
Abstract
Abstract
Background:
Health care providers' lack of education on spiritual care is a significant barrier to the integration of spiritual care into health care services.
Objective:
The study objective was to describe the training program, Clinical Pastoral Education for Healthcare Providers (CPE-HP) and evaluate its impact on providers' spiritual care skills.
Methods:
Fifty CPE-HP participants completed self-report surveys at baseline and posttraining measuring frequency of and confidence in providing religious/spiritual (R/S) care. Four domains were assessed: (1) ability and (2) frequency of R/S care provision; (3) comfort using religious language; and (4) confidence in providing R/S care.
Results:
At baseline, participants rated their ability to provide R/S care and comfort with religious language as “fair.” In the previous two weeks, they reported approximately two R/S patient conversations, initiated R/S conversations less than twice, and prayed with patients less than once. Posttraining participants' reported ability to provide spiritual care increased by 33% (p<0.001). Their comfort using religious language improved by 29% (p<0.001), and frequency of R/S care increased 75% (p<0.001). Participants reported having 61% more (p<0.001) R/S conversations and more frequent prayer with patients (95% increase; p<0.001). Confidence in providing spiritual care improved by 36% overall, by 20% (p<0.001) with religiously concordant patients, and by 43% (p<0.001) with religiously discordant patients.
Conclusions:
This study suggests that CPE-HP is an effective approach for training health care providers in spiritual care. Dissemination of this training may improve integration of spiritual care into health care, thereby strengthening comprehensive patient-centered care.
Introduction
R
Spiritual support is related to greater patient well-being, happiness, hope, optimism, and gratefulness. 18 Spiritual well-being protects against despair at the end of life, 19 leads to avoidance of burdensome treatment and improved quality of life, 20 increases hospice enrollment, 21 and promotes feeling at peace. 22 Spiritual care benefits patients emotionally and can strengthen patient-provider relationships. 23 Consistent with these findings, studies suggest that patients want to be asked about R/S beliefs, particularly in times of serious and life-threatening illness, 24 medical decision making, 25 and loss of a loved one. 26 However, many providers continue to overlook patients' R/S values, 27 and many patients with advanced life-threatening disease feel their spiritual needs are not addressed by their medical team or in their R/S communities.10,28
Lack of health care providers' education about R/S issues is one barrier to improved integration of spiritual care in health care.29,30 Therefore, we hypothesized that comprehensive education in integrating R/S care into medical practice may overcome these barriers.
This paper describes a five-month program that offers one model of educating health care providers about R/S care, and evaluates the frequency of and confidence in providers' provision of spiritual care following training as primary outcome measures.
Methods
Clinical pastoral education program
Clinical Pastoral Education for Healthcare Providers (CPE-HP) is a five-month fellowship in spiritual care, 31 taught by a nationally certified instructor. This clinical pastoral education program is accredited by the Association for Clinical Pastoral Education, Inc. It is offered through the Chaplaincy Department at the Massachusetts General Hospital, and supported through the Schwartz Center for Compassionate Healthcare, www.theschwartzcenter.org. The program is open to health care professionals with direct patient interaction and under employment with any institution. Applicants must demonstrate openness to diverse R/S affiliations in a pluralistic hospital and educational setting.
CPE-HP aims to teach integration of R/S care into clinical practice. Graduates are expected to conduct basic spiritual assessments, inquire about R/S issues impacting care, offer appropriate prayer, and refer to a board-certified chaplain as needed. CPE-HP offers process-oriented and relationship-centered adult experiential education, based in theology, psychology, group and educational theory.
Participants learn to assess and use patients' own R/S beliefs to enhance positive coping. They learn to initiate and end meaningful helping relationships and utilize diverse religious resources related to health, illness, and dying. CPE-HP trains participants to use similarities in different R/S beliefs to effectively navigate diversity. The diverse and interdisciplinary participant group becomes a laboratory for skill development for improving listening skills, reading nonverbal cues, assessing underlying motivations, using appropriate self-disclosure, and balancing interpersonal boundaries with empathy.
