
Abstract
Abstract
Background:
In Japan, a nationwide palliative care education program for primary palliative care (the Palliative care Emphasis program on symptom management and Assessment for Continuous medical Education: PEACE) was established in 2008. Effective delivery of such programs relies on adequate evaluations of program efficacy; however, such an instrument does not exist.
Objective:
This study aimed to develop and validate a measurement tool to quantify knowledge level of physicians about broader areas of palliative care, by which the effect of an education program could be measured.
Methods:
We conducted a cross-sectional, anonymous, self-administered questionnaire survey with a group of 801 conveniently sampled physicians in October 2010. To examine the test-retest reliability of items and domains, the questionnaire was reissued two weeks after the first survey was completed. This study used psychometric methods, including item response theory, intraclass correlation coefficients, and known-group validity.
Results:
The response rate was 54% (n=434). We included 33 items across the following 9 domains: (1) philosophy of palliative care, (2) cancer pain, (3) side effects of opioids, (4) dyspnea, (5) nausea and vomiting, (6) psychological distress, (7) delirium, (8) communication regarding palliative care, and (9) community-based palliative care. For these items, the intraclass correlation was 0.84 and the Kuder-Richardson Formula 20 (KR-20) test of internal consistency was 0.87. There was a significant difference in the scores between palliative care specialists and other physicians.
Conclusions:
We successfully validated a newly developed palliative care knowledge questionnaire to evaluate PEACE effectiveness (PEACE-Q). The PEACE-Q could be useful for evaluating both palliative care knowledge among physicians and education programs in primary palliative care.
Introduction
Recently, several countries established nationwide palliative care education programs.3,4 In the United States, the Education for Physicians in End-of-life Care (EPEC™) Project 3 aimed to increase physician knowledge about palliative care, with 62% of the participants attaining improved knowledge. In Japan, the Palliative care Emphasis program on symptom management and Assessment for Continuous medical Education (PEACE) was established in 2008,2,5 with more than 1000 PEACE education opportunities and more than 20,000 participating physicians reported throughout Japan from 2008 to 2010. 6 To sustain the efficacy and significance of such programs, timely adjustment based on adequate and ongoing evaluations of the program is essential. Such evaluations should assess participant achievement and the effectiveness of the program among participants.
To date, the palliative care knowledge test (PCKT) was developed to measure the levels of knowledge about palliative care. 7 The PCKT consists of five domains: philosophy, pain, dyspnea, psychiatric symptoms, and gastrointestinal symptoms. However, the PCKT was originally designed to quantify knowledge about palliative care among general health care professionals, especially nurses; and consequently, the reliability and validity of PCKT was not formally investigated in physicians. In addition, existing measurement tools to measure the knowledge of physicians in palliative care literature focus on pain management, and no instruments have been established to measure knowledge level of physicians about broader areas of palliative care.8–10
The primary aim of this study was to develop and validate a measurement tool to quantify knowledge level of physicians about broader areas of palliative care, by which the effect of education programs could be measured.
Methods
We conducted a confidential and anonymous questionnaire survey among physicians, consisting of two phases: (1) instrument development and (2) psychometric analysis and selection of the 33 items for the final instrument. The ethical and scientific validity of this study was approved by the institutional review board of Saku Central Hospital. Consent to participate was indicated by the completion and return of the questionnaire.
Development phase
Initially, 12 palliative care specialists generated a total of 83 items for an item pool based on all modules of the PEACE program. Each such module includes nine domains and thus we designed our measurement instrument to include all these domains: (1) concept and philosophy of palliative care, (2) cancer pain, (3) side effects of opioids, (4) dyspnea, (5) nausea and vomiting, (6) psychological distress, (7) delirium, (8) communication, and (9) community-based palliative care.
To confirm the content validity, we adopted a modified Delphi method 11 with another group of 10 physicians (9 palliative care specialists and 1 psychiatrist). The experts evaluated the appropriateness of each item according to nine grades from 1 (inappropriate) to 9 (appropriate). If a participant rated the grade as less than 6, we asked him or her the reason. Items rated by eight or more members at 7 or more were selected; the remaining items were modified according to the members' opinions and then reevaluated. Following two such content-setting rounds we generated a provisional version of the instrument, the 79-item PEACE-Q (palliative care knowledge questionnaire for PEACE). Each question requires potential responses of right, wrong, and unsure.
Validation phase
The survey was carried out in October 2010 on 735 physicians from 15 conveniently sampled hospitals. The inclusion criterion was registered physicians whose specialty was not palliative medicine. In addition, to explore the known-group validity, 66 palliative care specialists were recruited. For this study, “palliative care specialist” was defined as a responsible physician in a certified palliative care unit belonging to Hospice Palliative Care Japan.
