
Abstract
Abstract
Background:
Assessment of quality of life is of central importance in palliative care to understand patients' needs and improve their treatment. However, due to the severely compromised state of health of the severely ill or dying patients, the possibility of an adequate assessment with longer questionnaires is limited.
Objective:
Investigation of the criterion-oriented validity of a single item to measure quality of life in palliative care patients.
Design:
In a cross-sectional study, correlations of the single item with established questionnaires were analyzed.
Participants/Setting:
At Malteser Hospital Bonn and Bonn University Hospital, 72 palliative patients, mainly suffering from cancer, were investigated.
Measurements:
Clinical symptoms were measured by the Minimal Documentation System (MIDOS) and quality of life was assessed by the single item “How satisfied are you currently with your physical and emotional well-being?” on a 7-point scale as well as by the Functional Assessment of Cancer Therapy–General (FACT-G) and the Palliative Outcome Scale (POS).
Results:
Seventy-one of 72 patients filled in the single item and the POS, 64 patients the FACT-G. There was a high correlation between the assessment of quality of life by the single item and the FACT-G (r = 0.695, p < 0.01) as well as the POS (r = −0.630, p < 0.01).
Conclusions:
The study confirms the criterion-oriented validity of the single item to measure quality of life in palliative care patients. This can be seen as a first step to validate this economic instrument. Future studies should focus on the analysis of further psychometric aspects (e.g., reliability, sensitivity to change) of the single item.
Introduction
Quality of life in palliative medicine
T
Measurement of quality of life
Against this backdrop, several questionnaires measuring quality of life in chronic illness and cancer patients have been developed, such as the EORTC QlQ-C30, 5 the FACT-G, 6 and the SEIQoL. 7 However, the practicability of longer questionnaires is hampered by weakness, tiredness, and lack of concentration in patients who are severely ill. Consequently, palliative care is in urgent need of very brief, nevertheless valid, questionnaires to adequately measure quality of life. 8 In a previous attempt to meet this challenge, quality of life was measured by the single item 9 “How do you feel today?” and results were compared with findings of established questionnaires such as the SEIQoL, EORTC-QlQ-C30, and FACT-G. The magnitude of correlations ranged from 0.224 to 0.563 in the whole sample with significantly lower correlations in women ranging from 0.101 to 0.461. These results could not confirm the criterion-oriented validity of the abovementioned single item. Nonetheless, as a single-item approach is necessary in terms of clinical practicability, in our study we made a further attempt to develop and validate a single item allowing for a valid assessment of core aspects of quality of life in palliative care. To verify in a first step criterion-oriented validity, we hypothesized strong correlations of the single item with an established quality-of-life questionnaire (Functional Assessment of Cancer Therapy–General, FACT-G) and a slightly lower correlation with a questionnaire measuring quality of care and psychological well-being (Palliative Outcome Scale, POS). 10
Methods
Participants
According to inclusion criteria, the study population consisted of all palliative inpatients at the palliative care unit of Malteser Hospital Bonn as well as all accessible outpatients treated at the ambulance of the Center for Integrated Oncology at Bonn University Hospital and palliative inpatients receiving palliative care from mobile teams at Bonn University Hospital. According to exclusion criteria, all patients who were physically or cognitively unable to complete the questionnaire set were excluded. Recruitment period ranged from May 18, 2011, to March 30, 2012. A total of 72 palliative in- and outpatients participated in the study.
Instruments
Minimal documentation system
The Minimal Documentation System (MIDOS
Single item
The single item, which we investigated, was drafted by our research group. The exact question was as follows: “How satisfied are you currently with your physical and emotional well-being?” Patients were asked to use a verbal rating scale ranging from 1 (dissatisfied) to 7 (satisfied). A second single item (“How would you rate your overall quality of life during the past few weeks?”) to assess quality of life was taken from the EORTC-QoL-C30 questionnaire.
