
Abstract
Abstract
Purpose:
To clarify the family-perceived necessity of improvement in death pronouncement and explore the potential association between behaviors of physicians and the family-perceived necessity of improvement.
Subjects and Methods:
A questionnaire survey was conducted involving 226 bereaved family members of patients who had died at home while receiving hospice service. A total of 91 responses were analyzed (response rate, 47%).
Results:
All pronouncements were performed by physicians. A total of 89% (n = 81, 95% confidence interval, 81%–94%) of family members reported that they felt no necessity of improvement at all or that almost no improvement was needed. Behaviors of physicians significantly positively correlated with the family-perceived necessity of improvement were that physicians acted calmly, and were not rushed. Those negatively associated were that physicians did not verify the time of death clearly, left the patient's clothes disheveled, and touched the family members' backs or shoulders as an expression of empathy. More than 90% of family members recommended that physicians act calmly, have a suitable appearance for the situation, introduce themselves to family members, explain the cause of death explicitly, and conduct a check using a light and stethoscope for death pronouncement.
Conclusion:
Most of the family members who had experienced a patient's death at home were satisfied with the death pronouncement. Several factors were associated with family satisfaction, and further large studies are needed to confirm the results.
Introduction
T
The primary aims of this preliminary study were to: (1) clarify the family-perceived necessity of improvement in death pronouncement and (2) explore the potential association between behaviors of physicians and the family-perceived necessity of improvement. An additional aim was to clarify recommendations from the families about death pronouncement.
Method
We mailed the questionnaires to the bereaved families in April 2014. If the families did not want to participate, they were requested to return the questionnaire by checking the “no participation” box. The return of all other completed questionnaires was regarded as consent to participate. Ethical and scientific validity was confirmed after the Institutional Review Board of Seirei Mikatahara Hospital.
Subjects
Inclusion criteria for this study were a bereaved adult family member of an adult patient who had died at home while receiving hospice service provided by the Mirai Home Clinic from November 2011 to November 2013 (one family member was selected for each patient). Exclusion criteria were family member unavailable, inability to complete the questionnaire, and serious psychological distress, as recognized by the primarily responsible home care physicians. The last criterion, which was adopted in the same way as in previous surveys,17–19 was applied on the assumption that primarily responsible physicians could identify families who may suffer serious psychological distress resulting from this survey.
Questionnaire
A questionnaire was developed for this study based on a systematic literature review and discussions among the researchers.4–14 In Japan, because all death pronouncements are performed by physicians, questions focused on physicians' attitudes.
The primary end point was the family-perceived necessity of improvement in death pronouncement. We asked the following question: ‘‘How much improvement do you think is necessary in death pronouncement by the physician?’’ The response was rated on a 6-point scale ranging from 1 (much improvement needed) to 6 (no improvement needed at all). This type of question was adopted in the previous surveys.17–19
To explore the factors that potentially contributed to a family-perceived necessity of improvement, we asked about the availability of physicians/nurses at the time of death and the behaviors of physicians. The former was evaluated based on three items: whether or not the physicians/nurses were present at the time of death, time to the arrival of physicians/nurses after the patient's death (<1 hour or ≥1 hour), and whether the death pronouncement was performed on that or the next day. The behaviors of physicians were conceptualized into three categories: general attitude of the physicians (Table 1); 2 items, evaluated by the level of agreement with a statement on a 6-point Likert-type scale from 1 [strongly disagree] to 6 [strongly agree]); physicians' practice of death pronouncement (8 items, evaluated with a yes/no format); and physicians' attention to family members (7 items, evaluated with a yes/no format).
Rated on a 6-point Likert-type scale. Classified into Yes (slightly agree, agree, and strongly agree) and No (slightly disagree, disagree, and strongly disagree).
SD, standard deviation.
In addition, we examined the level of recommendation from the family members about death pronouncement by physicians. We asked them the question: “How necessary do you think it is regarding the behaviors of physicians on death pronouncement?” in response to 14 items (Table 2). The responses were rated on a 5-point scale from 1 (not necessary at all) to 5 (essential). As background data, the family members reported the age, gender, and primary disease of the patient; age and gender of the family members; and their relationship with the patient.
Rated on a 5-point Likert-type scale from 1: not necessary at all to 5: essential. For this table, the numbers show the response of slightly necessary/necessary and essential respectively.