CPE-HP includes an educational and a clinical component. The educational component consists of 100 hours parceled into eight-hour days, including didactic presentations, case presentations, leadership in interfaith services, and a process group. Didactics focus on literacy in diverse R/S paths, spiritual assessment, and spiritual care skills. Case presentations assess how interventions address patients' R/S needs. During the 300-hour clinical component, participants function in their professional home setting in their primary provider role, enhancing application of competencies. Participants assume the role of a spiritual care provider based on patients' expressed needs, disease progression, and on participants' perceived opportunities and increased abilities in the clinical context. CPE-HP does not lead to participants' certification in chaplaincy. Rather, posttraining participants continue to provide medical care and, where appropriate, integrate spiritual care. Participants receive biweekly supervision from the instructor focusing on individual challenges to spiritual care in each participant's clinical setting.
Written assignments include weekly reflection notes in which participants reflect on their learning experiences; case presentations; and papers on participants' R/S experiences related to topics including illness, death, suffering, and hope. Participants also describe changes in their attitudes, knowledge, behaviors, integration of R/S care into clinical practice, and plans for further provision of R/S care in their clinical context.
Study participants
Between 2003 and 2009, all participants (n=55) completed a questionnaire at the program's beginning and end. Institutional review board approval was obtained to examine these assessments retrospectively. To focus this study on the efficacy of the program for nonchaplain clinicians, chaplains were eliminated from the analysis, leaving a final sample size of 50. Participants reported their age; gender; education level; occupation; number of years of experience in their professional field; religious affiliation; and number of patients cared for weekly with acute, chronic, and life-threatening illness.
Measures
Validated measures of spiritual care training effectiveness have not been developed. Measures were created to assess four R/S care concepts targeted by the training program.
Ability to provide R/S care
Participants' ability to provide R/S 37 care was measured with a self-report measure assessing participants' ability to (1) identify R/S issues with patients and families; (2) initiate conversations about R/S issues with patients; (3) respond to R/S issues initiated by patients; and (4) make and follow through with spiritual assessments and care plans. Each of these items was rated on a five-point scale (1=no ability, 5=excellent). Participants' responses were averaged to create a total score (Time 1 Cronbach's alpha=0.78).
Frequency of R/S care
Participants reported the frequency with which they offered R/S care over the past two weeks, including R/S conversations with patients and families, initiation of R/S conversations with patients, and frequency of praying with patients. Each item was rated on a five-point scale (1=zero times, 5=four or more times). Participants' responses were averaged to create a total score (Time 1 Cronbach's alpha=0.86).
Comfort using religious language
Participants' comfort using religious language was assessed with a single item, “I am comfortable using religious language with patients,” based on a five-point scale from 1 (strongly disagree) to 5 (strongly agree).
Confidence in R/S care
Finally, participants rated their confidence in providing R/S care to Buddhist, Hindu, Jewish, Protestant, and Roman Catholic patients (e.g., “I feel confident providing care to Buddhist patients”) on a five-point scale from 1 (strongly disagree) to 5 (strongly agree). Participants' responses were scored in three ways. First, a measure of overall confidence in providing R/S care was created by averaging participants' scores on each item (Cronbach's alpha=0.87). Second, a measure of participants' confidence in providing care to patients of the same religion as the participant (religious concordance) was created by matching the participant's affiliation with the religious affiliation assessed in the item. Finally, a measure of confidence in providing care to patients of different religions (religious discordance) was created by averaging participants' responses to items assessing confidence in providing care for patients of religions different from the participant's.
Statistical analysis
Descriptive statistics were employed to describe the sample. To identify confounding variables, we examined the relationships between (1) sample characteristics (gender; education; occupation; number of years in current occupation; religious affiliation; age; number of patients seen weekly with acute, chronic, and life-threatening illnesses); (2) change in R/S care over time; and (3) confidence in providing R/S care from baseline to post CPE-HP training, using t-tests and one-way ANOVAs for categorical variables, and Pearson correlation coefficients for continuous variables. Sample characteristics significantly (p≤0.05) associated with outcome variables were controlled for in subsequent analyses of those outcome variables. Analyses to identify confounding variables were not conducted for outcomes within each religious affiliation due to small sample sizes. Analyses conducted within each religion should be considered exploratory.
Repeated-measures ANOVAs were used to examine change from baseline to post CPE-HP in participants' ability to provide R/S care and frequency of R/S care provision. Repeated-measures ANOVAs were also used to examine change in participants' confidence in their ability to provide R/S care from baseline to post CPE-HP. These analyses were conducted on participants' overall confidence and confidence in providing care to patients of concordant (same) and discordant (different) religion relative to the participant. Finally, repeated-measures ANOVAs were used to compare participants' relative confidence in providing care to patients of concordant versus discordant religion (concordant confidence minus discordant confidence) at each time point and to examine whether this relative confidence changed from baseline to post CPE-HP. All analyses were two-sided, using p≤0.05 as threshold for statistical significance and were performed with SPSS 20.0 (IBM, New York, NY).