Palliative outcome scale
The POS is a validated multidimensional outcome instrument especially designed for patients with advanced-stage diseases. The POS has been used to measure quality of life in several studies.12,13 It consists of 10 questions about the previous three days in the form of a verbal rating scale (0 = very good to 4 = very poor). POS includes questions concerning pain, other symptoms, general well-being, as well as patient and family assessments of how informed they are about the disease. In addition, the questionnaire asks about patients' emotional state, their sense of self-esteem, their quality of life, whether they believe certain treatments are unnecessary, and practical matters. An open question follows that asks what patients perceive as their three main problems experienced in the past three days. The higher the POS score (maximum 42), the lower the patient's sense of well-being. The questionnaire does not take more than 10 minutes to complete. The test demonstrated good internal consistency (Cronbach's alpha = 0.65). 14 Test–retest reliability, as measured by the proportion agreement within one score between assessments for the questionnaire items was very good, ranging from 0.74 to 1. Further psychometric analysis showed good construct and criterion-oriented validity. 14
Functional assessment of cancer therapy–general
The FACT-G questionnaire aims at collecting data on the quality of life of cancer patients. The 4th version used in this study includes four categories and a total of 27 questions. The categories take into account the aspects of patients' physical, social, emotional, and functional well-being. The collected data regard patients' well-being during the previous seven days. Items are assessed on a rating scale ranging from “0 = not at all” to “4 = very.” The total of the scores correlates with the patients' quality of life (“0 = best possible” to “100 = worst possible”). The FACT-G has demonstrated adequate internal consistency (Cronbach's alpha 0.56 to 0.89) and test–retest reliability (Pearson's r = 0.92) as well as evidence of validity (content, criterion, discriminant). 15
Sequence of the study
The study was approved by the local ethics committee. Inpatients filled in questionnaires after having given informed consent within one week after hospital admission or consultation. Outpatients completed questionnaires within one week after their first outpatient appointment. In most cases, data were collected in the form of an interview where the patient was presented copies of the questions and possible answers. The battery of tests was administered in the following sequence: the two stand-alone questions, MIDOS 2 , POS, and FACT-G.
Statistics
Categorization of answers to the open POS questions was done by content analysis. We performed correlation analyses on the whole patient sample as well as separate analyses on men and women to confirm criterion-oriented validity in both genders. As test data and criterion data were collected at the same time, we analyzed a specific type of criterion-oriented validity called concurrent validity; therefore, both terms are used synonymously in the text. The correlation calculations for the ordinal data were done with the Spearman correlation coefficient, for metrical data with the Pearson correlation coefficient. Differences with an error level of p ≤ 0.05 were considered significant. Expecting a minimum correlation magnitude of 0.35 and a power of 80%, Cohen recommends a sample size of at least 62. 16 Correlation coefficients between 0.31 and 0.50 were considered moderate and those over r = 0.50 were considered high. 17
Results
Forty-one out of 179 patients who were admitted in the recruitment period to the palliative care unit of the Malteser Hospital in Bonn could be included (22.9%). Reasons for exclusion are shown in Table 1. There was no significant difference between participants (17 male, 24 female; age 67.4 ± 13.9 years) and excluded patients (71 male, 67 female; age 71.6 ± 13.2 years) with regard to sex (χ2 = 1.261; p = 0.261) and age (t = −1.78; p = 0.077). In addition, 21 outpatients and 10 inpatients receiving palliative care from mobile teams at Bonn University hospital were asked to participate. All of these patients could be included.
Description of the study population
Diagnoses are summarized in Table 2.
Only four patients suffered from other life-threatening diseases (ALS, renal disease, amyloidosis, mitochondrial disease) than cancer.
Clinical condition on the basis of MIDOS
The most prominent symptoms with regard to frequency and intensity were tiredness, weakness, and loss of appetite (Table 3). Mean and median treatment days were calculated for the treatment duration of patients treated on the palliative care unit. These data were not available for patients treated by the mobile teams. The mean number of treatment days at the palliative care unit was 19 (±12 days SD; median 17 days).
Nine (22%) of the 41 surveyed palliative care unit patients died during hospitalization. Death occurred on average 28.7 days after admission and 15.1 days after being surveyed. Six (14.6%) patients were transferred to an inpatient hospice, and 26 (63.4%) patients were discharged back home.
