
Abstract
Abstract
Background:
An increasing proportion of hemodialysis patients are ineligible for transplant. Often these patients are elderly, with multiple comorbidities and decreased functional status. Such patients may benefit from modified treatment goals to reduce symptom burden.
Objective:
To demonstrate the feasibility of a trial of reduced-intensity treatment in nontransplantable patients with end-stage renal disease (ESRD).
Study Design:
A 6-week study randomized patients to a reduced-intensity intervention versus usual care. Intervention subjects were treated with liberalized goals for serum phosphorus and parathyroid hormone (PTH) as well as predialysis blood pressure in comparison with usual care subjects. Outcomes included assessed feasibility of recruitment, randomization, and data collection.
Setting and Population:
Sixteen transplant-ineligible hemodialysis patients were recruited from two urban units.
Measurements:
Blood pressure was recorded weekly, while serum PTH and phosphorus were assessed every 10 days. A quality-of-life measure was administered before and after the trial.
Results:
Of 300 patients, 51 were eligible and 16 consented. All were randomized and completed the trial. Patients in the intervention group received significantly lower doses of phosphorus binders and vitamin D analogues, and were less likely to have their dry weight reduced. All patient surveys were completed.
Conclusions:
High-risk hemodialysis patients may benefit from liberalized treatment guidelines but larger studies are necessary.
Introduction
T
Burdensome symptoms experienced by nontransplantable dialysis patients vary widely, but include significant rates of nausea, vomiting, dyspnea, and anxiety. 5 Moreover, these symptoms stem from multiple sources. Underlying comorbidities, residual uremia, 6 and the dialysis procedure itself 7 can contribute to decreased quality of life, and constitute complex problems that often elude simple solutions. Interventions used to treat the metabolic complications of ESRD can also contribute to patient symptom burden. The average dialysis patient takes nearly 20 pills per day, 8 many of which are phosphorus binders or blood pressure medications with extensive side effect profiles.9,10 Moreover, aggressive ultrafiltration can contribute to symptomatic posttreatment hypotension, 7 weakness, lethargy, and possibly even heart failure 11 and death. 12 Therefore, while treatment of hyperphosphatemia, hypertension, and hyperparathyroidism can also add to patients' symptom burden, these practices have become a cornerstone in the treatment of ESRD despite scant evidence to support the practice. 13 Practice patterns are largely based on studies from the general population or cross-sectional, epidemiologic studies in the general dialysis population. 14 The benefit of treating these conditions in the high-risk dialysis population remains unknown.
Prior published attempts to palliate burdensome symptoms in ESRD patients have been either modest in scope, 15 focused on individual symptoms, 16 or reported disappointing results. 17 As in palliative treatments directed at other advanced diseases, these interventions have mostly added to standard care, with additional attention to symptoms that might otherwise go unaddressed. To date, no trial has described a palliative strategy that involves removing unproven treatments that may contribute to symptom burden. This study was designed to test the feasibility of a protocol designed to reduce symptom burden in transplant-ineligible patients by liberalizing practice guidelines, specifically minimizing the use of treatments with no proven benefit.
Methods
Study sites and sample assembly
Patients were recruited from two dialysis units, one located in Manhattan and the other in Queens, New York, representing a total dialysis population of approximately 300 patients. Based on previous studies, 4 patients deemed medically nontransplantable comprised approximately 20% of the hemodialysis population. With a projected accrual rate of 40%, the recruitment goal was 20 patients. Patients were recruited by the primary investigator, during a 15-month recruitment period. The study was approved by the Weill Cornell Medical College Institutional Review Board.
Study design
Patients were randomly assigned to intervention or usual care. Patients in the usual care group were treated according to the prevailing dialysis unit practice patterns. Blood pressure was targeted to less than 130 mm Hg systolic prior to dialysis, using a combination of ultrafiltration and medications; serum phosphorus was targeted to less than 5.5 mg/dL, using nutritional phosphorus restriction and use of phosphorus binders; serum parathyroid hormone (PTH) was targeted to 150–300 pg/mL, using vitamin D analogues and calcimimetics. For patients in the intervention group, treatment goals were systolic blood pressure less than 150 mm Hg prior to dialysis, serum phosphorus less than 6.5 mg/dL, and serum PTH 150–500 pg/mL. These goals represented a relatively modest liberalization of treatment guidelines; however, based on our clinical experience, these interventions were thought to be acceptable to both treating nephrologists and patients. Moreover, changes to dialysis frequency, clearance and target hemoglobin could not be made without violating Centers for Medicare and Medicaid Services (CMS) goals.
