospice system that necessitates a choice between hospice and life-sustaining treatments; 12 however, almost all Canadian residential hospices provide exclusively end-of-life care, in a home-like residential setting. The Ontario Ministry of Health End-Of-Life Care Strategy increased funding for residential hospices in 2005, 13 but a large proportion of the budget for hospices still comes from private funds, and they rely heavily on volunteers. In contrast, PCUs are located in ministry-funded hospitals, although access to acute medical services within the hospital may be restricted according to unit or hospital policies. MWs that provide palliative care may or may not have a small number of beds designated for this purpose and may or may not have access to a consultant palliative care team.
In order to make improvements to the delivery and accessibility of palliative care, it is necessary to identify what services units are currently able to provide and what barriers may limit their availability. The primary goal of this study was to determine the availability of medical services and procedures and of complementary recreational and spiritual programs in institutions offering inpatient palliative care in Ontario, Canada. Secondary goals were to compare services, programs, and procedures provided in residential hospices, PCUs, and MWs, and to identify barriers to their provision.
Methods
Survey design
The survey was developed after a comprehensive literature review and with input by a multidisciplinary palliative care team consisting of five physicians, a social worker, a spiritual care provider, a pharmacist, and an advanced practice nurse. The 56-question survey assessed four main areas regarding inpatient palliative care: general characteristics; medical services and procedures available; complementary therapies and recreational programs offered; and challenges to providing care. General characteristics included the location and type of facility; number of beds in the overall facility and designated for palliative care; specialized staff available; affiliation with a university or college; and requirements for admission, such as a minimum age, specific diagnosis, or written do-not-resuscitate (DNR) order. The question regarding medical services and procedures was phrased, “Please check which of the following patient medical needs you can accommodate at your facility.” The survey was piloted on three residential hospices and 3 PCUs and further modified based on the feedback provided. The University Health Network research ethics board reviewed this study and granted approval.
Survey sample
Figure 1 shows a flow diagram of how facilities were identified and of the survey completion rates. Facilities providing hospice or palliative care in Ontario, Canada, were identified using the Ontario Hospital Association (OHA) 14 and the Hospice Association of Ontario (HAO) 15 websites. Health care facilities are listed on the OHA website by region; telephone contact information for each health care facility was obtained by searching each region on the website. Two hundred and sixty-one inpatient health care facilities were identified using this method; 233 remained after excluding mental health (n=16) and rehabilitation facilities (n=11) and a diabetes clinic (n=1). Using the HAO directory, 19 residential hospices were identified. Two further hospices known to the investigators but not listed in the directory were also included.
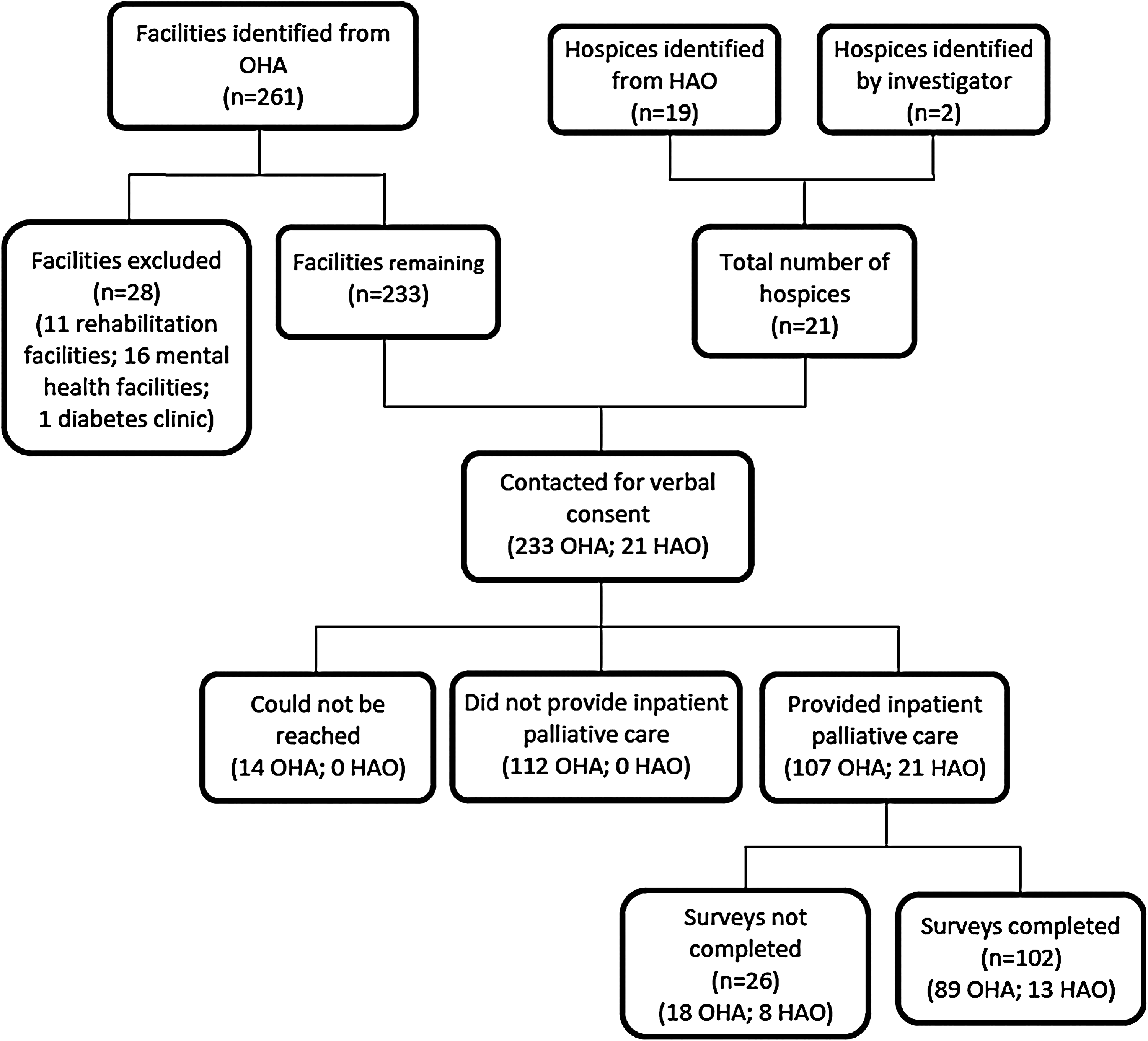
Flow diagram of recruitment process.