Quality of life
There were 71 answers to the single item “How satisfied are you currently with your physical and emotional well-being?” that could be evaluated. One patient rated this single question with a three for his physical condition and five for his mental state, noting critically that it is impossible for him to evaluate both aspects in a single question.
Mean for the single item was 3.0 ± 1.49, median 3.0 with a range between 1 and 6 on the 7-point rating scale.
Palliative outcome scale
A total of 71 patients filled in the POS. The mean sum score for all patients was 12.8 ± 6.3 (range 0–35).
To the open POS question “Which (three) problems stood out for you in the past three days?” 85% of patients responded with one or more problems. A second problem was mentioned by 43% of subjects, and 14% reported a third problem. Somatic symptoms ranged in first place, further social and psychological concerns ranged second and third (Table 4). These concerns dealt predominantly with issues of palliative care at home or in hospice as well as worries about the personal future and the future of significant others.
POS, Palliative Outcome Scale.
Functional assessment of cancer therapy–general
In 64 patients, the FACT-G was completed. Patients rated the highest satisfaction with social well-being (Table 5).
Correlations of FACT-G subscales; POS and single item.
p ≤ 0.01, *p < 0.05.
FACT-G, Functional Assessment of Cancer Therapy–General; PWB, physical well-being; SWB, social well-being; EWB, emotional well-being; FWB, functional well-being.
Criterion-oriented validity
The first single item showed a high correlation (Spearman-Rho) of −0.63 with the POS. The correlation (Spearman-Rho) with FACT-G total score was even higher with 0.695. A very high correlation (Pearson) of r = 0.715 (p ≤ 0.01) was also found between the POS and FACT-G total scores. With regard to FACT-G subscales (Table 5), POS and single item showed the strongest correlations with physical well-being and emotional well-being. The subscales social well-being and functional well-being demonstrated weaker associations.
The second single item showed significantly lower correlations (Spearman-Rho) of 0.413 (FACT-G) and 0.322 (POS).
Gender differences