Primary outcomes included demonstration of feasibility of recruitment, randomization, and application of the protocol and data collection. Additional outcomes were measures of separation between the intervention and usual care groups in the targeted indicators: serum phosphorus and PTH, blood pressure, use of blood pressure medications, phosphorus binders, and vitamin D. Additionally, quality-of-life measures were administered at baseline and at 6 weeks.
The trial lasted 6 weeks. Blood pressure was checked as per dialysis unit protocol, and adjustments were made to dry weight and medications weekly. Serum phosphorus and PTH were checked every 10 days, and adjustments were made accordingly, based on treatment goals. Changes were discussed with and approved by the patients' primary nephrologist. Changes were made only as tolerated by patients' symptoms and other medical concerns. For example, dry weight would only be increased if it would not worsen dyspnea or symptomatic edema, and beta blockers could be maintained if deemed necessary to treat heart failure. Other treatment goals, such as clearance and hemoglobin concentration, were unaffected by the protocol.
Patient surveys were administered at the start of and following the trial, including the dialysis symptom index, 18 SF-36 19 , and the Patient Reported Outcomes Measurement Information System (PROMIS) 20 depression short form. A Charlson comorbidity score 21 was calculated for all patients using data collected from the medical record.
Statistical approach
Because this was a feasibility study, the only tests of statistical significance reported are for the intervention variables targeted for group separation. The Mann-Whitney nonparametric test was used to compare means between usual care and the intervention group for the laboratory values and medications targeted.
Results
Of approximately 300 patients receiving dialysis in the two units, 51 were identified as nontransplant eligible, English-speaking, and able to give consent. Of these, 16 (30%) consented. Eight were randomized to the treatment group and eight to usual care, and all 16 patients completed the trial (Fig. 1).
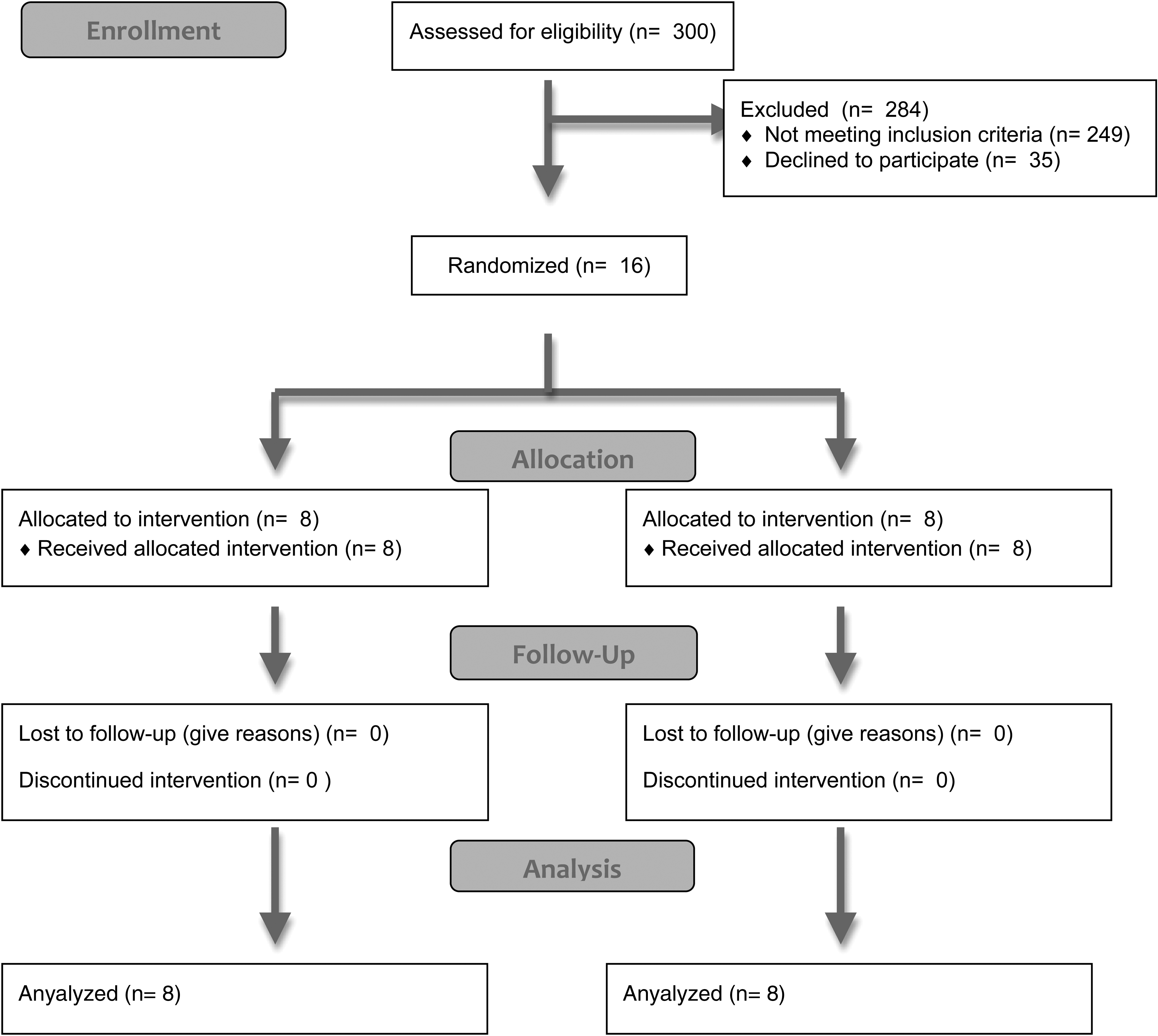
Enrollment and randomization.
There were no significant baseline differences between the usual care and intervention groups with regard to potential covariates such as age and Charlson comorbidity score. Patients in the usual care group had higher mean blood pressure, PTH and serum phosphorus levels at baseline, and the difference persisted throughout the study, but with no statistically significant divergence (Table 1). At baseline, 31%, 68%, and 50% of subjects met usual care treatments goals for PTH, serum phosphorus and blood pressure, respectively; 62%, 81%, and 75% of subjects met intervention treatment goals for PTH, serum phosphorus and blood pressure, respectively.