Results
Sample characteristics
Demographics and professional experience of the sample are shown in Table 1. Participants were primarily female (82%) with a mean age of 47.1 years (SD=10.78). The sample was primarily Christian, with 40% Protestant and 20% Roman Catholic. A minority of participants were Jewish (16%) and of other (18%) traditions.
Sample size ranges from 39 to 50 due to missing data.
Spiritual care provision at baseline
At baseline, participants rated their ability for R/S care provision as “fair” (M=3.14, SD=0.59) and reported a fair degree of comfort using religious language (M=3.21, SD=0.92). Participants reported having R/S conversations with patients approximately twice in the two weeks (M=2.13, SD=1.59) and initiating R/S conversations less than twice in the past two weeks (M=1.80, SD=1.60). Participants reported praying with patients less than once in the past two weeks (M=0.76, SD=1.20).
Change in spiritual care provision from baseline to posttraining
Younger age (p=0.02) and fewer years in the current occupation (p<0.05) were associated with greater increase in self-reported ability to provide R/S care over time. Participants with≤12 years of education reported a larger increase over time in the frequency of initiating R/S conversations than participants with higher education levels (p=0.02). These sample characteristics were controlled for in subsequent analyses. No other significant relationships between sample characteristics and change in R/S care emerged.
Participants reported improvements from baseline to posttraining in ability to provide spiritual care (p<.001, 33% increase; see Table 2) and comfort using religious language (29% increase, p<.001). Additionally, participants reported increased frequency of R/S care provision from baseline to posttraining (75% increase, p<0.001). Examination of the frequency of specific types of R/S care indicated increase in frequency of R/S conversations with patients (61% increase, p<0.001); initiation of R/S conversations (83% increase, p<0.001); and praying with patients (95% increase, p<0.001) over time.
p≤0.05 considered significant.
R/S ability items include ability to identify R/S issues with patients and families; ability to initiate conversations about R/S issues with patients; ability to respond to R/S issues initiated by patients; ability to make and follow through with spiritual assessments and care plans. Repeated measures ANOVA adjusted for age and number of years in current occupation.
Frequency of R/S care items include frequency of R/S conversations; frequency of initiating R/S conversations; frequency of prayer with patient.
Repeated measures ANOVA adjusted for education level.
R/S, religious/spiritual.
Confidence in providing spiritual care
Change in confidence in providing R/S care overall (p<0.05) and to patients from different religious affiliations (p<0.05) from baseline to posttraining differed by religion, with Jewish participants reporting greater change than Roman Catholic participants. Additionally, participants' relative confidence in providing R/S care to religiously concordant versus religiously discordant patients at baseline differed by participants' religion (p<0.05), although post hoc analyses of group differences were not significant. Change in participants' relative confidence in providing R/S care for patients of the same versus a different religion also differed by religion of participants (p<0.05) and gender (p<0.05). Participants identifying with “other” religion reported greater change in relative confidence from baseline to posttraining compared to Protestant participants, and women reported greater change than men. These sample characteristics were controlled for in subsequent analyses.
Participants' confidence in providing spiritual care improved from baseline to posttraining (36% increase, p<0.001; see Table 3 and Fig. 1). This change was then examined for provision of R/S care to patients with the same (religiously concordant) and different (religiously discordant) religions. Participants' confidence in their ability to provide R/S care to religiously concordant (20% increase, p<0.001) and religiously discordant patients (43% increase, p<0.001) significantly improved.