Statistical Analyses
We first calculated the distribution and 95% confidence interval for the primary end point, i.e., the family-perceived necessity of improvement in death pronouncement. We then compared the score for the family-perceived necessity of improvement between the group with and without each factor that potentially contributed to the family-perceived necessity of improvement. The responses to the question regarding the general atmosphere of the physician were classified into two groups: those who rated the level of their agreement as strongly agree, and agree or slightly agree versus others. The numbers of missing values in the questions about physicians' behaviors ranged from 7.7% to 29%. We decided to include all responses and calculate percentages using the number of the total sample as a denominator, because our primary intent was to compare the score of necessity for improvement between the group with or without each factor, and not to estimate the frequency of behaviors of physicians. In regard to recommendations from family members, the rates of those whose responses were essential, necessary, or slightly necessary were calculated.
Univariate analyses were performed using Student's t-test. All analyses were conducted using the Statistical Package for the Social Sciences, version 19.0 (SPSS Inc., Chicago, IL).
Results
Of the 226 family members considered as potential participants, 13 were excluded due to serious psychological distress recognized by physicians (n = 8), an inability to complete the questionnaire (n = 3), or the lack of available family members (n = 2). Of the 213 questionnaires sent, 18 were returned as undeliverable, with a total of 105 returned by the families (response rate, 54%). Of those, 6 refused to participate and 8 responses were excluded due to missing data on primary end points. Thus, 91 responses were finally analyzed (effective response rate, 46.7%; 91/195). Table 3 summarizes the backgrounds of patients and family members.
SD, standard deviation.
Family-perceived necessity of improvement in death pronouncement
In total, 89% (95% confidence intervals, 81%–94%, n = 81) of all family members reported that they felt no necessity of improvement at all or that almost no improvement was needed in death pronouncement by the physician (Fig. 1).
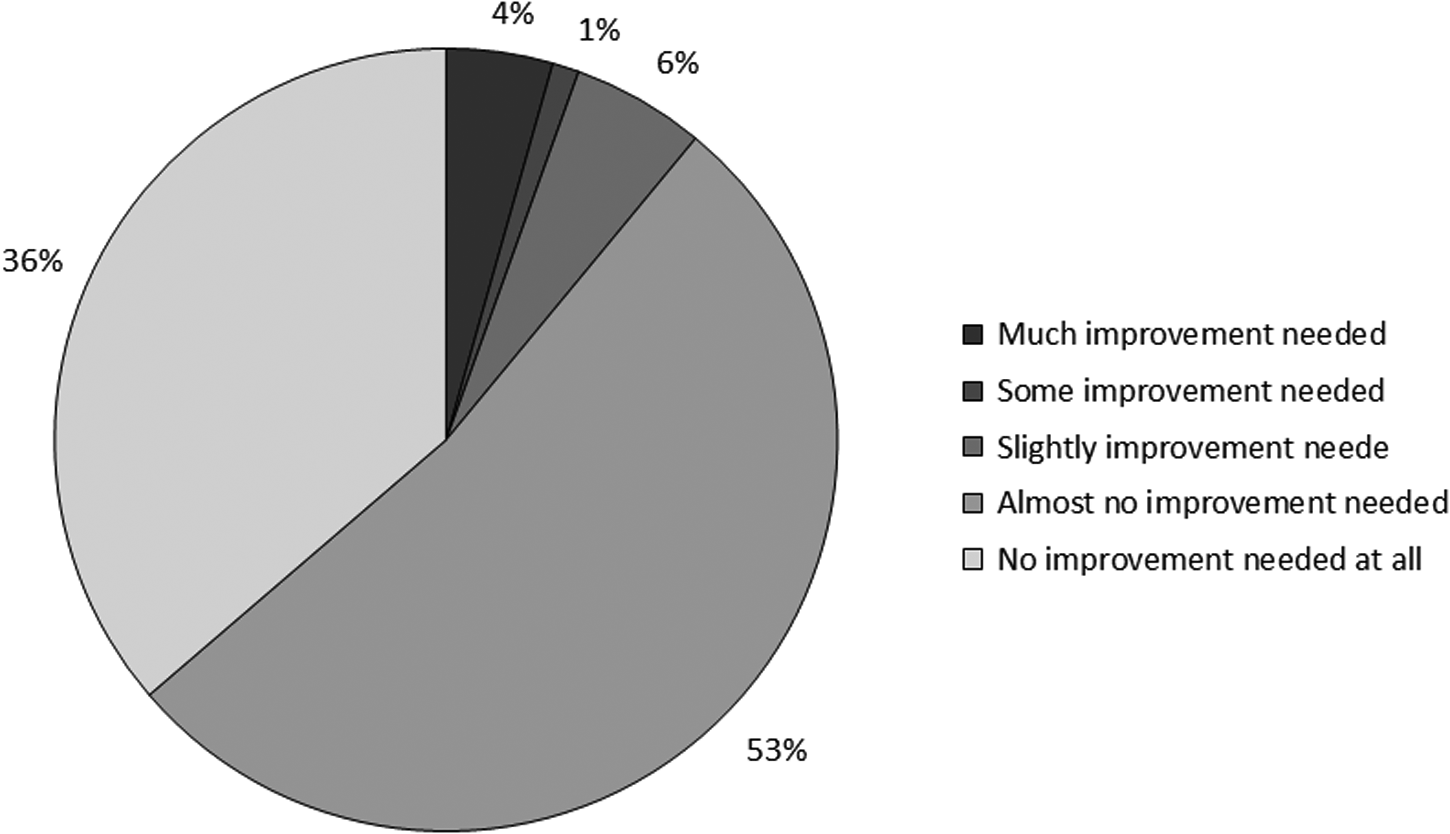
Primary end points: the family perceived necessity of improvement in death pronouncement.
Factors associated with family-perceived necessity of improvement
The family members who reported that a physician/nurse was present at the time of death were significantly more likely to feel a necessity for improvement (Table 4).
The scores for necessity of improvement are from 1 = much improvement needed to 6 = no improvement needed at all.
SD, standard deviation.
The family members who reported that the physician acted calmly were significantly less likely to feel a necessity for improvement (Table 1). Those who reported that the physician did not verify the time of death clearly, left the patient's clothes disheveled, and touched their backs or shoulders as an expression of empathy were significantly more likely to feel a necessity for improvement.
