
Abstract
Abstract
Background:
Oral administration of medication is often difficult in terminally ill patients with cancer. These patients require intravenous routes for high-dose opioid administration and/or parenteral nutrition. When the superior vena cava (SVC) is unsuitable for central vein catheter insertion (i.e., in patients with mediastinal masses involving the SVC), alternative access routes are needed. Of these, the femoral vein is most utilized. In our experience, the femoral tunneled catheter (FTC) is easy and safe to use. We retrospectively studied FTC outcomes in terminally ill patients with cancer.
Materials and methods:
Charts of consecutive patients admitted to the palliative care unit between April 2008 and December 2011 were reviewed. FTC is inserted into the vein by the single-puncture method using a 16-gauge catheter with a 14-gauge peel-away introducer.
Results:
Eleven patients underwent FTC insertion. In total, there were 207 days of FTC placement; the mean period in place was 19±15 days. Eight patients received parenteral opioid therapy, high doses in four cases, via FTCs. Complications were incidental arterial puncture and poor infusion rate due to hip joint bending in one case each. Neither catheter-related infection nor clinical venous thrombosis occurred.
Conclusions:
FTCs were successfully inserted, with a low complication rate. FTC, a simple technique, might be an acceptable alternative in selected terminally ill patients with cancer, when SVC insertion is difficult or contraindicated.
Introduction
However, the selected patients need intravenous routes to administer high-dose opioids when subcutaneous administration is impossible, 3 to provide osmotic diuretics, 4 blood components, 5 and total parenteral nutrition. 6 In general, central venous catheters (CVC) are inserted into the superior vena cava (SVC) via the subclavian or jugular vein. Currently, peripherally inserted central venous catheters (PICCs) are frequently used for patients with advanced cancer, mainly to maintain chemotherapy, nutritional therapy, and/or for symptom control.7,8
The subclavian or jugular venous access route and PICC may be difficult or contraindicated in some clinical situations (in patients with mediastinal masses, SVC thrombosis, or massive cutaneous metastases). In addition, subclavian or jugular vein catheterization may involve life-threatening procedure-related complications (pneumothorax, hemothorax, and arterial puncture) in terminally ill patients with cancer. 9 In these situations, alternative access routes are needed. The femoral vein is the alternative most utilized.
One problem with femoral access is catheter-related infection, which has an unacceptably high rate because of fecal contamination. 10 However, use of subcutaneous tunneling can reduce catheter-related infections.11–15
We have experience using a catheter with a peel-away introducer in the femoral vein and were able to insert this catheter into the inferior vena cava easily and safely. We assessed the frequency, medical indications, intervals of femoral tunneled catheter (FTC) use, and complications in terminally ill patients with cancer.
Patients and Methods
Charts of consecutive patients admitted to our certified palliative care unit between April 2008 and December 2011 were retrospectively reviewed. Information collected on patients undergoing FTC included age, gender, primary tumor location, Eastern Cooperative Oncology Group (ECOG) performance status, medical indication for intravenous route, reason for selecting femoral access, and intervals between FTC placement and catheter-associated complications.
FTC was inserted in routine clinical practice, with written informed consent from all patients. This study was approved at an ethics meeting of the palliative care unit.
Treatment setting
Our palliative care unit has 18 beds in a 400-bed local cancer center. Inpatients (200 per year) are usually referred from home, for end-of-life care and/or intensive symptom control. Our unit has 3 attending physicians and 20 nurses, in addition to psychologists, a pain specialist service, rehabilitation staff, and volunteers.
FTC insertion procedure
All catheters are inserted by the palliative care physician in the patient room with sterile barrier precautions. FTC is inserted into the vein by the single-puncture method using a 16-gauge catheter (Argyle, 16-gauge single-lumen 70-cm catheter; Nippon Sherwood, Tokyo, Japan), packaged with a 14-gauge peel-away introducer needle and 3-mL syringe.
The technique is as follows (Fig. 1).