SD: standard deviation.
Patients in the intervention group trended toward less intensive treatment (Table 2). Over the course of the trial, the daily phosphorus binder intake in the intervention group decreased significantly from 5.63 ± 4.07 pills per day to 1.75 ± 2.19 pills per day; phosphorus binder use increased in the usual care group from 5.25 ± 3.85 pills per day to 5.88 ± 4.91 pills per day (p = 0.011). Similarly, use of vitamin D analogues fell significantly in the intervention group from 7.50 ± 6 μg per week to 5.38 ± 6.25 μg per week, while use in the control group increased from 9.38 ± 6.70 μg per week to 13.13 ± 5.77 μg per week (p = 0.028). The number of medications used to treat blood pressure was stable in the usual care group (staying at 1.75 medications per day) and decreased slightly in the intervention group, from 1.75 ± 1.58 medications per day to 1.63 ± 1.60 medications per day (p = 0.35). Furthermore, patients in the intervention group had their dry weights reduced less often at any point during the trial than those in the usual care group (37.5% versus 75% p = 0.315).
SD: standard deviation; PTH: parathyroid hormone; PROMIS: Patient Reported Outcomes Measurement Information System.
Patients in the usual care group had higher scores on the PROMIS depression survey at baseline and at the completion of the study (52.00 ± 10.77 and 48.38 ± 9.43, respectively), compared with patients in the intervention group (48.90 ± 9.31 and 47.81 ± 9.05). Similarly, the usual care group reported greater symptom burden at baseline and week 6 (39.25 ± 24.30 and 28.30 ± 16.88, respectively) compared with the intervention group (22.50 ± 11.83 and 26.50 ± 16.05, respectively). Patients in the usual care group evidenced slightly lower physical function, slightly less pain, and lower general health as compared to those in the intervention group. As this was a feasibility study underpowered to detect changes in these outcomes, tests of statistical significance were not performed.
Discussion
This feasibility study successfully recruited and randomized high-risk ESRD patients for a trial of reduced-intensity treatment. Patients demonstrated willingness to be enrolled and randomized, with an approximate 30% accrual rate. Furthermore, treating nephrologists were willing to accept these new practice guidelines and did not resist treatment changes made in their enrolled patients. Of the patients who were reluctant to enroll, most expressed anxiety regarding any change to long-established practice patterns. Recruitment of incident dialysis patients, naive and unaccustomed to any practice patterns, may have yielded a higher rate of accrual.