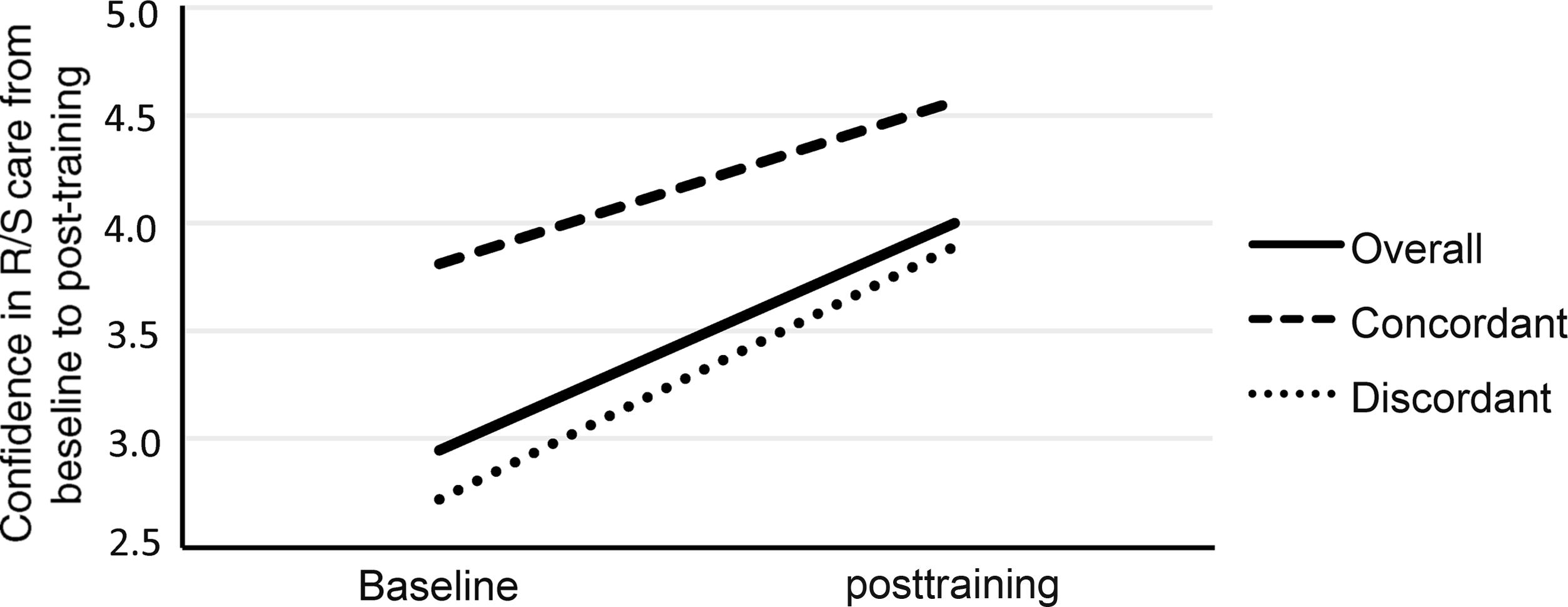
Confidence in providing spiritual care for the total sample. (Sample size varies due to missing data. Overall n=44; concordant n=36; discordant n=35.)
p≤0.05 considered significant.
Confidence range measured on a scale from 1 to 5.
Repeated measures ANOVA adjusted for participant religious affiliation.
Change in confidence was also examined by participants' religion (see Table 3). Jewish participants reported an increase in confidence in providing R/S care over time (40% increase, p=0.001). Jewish participants also reported an improvement in confidence in providing R/S care to Jewish patients (32% increase, p=0.002) and non-Jewish patients (77% increase, p=0.001). Similarly, Protestant participants reported increased confidence in ability to provide R/S care overall (40% increase, p<0.001) and to Protestant (18% increase, p=0.001) and non-Protestant patients (48% increase, p<0.001). While Roman Catholic participants reported an increase in confidence over time (15% increase, p<0.05), the change was not significant when examined for religiously concordant (9% increase, p=0.20) and religiously discordant patients (15% increase, p=0.07).
Change in confidence over time was examined in participants who self-identified as “other” in religious tradition. These participants reported an increase in overall confidence in providing R/S care from baseline to posttraining (28% increase, p=0.005). They also reported improved confidence in providing spiritual care to Jewish (31% increase, p=0.009); Roman Catholic (15% increase, p=0.04); Protestant (27% increase, p=0.009); and Buddhist patients (32% increase, p=0.04). Participants' confidence in their ability to provide care to Hindu patients did not significantly improve over time (40% increase, p=0.07).