With contact information from the websites, each of the 254 facilities was telephoned by one of the investigators (ED) and asked if their facility provided inpatient hospice/palliative care. If so, then the investigator requested the telephone number of the person in charge of hospice/palliative care for the facility, who in turn was called, informed of the purpose and nature of the study, and asked to provide verbal consent to receive a survey. If it was discovered that incorrect contact information had been provided, the investigator requested the correct telephone number, so that this person could be reached. Consenting participants provided their e-mail address so that the survey could be sent and completed electronically. At least two attempts were made to contact each palliative care representative by telephone. A total of 128 facilities provided inpatient hospice/palliative care (21 HAO facilities and 107 OHA facilities) and provided verbal consent to receive the survey; 14 OHA palliative care contacts could not be reached directly and did not answer voicemail messages.
Participants provided the name of their facility, so that they could also participate in a future online directory providing information on services accessible to patients and care providers. All participants were informed that published results of the survey would be anonymous. Surveys were sent to the 128 participating facilities. A reminder telephone call was placed at two weeks and electronic reminders were sent at one and five months. Data collection was performed between October 2008 and March 2009.
Statistical analysis
The statistical analyses were performed using SAS® (Cary, NC). Summative statistics were used to describe the characteristics and staff availability at each type of unit. Rural versus urban location of the facility was assessed using the designation of community of ≥10,000 as urban/city and <10,000 as rural/small town. 16 Fisher's exact test was used to compare medical services and programs offered at each type of unit. The nonparametric Kruskal-Wallis test was used to compare the perceived challenges to providing hospice palliative care on the four-item Likert scale.
Results
Sample characteristics
Of 128 surveys sent, 102 (80%) were completed and returned (Figure 1). We also calculated a conservative overall completion rate, including those OHA contacts whose units could not be assessed for eligibility due to lack of telephone response, which was 72% (102/142). Respondents were nurses (34%), unit managers (28%), executive directors (18%), social workers/admissions coordinators (16%), or physicians (3%). There was representation from each of the 14 Local Health Integration Network districts in Ontario (Table 1).
Source: Statistics Canada Community Profiles. 36
ACW, acute care ward; LHIN, local health integration network; PCU, palliative care unit.
Table 2 summarizes the characteristics of the health care facilities providing palliative care. The size of facility ranged from freestanding hospices or rural health care facilities of less than 16 beds to large hospitals of more than 300 beds. Most facilities had 15 palliative care beds or less and required no specific admission diagnosis. Admission was restricted to patients with cancer for one hospice, four PCUs, and three units with palliative care beds. Approximately 65% of hospices and PCUs but only 26% of MWs required a DNR order. Admission was generally restricted to adults; there were two pediatric units and two limited to patients aged 55 and over.
Rural/small town refers to municipalities with a population of less than 10,000 and urban/city refers to municipalities with a population of 10,000 or more.16
ACW, acute care ward; DNR, do-not-resuscitate; PCU, palliative care unit.