Procedures
The questionnaire with an accompanying cover letter was distributed to physicians by mail. Completed questionnaires were collected in a box specifically provided in each participating hospital. The survey for test-retest examination was conducted on the subjects who had consented to participate during the first survey in three institutions with two-week interval administrations. For the 79-item PEACE-Q, we then analyzed and compared physician backgrounds—i.e., age, gender, specialty, institutions, years of clinical experience, the number of terminally ill cancer patients seen in the past year, the number of cancer deaths per year, the number of patients they prescribed opioids to in the past year, and whether they participated in a PEACE program. No reminder or reward was used.
Statistical analysis and item selection
For analyses, ‘unsure’ responses were regarded as incorrect. First, to assess feasibility we calculated the percentage of missing data for each question; if the missing value accounted for more than 1% of all data, that item was regarded as inappropriate. Next, to assess sensitivity we calculated the percentage of correct answers for each question; if correct answers accounted for more than 90% of all data, that item was regarded as inappropriate. Third, to examine the test-retest reliability of each item, the kappa coefficients were calculated (cutoff: kappa coefficient of 0.3). Fourth, we estimated the difficulty and discrimination based on the two-parameter logistic Item Response Theory (IRT) model. IRT models are used for the statistical estimation of parameters that represent the magnitude of a latent trait attributable to the items. An advantage of IRT is that it potentially enables a researcher to improve the precision and reliability of an assessment. 12 We then determined the precision (cutoff: discrimination of 0.5). Finally, to confirm the content validity, the first 12 experts discussed the appropriateness of each item from both statistical and clinical viewpoints: (1) items in which sensitivity was likely to be higher and (2) items that could be viewed as providing lessons. Through this process, 33 items were selected to comprise the PEACE-Q.
Reliability and validity
Internal consistency was determined by calculating the Kuder-Richardson Formula 20 (KR-20) index. The test-retest reliability was explored by calculating intraclass correlation coefficients. To explore known-group validity, the unpaired t-test was used to determine a potential statistically significant difference in the total score of the PEACE-Q (33 items) and for each domain, between the palliative care specialists and the other physicians.
Statistical analysis was performed using statistical software SAS (SAS version 9.1; SAS Institute Inc., Cary, NC). The significance level was set at P<0.05 (two-tailed).
Results
Among 801 physicians included in the validation study, 434 responses (54%) were obtained and analyzed. For the test-retest investigation, 124 physicians agreed to participate and a total of 44 responses (35%) were obtained and analyzed.
The subject characteristics are summarized in Table 1. Approximately 70% were male, with an average of 16 years of clinical experience. Among them, 51% experienced more than 21 terminally ill cancer patients in the past year, while 17% cared for less than 5 cancer patients.
The percentages do not add up to 100% due to missing values.
Item selection
Missing values totaled more than 1% in three items (1.2% each). However, we gave priority to content validity over psychometric properties based on the discussion among experts; thus, these three items were included in the PEACE-Q.
The percentage of correct answers ranged from 19% to 99% across the items, with the highest percentage of correct answers (99%) for, ‘Oral care should not be offered to the patients with nausea and vomiting, because mouth stimulation causes vomiting.’ Eighteen items showed a correct response rate of 90% or more, and these items were excluded. There were no items with 10% or less correct response rate.
The kappa coefficient in the test-retest reliability of each item ranged from −0.04 to 0.85, and was 0.3 or less for 14 items. However, we gave priority to content validity over psychometric properties based on the discussion among experts, and 6 out of these 14 items were included.
The results of the item analysis and IRT are shown in Table 2. The difficulty in all items ranged from −2.76 to 0.29, with a discrimination of 0.69 to 2.67. We determined that a subject who correctly answered an item with high discrimination would also have a high total score, whereas for an item with poor discrimination, the percentage of correct answers for that item would not relate to the total score.