Only slight differences between men and women can be seen in the POS mean values (female 12.94 ± 5.12 vs. 12.64 ± 7.14). Regarding absolute scores on the FACT-G, men rated their quality of life slightly better than women (Table 6). The physical well-being scale showed the largest gender-specific difference in the FACT-G subscales. All correlations between single item and sum scores of FACT-G and POS in male and female subjects were high with a magnitude over 0.5. In male patients, association between single item and FACT-G displayed a very high score with a magnitude over 0.8 (Fig. 1).
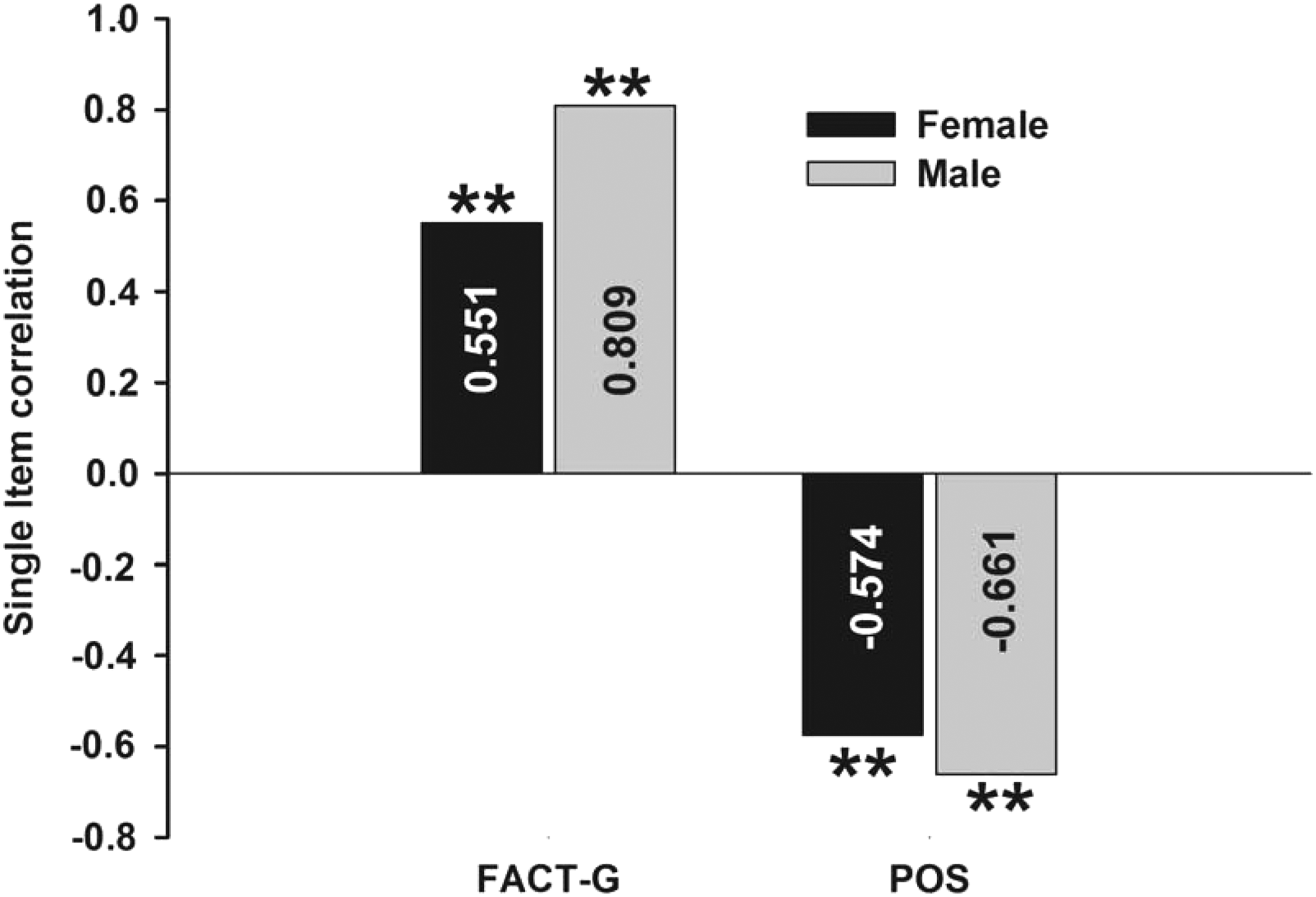
Gender-specific correlations between single item, FACT-G, and POS. FACT-G, Functional Assessment of Cancer Therapy–General; POS, Palliative Outcome Scale. **p ≤ 0.01.
Discussion
Sample characteristics
Our study assessed the criterion-oriented validity of a single item to assess quality of life in palliative care patients. The study sample was typical of palliative care populations previously studied,9,18 in terms of sociodemographic and clinical characteristics. The vast majority of patients in abovementioned studies suffered from cancer, with weakness, tiredness, and loss of appetite being the most prominent symptoms. The mean age of patients ranged from 64 to 71 years, between 48% and 58% of patients were female.
Criterion-oriented validity as measured by FACT-G and POS
As an empirical criterion to test concurrent validity, we selected two internationally well-established questionnaires assessing quality of life (FACT-G) and quality of care as well as psychological well-being (POS) in advanced cancer patients or palliative care patients. As hypothesized, we found a closer association of the first single item with FACT-G compared to the POS, even though this difference was not statistically significant. Thus, the single item showed the strongest association with the questionnaire, which merely measured quality of life and a somewhat lower correlation with the instrument, which captured psychological well-being as well as quality of care. The magnitude of these correlations confirms a satisfactory criterion-oriented and concurrent validity of the single item for assessment of quality of life in palliative care patients. The second single item did not show satisfactory correlations, and so, criterion-oriented validity could not be confirmed. Regarding gender-specific analyses, the magnitude of correlations of the first single item with POS and FACT-G achieved for both sexes high values above 0.5, indicating good criterion-oriented validity. Regarding subscales of the FACT-G, the magnitude of correlations with physical, emotional, and functional well-being ranged above or close to 0.5. Merely, the correlation with the social well-being subscale was moderate.