Although the information about procedures/service availability in this survey was about inpatient care, we also asked which other palliative care services were provided. Community outreach teams were most commonly associated with hospices (31% of residential hospices also had such teams), while inpatient consultation services were most commonly found in hospitals with PCUs (68%). Few facilities had a palliative care clinic (13%, 14/102). In rural locations, inpatient palliative care was mostly provided on MWs (25/28 rural facilities provided inpatient care in this manner), whereas in urban locations, 55% (41/74) of facilities were either residential hospices or PCUs.
Table 3 describes specialized staff available at each type of unit. Greater than 90% of residential hospices and PCUs had access to a palliative care physician, whereas this was the case for less than 50% of MWs. PCUs were most likely to have access to other specialized health care professionals.
Includes clinical nurse specialist and nurse practitioner.
ACW, acute care ward; PCU, palliative care unit.
Availability of medical services
No medical service was universally offered by all facilities (Table 4). Services available at greater than 80% of units in all three categories were oxygen, wound care, suctioning, care for central lines, and colostomy/ileostomy care. Services offered by less than 50% of units in all three categories were dialysis, intravenous chemotherapy, intraspinal analgesia, and radiation treatment.
ACW, acute care ward; CADD, Continuous Ambulatory Delivery Device; MRSA, Methicillin Resistant Staphylococcus Aureus; PCU, palliative care unit; PICC, Peripherally Inserted Central Catheter; VRE, Vancomycin Resistant Enterococcus.
PCUs were most likely to be able to provide care for patients with medical procedures, such as tracheostomies and nephrostomies; to have access to physicians who were able to prescribe methadone for pain management; to accommodate patients with antibiotic-resistant infections; and to offer palliative radiation treatment. MWs were most likely to offer aggressive medical therapies, such as IV chemotherapy and IV antibiotics. Transfusions of blood products were available in the majority of PCUs and MWs, but only in one hospice.
Availability of supportive care programs
All hospices and PCUs offered some type of supportive care program, with less availability at MWs (Table 5). Residential hospices were more likely than PCUs or MWs to provide some complementary therapies, such as therapeutic touch, massage therapy, chiropractic therapy, and acupuncture. PCUs were most likely to offer individual counseling and recreation therapy. A minority of units of any type offered group counseling.
ACW, acute care ward; PCU, palliative care unit.
Perceived barriers to providing palliative care
Lack of financial support and lack of human resources were the most commonly perceived barriers to providing quality inpatient palliative care at all three types of facility (Table 6). However, 92% of hospices identified lack of financial resources as a moderate to severe challenge, compared to 70% of PCUs and 61% of MWs (p=0.02). Late referrals were mainly thought to be a barrier for hospices (73%) rather than for PCUs (37%) and MWs (28%; p=0.01). Geographic limitations were perceived to be a problem only for a minority of facilities.
Discussion
In this survey of inpatient palliative care in Canada's most populous province we found considerable variability of available services. Palliative care was provided on MWs in the majority of facilities and in almost 90% of those in rural areas. These wards were least likely to require a DNR order, and most likely to offer access to more aggressive medical therapies, such as intravenous chemotherapy and intravenous antibiotics. More than 30% of MWs did not offer care for chest tubes, nephrostomy tubes, or tracheostomies, more than 30% did not provide thoracentesis or paracentesis, and 28% did not provide care for intrathecal pain pumps. Only half had access to a palliative care consultation service, and fewer than half had access to a palliative care physician or to individual psychosocial counseling.
Given that most Canadians die on MWs in hospitals, 1 and that general medical staff tend to have inadequate training in palliative care,17,18 efforts should be made to recruit specialized palliative care staff who can provide advice to primary care clinicians and to increase training of other clinical staff in palliative care. This training should include not only pain and symptom management, but also care for basic medical devices such as tracheostomies and chest tubes, and training in counseling and psychosocial care. The latter is particularly compelling given the results of a recent survey of Canadian patients and caregivers, which defined improved psychological and spiritual support, and better communication and decision making, as priorities for improving end-of-life care. 19
Although palliative care services and personnel were most likely to be available in PCUs, not one type of service or specialized staff was universally provided. In particular, basic palliative measures, such as oxygen, intravenous hydration, suctioning, thoracentesis and paracentesis, were not always available. It is noteworthy that some of these services can be provided at home. Oxygen can be provided in the home setting, and provides palliative benefit for dyspnea for patients with hypoxemia.20,21 Intravenous hydration can also be provided at home and may prevent or alleviate delirium, sedation, and myoclonus.22,23 Paracentesis and thoracentesis, which were offered at a minority of hospices and only approximately a third of MWs and PCUs, are procedures that have been proven to palliate associated symptoms and improve quality of life.24,25 Although some facilities may lack proper imaging resources to prevent or rule out complications, these bedside procedures may offer substantial palliation; an effort should be made to ensure that they are more readily available.