In addition, the protocol reduced treatment intensity in the intervention group, compared with the usual care group. Patients in the intervention group were prescribed significantly fewer phosphorus binders, received less aggressive ultrafiltration, received fewer blood pressure medications, and were treated with lower doses of intravenous vitamin D. Although not all indicators reached statistical significance given the small sample size, these changes were clinically significant and could conceivably result in diminished symptom burden if attempted in a larger, adequately powered study. Additionally, a longer trial may have yielded a larger separation. There were no adverse events related to the study in either group. Despite a reduction in overall treatment intensity, the intervention did not lead to a clear change in blood pressure or serum phosphorus and PTH levels, likely because the trial was of short duration and not powered or designed to do so. Furthermore, data related to a wide variety of symptoms were successfully collected at baseline and at the end of the trial; given the nature of the trial, these outcomes could not be evaluated for statistical significance.
This trial focused on transplant-ineligible dialysis patients, in contrast to previous palliative trials of symptom reduction in dialysis patients, which have targeted the broader ESRD population. 17 Furthermore, previous trials have attempted to add a layer of treatment on top of usual care, or focused on specific treatments or symptoms. 16 The reasoning behind this feasibility trial is novel in several distinct ways. Previous work has shown increased symptom burden in the nontransplant eligible dialysis population. 4 Moreover, this subset of the ESRD population is characterized by risk factors that portend a poor prognosis, namely advanced age, 1 frailty, 22 and multimorbidity. 23 Therefore, modifying treatment in the nontransplantable population may yield higher dividends, given the substantial symptom burden experienced by this population.
Moreover, the risk posed by treatment modification may be lower in this population. High-risk dialysis patients have mortality rates similar to patients with advanced cancer. 24 The putative, and largely speculative benefits of phosphorus and PTH control (i.e., vascular calcification and bone health) may no longer accrue in such patients. Similar to patients with advanced cancer, high-risk dialysis patients may already be at the point in their illness where traditional interventions may no longer be able to modify the course of the disease. 25 Palliative efforts in patients with cancer are often designed by adding interventions to standard care, and withdrawing care whose risks exceed potential benefits. 26 In ESRD, however, standard care is often unsubstantiated by robust prospective data, while carrying substantial risk. To our knowledge, this is the first trial to attempt to reconfigure standard care for the high-risk ESRD population to better acknowledge the potential for increased symptom burden associated with aggressively treating hyperphosphatemia, hyperparathyroidism, and hypertension. This protocol, if proven effective, has the potential to ameliorate multiple different symptoms, rather than addressing each symptom individually.
While our intervention was relatively modest, a more aggressive intervention could be designed that would remove treatment of hyperparathyroidism, hyperphosphatemia and hypertension entirely in the high-risk hemodialysis population. We believe, however, that such an approach would have been met with resistance, while the protocol described above both reduced intensity of treatment and was broadly palatable to both patients and nephrologists. Ultimately, whether a protocol of reduced- intensity treatment would reduce symptom burden without a negative impact on survival awaits a larger, long-term study—and a more modest protocol may have more promise in achieving recruitment goals. Given the overall survival and symptom burden in this population, a 6-month trial might be adequate to demonstrate this concept.
Our study has several limitations that warrant consideration. The study was limited by its small size and short duration. Any definitive conclusions regarding meaning clinical benefits and safety that may be derived from treatment modification would require a well-powered, multicentered trial. Furthermore, there are other domains, such as anemia, frequency of dialysis and clearance that were not addressed, in part because such changes would have likely been met with resistance on the part of nephrologists and patients. And finally, clearing every treatment modification by the primary nephrologist, while making recruiting more feasible, introduced a layer of bias to the protocol.
In summary, this feasibility trial demonstrated that high-risk dialysis patients can be randomized to treatment modification, which successfully reduced treatment intensity. Ascertaining the clinical effects of such a treatment change awaits an adequately powered, long-term study.
Source of Funding
This study was funded by a grant from the Weill Cornell CTSC; and the National Institute of Aging: An Edward R. Roybal Center Grant [P30AG022845].
Author Disclosure Statement
No competing financial interests exit.