Lastly, we examined participants' relative confidence in providing R/S care to patients of the same and different religion, and change in this relative confidence over time. Participants across religious affiliations reported greater confidence in ability to provide R/S care to patients of the same versus a different religious affiliation at baseline (p<0.001; see Table 4) and posttraining (p<0.001). The difference in participants' confidence in providing care to religiously concordant versus religiously discordant patients decreased over time but this change was not significant (p=0.46).
p≤0.05 considered significant.
Mean is average difference in confidence in providing care to patients of the same versus a different religious affiliation [average: (religious concordance – religious discordance)]. These ANOVAs compare the average concordant confidence to average discordant confidence.
Repeated measures ANOVA adjusted for participant religious affiliation.
Mean is average change in difference in confidence providing care to patients of the same versus a different religious affiliation across time [(baseline religious concordance – baseline religious discordance) – (post religious concordance – post religious discordance)]. This ANOVA compares the average baseline difference in concordant and discordant confidence to the average posttraining difference in concordant and discordant confidence.
Repeated measures ANOVA adjusted for participant religious affiliation and gender.
Similarly, Jewish participants reported greater confidence in ability to provide R/S care to Jewish versus non-Jewish patients at baseline (p=0.001) and posttraining (p=0.001). Additionally, the difference in Jewish participants' confidence in providing care to religiously concordant versus religiously discordant patients significantly decreased over time (41% decrease, p=0.035). Protestant participants also reported greater confidence providing care to religiously concordant versus discordant patients at baseline (p<0.001) and posttraining (p<0.001) and a reduction in this difference over time (48% decrease, p=0.003). Roman Catholic participants reported greater confidence in providing spiritual care to Roman Catholic versus other participants at baseline (p=0.022) and posttraining (p=0.005). However, the difference in confidence with religiously concordant versus religiously discordant patients did not change (3% decrease, p=0.74). These analyses were not conducted for participants self-identifying as “other” in religious tradition, because the survey did not assess confidence in providing care to patients of “other” religious traditions.
Discussion
Although spiritual care is an important component of high-quality health care, many patients report that their spiritual care needs are unmet. 10 Inadequate provider training is a significant barrier to integrating R/S in patient care. 3 Several educational models exist, 34 but little is known about their effectiveness. The number of medical schools offering courses in R/S topics grew from 3 to 75 of 125 between 1992 and 2001, with many of those courses required and integrated into the overall curriculum.35–38 This study assesses the impact of the CPE-HP program on participants' self-rated ability to provide R/S care, confidence in this ability, and frequency of R/S care provision. From baseline to posttraining, participants' self-reported ability and confidence improved. They also reported providing spiritual care more frequently posttraining.
Improvements in participants' confidence occurred whether the patient's religion was concordant or discordant from the providers for participants of Protestant, Jewish, and “other” religious affiliation. However, while Roman Catholic participants reported improvements in their confidence overall, changes by patient affiliation were not significant. This difference may be due to Roman Catholic participants reporting higher baseline confidence, leaving less room for improvement; and/or it may be due to the small sample size rendering differences difficult to detect. Thus, CPE-HP improves participants' confidence in providing spiritual care for most participants independent of patient affiliation.
The program addresses a barrier to provision of R/S care by providing knowledge regarding a variety of religions. It teaches participants to bridge the gap between patients' and their own religion, suggesting an improved ability to relate across belief systems. Many disciplines participate in CPE-HP, mirroring the multidisciplinary medical team. The program's focus on integration of R/S concerns into patient care in participants' regular work setting appears effective.
Study limitations include utilization of self-reported measures that may be influenced by social desirability bias. Furthermore, participants in CPE-HP or any other elective R/S care education are self-selected, interested, and committed to R/S care. Observational measures of the frequency of participants' R/S care provision would address self-report bias. Assessment of the relative efficacy of the educational and clinical components will inform program modifications. Longitudinal participant assessment beyond posttraining measures will determine lasting training impact.
Conclusions
Participants' self-reported ability and confidence with providing spiritual care, comfort using religious language, and frequency of R/S care increased over the course of CPE-HP. These results suggest that CPE-HP is an effective program for improving health care providers' ability to integrate spiritual care into patient care. Patient care standards and guidelines call for addressing patients' spirituality; CPE-HP represents a promising model for training providers to meet these standards that warrants additional investigation.
Footnotes
Acknowledgments
The authors wish to thank Sr. Sheila Hammond for her contribution to the development of the Clinical Pastoral Education program at Massachusetts General Hospital.
Author Disclosure Statement
No competing financial interests exist.