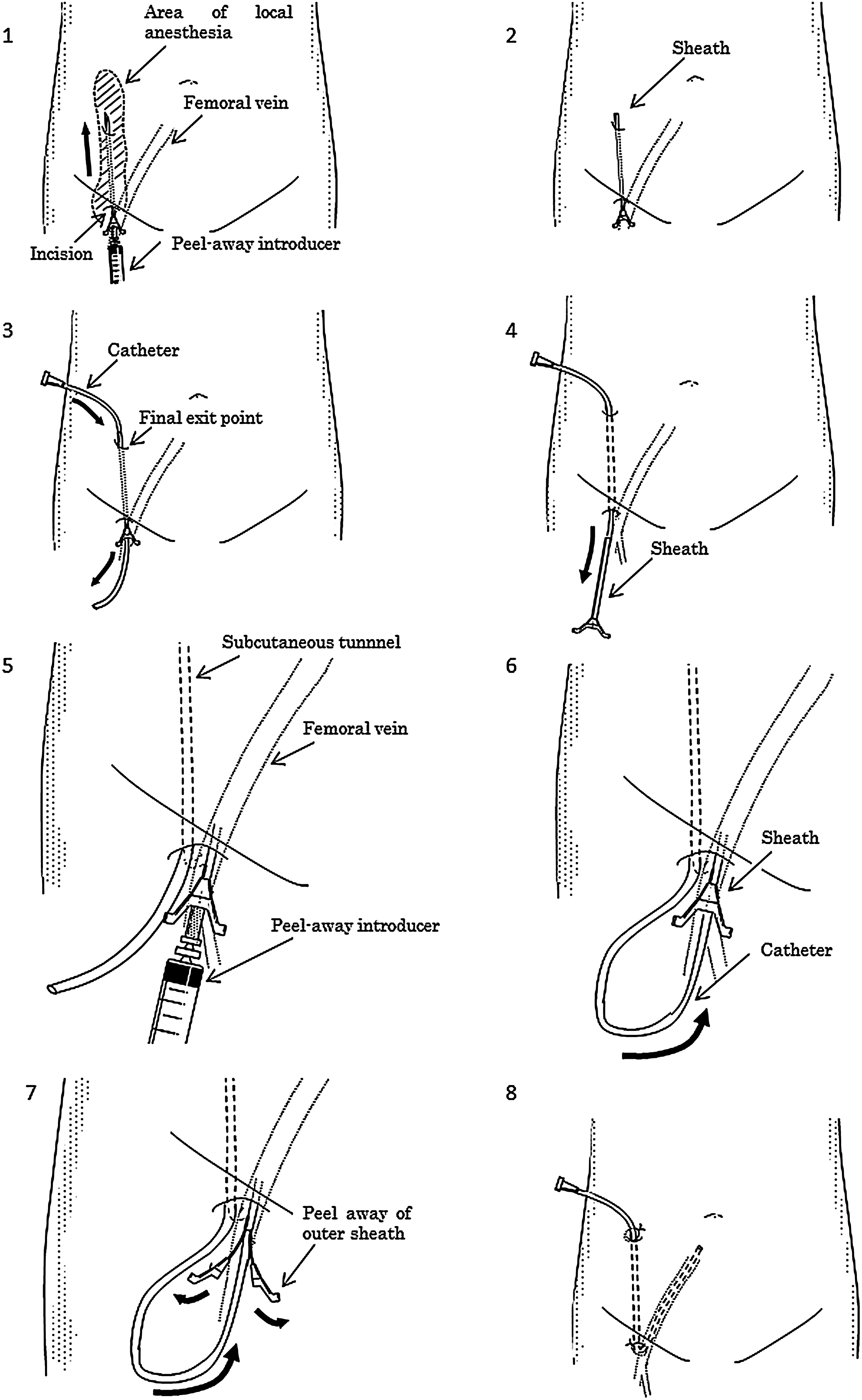
FTC insertion procedure.
Before insertion, we administer anesthesia for the right groin region and abdomen at the umbilicus level using a local anesthetic-loaded syringe with a long 23-gauge needle. If necessary, endovenous sedation is added. Then, the 23-gauge needle is first inserted into the femoral vein well below the inguinal ligament using the femoral artery pulse as a landmark to identify blood back-flush from the femoral vein using a saline-loaded syringe. An approximately 1-cm horizontal incision is made at the insertion site to widen the cutaneous opening and facilitate subsequent operations. Then, a 14-gauge peel away-introducer needle is inserted with a subcutaneous trajectory from the initial puncture point until it passes through the incision previously made to the final exit point. The final exit point is generally located on the abdomen at umbilicus level (Fig. 1, part 1). The inner needle of the introducer is removed (Fig. 1, part 2), and a catheter is threaded through the sheath in the opposite direction (from the final exit point to the incision) (Fig. 1, part 3). The sheath is withdrawn. The tunneled catheter is thereby created (Fig. 1, part 4). This tunneling technique can be repeated to prolong catheter use. Another 14-gauge peel-away introducer needle is passed through the skin at the first insertion site into the femoral vein (Fig. 1, part 5). After puncture, the inner needle is removed, and the catheter that previously created the subcutaneous tunnel is inserted into the vein (Fig. 1, part 6). The introducer is then peeled away (Fig. 1, part 7). The catheter is fixed and secured at the cutaneous exit point, and the incision is sutured closed (Fig. 1, part 8).