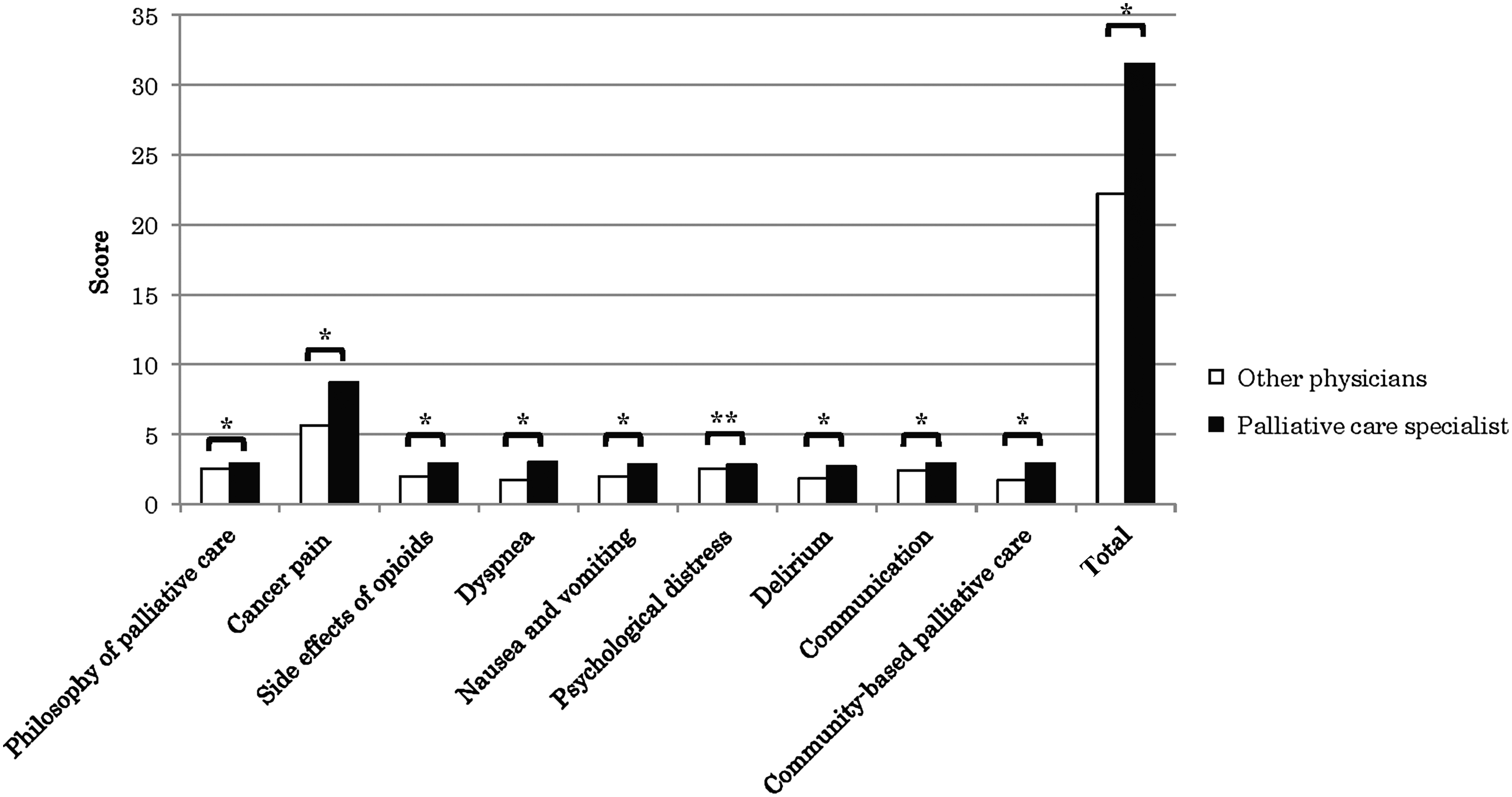
Based on the item analysis, IRT, and expert discussions, we determined 33 items for inclusion in the final version of PEACE-Q across the following 9 domains: (1) philosophy of palliative care, (2) cancer pain, (3) side effects of opioids, (4) dyspnea, (5) nausea and vomiting, (6) psychological distress, (7) delirium, (8) communication, and (9) community-based palliative care.
Reliability and validity
The KR-20 index of internal consistency was 0.87, and the intraclass correlation in the test-retest examination was 0.84. Regarding the known-group validity, there was a significant difference in the score for each domain as well as in the total score between palliative care specialists and other physicians (see Figure 1).
PEACE, Palliative care emphasis program on symptom management and assessment for continuous medical education.
Discussion
This study validated an instrument to measure the levels of knowledge about palliative care among physicians. This measurement tool enables us to evaluate the ongoing effectiveness of the PEACE program. The instrument showed good internal consistency, test-retest reliability, and known-group validity.
PEACE-Q would be useful for measuring the level of palliative care knowledge that all physicians engaged in cancer treatment should have. Furthermore, it could be used to measure the efficacy of undergraduate education programs about palliative care.
Previous measurement tools for quantifying the effect of palliative care education programs for physicians showed insufficient evaluation of reliability and validity,13–16 and none other than the PCKT addresses a broad knowledge of palliative care. 7 However, the psychometric properties of the PCKT were formally evaluated only among nurses. The PEACE-Q is a specific measure for physicians in both patient care and symptom management.
This study has several limitations. The tool was developed only for physicians who attend a PEACE-based seminar. In addition, several questions (2, 3, 31, 32, 33) are specifically about the Japanese medical system, and thus are not suitable for physicians in other countries; this limits the instrument transferability.
In conclusion, this study used psychometric methods to validate an instrument for evaluating palliative care knowledge among physicians who attend a PEACE-based seminar, which was developed as a nationwide education program in palliative care. This evaluation instrument was constructed to cover nine domains: philosophy of palliative care, cancer pain, side effects of opioids, dyspnea, nausea and vomiting, psychological distress, delirium, communication, and community-based palliative care. The PEACE-Q could be useful for evaluating both knowledge among physicians and education programs in primary palliative care.
Footnotes
Acknowledgments
The authors acknowledge financial support for the research, authorship, and/or publication of this article from a Health and Labor Sciences Research Grant for Clinical Cancer Research.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.