Methadone for pain management was not available in 15% of PCUs, 33% of hospices, and 62% of MWs. This unique opioid agonist is useful for cancer patients with refractory pain or dose-limiting toxicity with other opioids. 26 Because methadone is a controlled substance, Canadian physicians who wish to prescribe it need to apply for an exemption, or “methadone license” under section 56 of the Controlled Drugs and Substances Act. 27 However, those who apply are generally specialists in pain control or palliative care, with most general physicians lacking both a license and experience in prescribing and titrating methadone. As a result, patients who have been successfully rotated to methadone for intractable pain in a tertiary PCU may then have no physician able to provide ongoing supervision and prescription when transfer is attempted to another facility, particularly in rural areas where palliative care is provided mainly on MWs. Given the increased availability and use of methadone for pain control, all physicians providing palliative care should be familiar with this medication and have a license to use it.
A minority of facilities had palliative care outpatient clinics. Although this is not surprising for residential hospices, these clinics were also not available at more than 80% of hospitals offering palliative care in PCUs or MWs. A recent survey of cancer programs in the United States similarly found that less than half had palliative care outpatient services. 4 In a randomized trial of patients with lung cancer, early integration of palliative care improved quality of life, and was associated with less aggressive end-of-life care and longer median survival compared to standard oncology care alone. 28 Palliative care clinics are necessary for early integration and can improve both symptom control and patient satisfaction in cancer and noncancer populations.28-30 The survey responses regarding community outreach teams are more difficult to interpret, as these teams tend to operate on a community-wide basis, each encompassing catchment areas from several hospitals. 31 Thus although a particular facility may not itself offer home palliative care, this service may still be available at that facility, either through an external specialized hospice/palliative care program or by the patient's family physician.
A minority of respondents from all three types of facilities felt that geographic barriers limited the provision of high quality palliative care at their facility. However, they were responding from their perspective as care providers, rather than from a larger health services perspective, and difficulties of access to hospices and PCUs for patients in rural settings have been described in other studies. 32 A majority of respondents identified lack of human resources and financial support as moderate to severe barriers. Financial support was a particular concern for hospices, which is not surprising, in that hospices in Ontario are only partially funded by the Ministry of Health and rely heavily on less stable private funding. Nevertheless, financial concerns were also prevalent for a majority of PCUs and MWs. A majority of residential hospice respondents indicated that late referrals were a moderate to severe barrier compared to a minority of those from PCUs or MWs. However, the services provided by residential hospices may allow them to provide care only at the very end of life, with less availability of treatments for palliation earlier in the disease course, such as paracentesis, thoracentesis, intravenous hydration, intravenous antibiotics, or transfusions.
This study has several limitations. The sample was obtained from two websites that have the most comprehensive listings of facilities in the province, and there was representation from every Ontario Local Health Integration Network region. However, these listings may not be complete and there were likely hospices or hospitals providing palliative care that were not included. As well, despite an attempt to be inclusive, there were likely services/procedures that were omitted; subcutaneous hydration is one omitted procedure that would have been useful to include. The non-anonymous nature of the survey could have prevented participants from providing truthful answers regarding barriers to care, although answers regarding services provided might be more accurate due to transparency of the source. We did not specify whether availability of staff from various disciplines was in person or by telephone consultation, though the former was intended, nor did we ask more specifically about availability in terms of hours per day or days per week. There may also be response bias, depending on the role of the person who completed the survey. Lastly, we did not include nursing homes in our survey, which are the site of death for approximately 30% of Canadians. 1 The limited research about end-of-life care provided in long-term care settings suggests that there are unmet symptom needs, 33 which may be due to inadequate staffing and lack of resources.34,35 Further research in this area is needed.
In summary, we have found a broad range and variability of available palliative care services throughout the province. Regional inpatient palliative care directories providing information about available medical services would help patients and care providers to choose an inpatient palliative care setting that meets individual needs. However, such choices are not always possible, particularly in rural areas, where palliative care is offered mostly on MWs. Further efforts are required to ensure that all inpatient palliative care facilities have sufficient resources to supply basic palliative measures to patients and to offer care for common interventional procedures. Dissemination of information about available resources may be useful not only to inform referral decisions, but also for advocacy to enhance the acquisition of resources and standards of palliative care.
Footnotes
Acknowledgments
This research was funded in part by the Bluma Appel Research Fund and by the Ontario Ministry of Health and Long Term Care. The views expressed do not necessarily reflect those of the funding agencies, which had no role in the study design, data collection, analysis and interpretation, writing, or decision to submit for publication.
Author Disclosure Statement
No competing financial interests exist for any of the authors.