Abdominal radiography is performed to ensure correct placement of the catheter tip in the inferior vena cava. Nurses perform dressing changes.
Results
Our palliative care unit admitted 648 terminal patients during the study period. Among them, 87 (13%) underwent CVC insertion, while 11 (1.7%) with contraindicated subclavian or jugular access routes or PICCs underwent FTC insertion. Patient characteristics and FTC outcomes are shown in Table 1. Mean age was 69±12 (median, 68; range, 38–86) years. Mean ECOG performance status was 3.3±0.8 (median, 3; range, 2–4).
PS, Eastern Cooperative Oncology Group (ECOG) performance status; CVC, central venous catheter; TPN, total parenteral nutrition; SVC, superior vena cava.
FTC was successful and femoral vein cannulation was performed on the right side in all patients. Local anesthesia alone was used in nine cases, local anesthesia with endovenous sedation in two. An incidental femoral artery puncture occurred in one case, but was arrested by 10-minute compression against the pelvic bone. Superficial subcutaneous hematoma was not observed at the insertion site.
Total FTC placement was 207 days; the mean period in place was 19±15 (median, 17; range, 4–48) days. Eight patients received parenteral opioids via FTCs, high-dose (defined as an infusion rate exceeding 1 mL/h) in four cases, i.e., morphine hydrochloride and compound oxycodone injection (Pavinal) containing a small amount of hydrocotarnine in two each.
Catheter removal occurred in 2 of the 11 cases. One underwent central venous access from the subclavian vein because respiratory status improved, the other discontinued catheter use due to appetite improvement (cessation of parenteral nutrition) and discharge from the palliative care unit. The remaining 9 catheters functioned and remained in place until the patients died. These events were always related to disease progression, never to vascular access complications.
One patient had a poor infusion rate due to hip joint bending. No complications, e.g., catheter-related infection, venous thrombosis and catheter migration, were observed.
Discussion
This is, to our knowledge, the first descriptive study of FTC in a palliative care setting. FTCs were successfully inserted in terminally ill patients with cancer at the bedside, with a low complication rate.
One of the most important findings was that the femoral route is the main alternative when the SVC is unsuitable for CVC insertion in terminally ill patients with cancer, but this situation is uncommon. This catheter may be indicated in patients requiring high-dose opioid administration.
Another important finding was the high success rate without serious complications. The reported femoral catheter success rate in patients with cancer approaches 100%.12–15 The femoral site has anatomic advantages for percutaneous catheter introduction. The femoral pulse provides an easy landmark for vein localization. The insertion of a needle under ultrasound guidance also ensures secure access to the femoral vein and avoidance of arterial puncture. However, even if the artery is accidentally punctured, this complication can easily be managed by direct compression. In addition, there is no risk of fatal procedure-related complications such as pneumothorax, the major complication of subclavian and jugular access. PICC is also safe, but the reported success rate in the palliative care setting is 86%, 8 lower than with than femoral access.
Major problems with femoral access include catheter-related infections. However, a previous randomized clinical trial showed that in critically ill patients, FTC is associated with a fourfold reduction in systemic catheter-related sepsis risk. 16 For short-term catheter placement, the skin is the main source of catheter colonization and catheter-related sepsis. 17 Therefore, methods diminishing intercutaneous migration of organisms, such as tunnelization, may also decrease the risk of catheter-related infections.
Catheterization of the femoral vein is associated with more frequent venous thrombosis than other sites in critically ill adults.18,19 In this series, there were no signs of femoral thrombosis such as edema, pain, erythrocyanosis and collateral circulation in the limb. However, the clinical definitions used herein may have largely underestimated deep venous thrombosis incidence. Accurate evaluation of venous thrombosis requires ultrasound examination of the femoral vein. Based on this, prospective studies involving sufficient numbers of terminally ill patients with cancer are needed to compare thromboembolic events associated with femoral access. This was a retrospective chart review, with objective data collection. Therefore, we evaluated neither patient's subjective comfort and convenience, nor procedure-related distress. Future studies should focus on patient-perceived usefulness.
In conclusion, FTC might be an acceptable and simple alternative in selected terminally ill patients with cancer (i.e., those needing high-dose parenteral opioids), when subclavian or jugular access and PICC are difficult or contraindicated, a clinical situation seen in 13% of our series undergoing CVC.
Footnotes
Author Disclosure Statement
None of the authors has any conflicts of interest, financial or otherwise, to declare.