Recommendations from family members about death pronouncement
Table 2 shows that more than 90% of family members recommended that physicians act calmly, have a suitable appearance for the situation, introduce themselves to family members, explain the cause of death explicitly, and conduct a check using a light and stethoscope for death pronouncement.
Discussion
This study investigated the family-perceived necessity of improvement in death pronouncement in a Japanese home hospice.
The first important finding was that approximately 90% of family members were satisfied with the death pronouncement by the physician. Compared with a survey in an emergency department, this proportion was high. 9 In home hospice settings, patient deaths are generally expected, and recent studies revealed the good deaths of patients receiving home hospice care programs.17,20 In addition, because the deceased patients were elderly (mean age, 82) in this study, their deaths could have been acceptable for family members.21,22
The second important finding was the identification of the potential association between behaviors of physicians and family-perceived necessity of improvement in death pronouncement. The importance of acting calmly and verifying the time of death clearly is consistent with clinical recommendations.4,10–14,23 Our study provided empirical evidence to support these recommendations. Tidying the patient's clothes after examination is also important, because being respectful and dignified even after death is essential for the family. 24 In contrast, touching the family members was unfavorable in this study population. Generally, the Japanese prefer indirect communication, and an empirical study revealed that 58% of patients with cancer preferred not to be touched on hearing bad news. 25 Although the small sample size limits the generalizability, this suggests that physicians should express empathy in a culturally acceptable manner for each ethnic population.
This study had several limitations. First, the subjects of this study were limited to family members of patients who had died while receiving a single home hospice service. Second, there may have been recall bias. Third, the effective response rate was relatively low (47%). Finally, the findings of this study might not be generalizable for countries where not only physicians but also nurses perform death pronouncement.
In conclusion, most family members who experienced a patient's death at home were satisfied with the death pronouncement. Recommended behaviors of physicians on death pronouncement include: suitable atmosphere and appearance for the situation, self-introduction, examination to confirm death using a light/stethoscope, informing of the death and its cause explicitly, tidying the patient's clothes after examination, and expression of empathy in a culturally acceptable manner. A larger study in more variable settings is needed to confirm the results of this preliminary study.
Footnotes
Acknowledgments
This study was funded by the Yuumi Memorial Foundation for Home Health Care, and partially by the Sasakawa Memorial Health Foundation.
Author Disclosure Statement
No competing financial interests exist.