Criterion-oriented validity compared to previous single-item study
In a previous study by Stiel et al., 9 the single item “How do you feel today?”did not show satisfactory validity. Analysis displayed no association of this single item with social well-being, and gender-specific analysis unveiled correlation coefficients far below 0.5 for women between single item and FACT-G. This may be explained by the fact that the psychological construct of quality of life is highly complex, encompassing not only physical complaints but also emotional and spiritual well-being.3–5 However, a single item asking for current feelings and/or mood might be answered rather spontaneously by the patient, who would not weigh different aspects of well-being before formulating his answer. 19 One could argue that, for example, feeling pain in the very moment of this question may lead to the simple answer “bad” and a low numerical rating, which may not reflect patients overall quality of life. In accordance, a recent study found that reliability and validity of answers to a subjective well-being item in a nonclinical population sample were low for fast respondents aged 70 and older. 19 The patient's answer may also be influenced to a large degree by the expectations of the medical staff. In most clinical settings, patients may be biased expecting medical staff to care about physical complaints much more than emotional or social distress, and may formulate their answer on well-being with this focus in mind. 20 This discrepancy is also reflected in the focus of most quality measures for palliative care. 20 Consequently, we chose a single item, which asked specifically for physical and emotional well-being, thus defining concretely a relevant core content of the psychological construct of quality of life.3–5 This explicit question may prime a reflection process in the patient, weighing individually different aspects of physical and emotional well-being according to a highly individual inner scale. In more complex questionnaires, this process is specified by a more time-consuming set of questions.
Methodological implications of single-item construction
One might argue that the single item is a double-barreled question asking for two issues but allowing only for one answer, which may lead to inaccuracies as there is no indication to which issue the patient is answering. However, the single item aims at assessing the patient's overall well-being by briefly presenting relevant cues. Thus, well-being is not merely the mean of physical and emotional well-being, but the overall score reflects the subjective weighting of the relevance of both aspects. Therefore, the formal inaccuracy is on purpose because it makes the patient clear that a brief response needs weighting and integration of physical and emotional well-being thereby ensuring that all relevant aspects are fully considered. 21 There is sound evidence that longer response latencies in answering double-barreled questions reflect a deeper and more elaborate information processing. 22 This complex single item may also overchallenge patients. Thus, one of our patients felt unable to integrate physical and emotional well-being in one score. Nevertheless, it is highly important to guarantee a precise and valid measurement of quality of life in palliative care, which is not too time-consuming and can be applied easily by health professionals. 23 Criterion-oriented validity confirms the ability of the single item to capture clinically relevant differences in quality of life. The practicality of this instrument and the low burden with the single item ensure that patients far advanced in the disease trajectory such as palliative patients near the end of life are not to be excluded from research projects and in consequence can benefit from the best evidence. The validity of single-item measurement was confirmed in recent years for the assessment of depression 18 and fatigue. 24 De Boer et al. 25 tried to measure global quality of life by a single visual analogue scale (VAS) in advanced cancer patients. On the whole, the VAS showed merely a satisfactory measurement of health perceptions and physical functioning, however, proved inadequate for the assessment of global quality of life.
Single item and social/functional aspects of quality of life
In our study, as in previous studies,9,26 participants' scores on physical and emotional areas of quality of life ranged above scores on functionality and social well-being. This may reflect the greater importance of these two domains for palliative patients in determining quality of life. The answers to the POS open questions show that full integration in work life and social life is obviously not the main focus in palliative patients. Quality of life is more closely connected to issues such as (control of) somatic symptoms and worries about the personal future (length of survival, thoughts about death/dying) as well as the future of significant others (coping, care). Taking a close look at the 7 items of the functionality section of the FACT-G, it becomes evident that functionality predominantly focuses reintegration in daily life as well as acceptance of illness. Items such as “I am able to work” or “My work is fulfilling” or “I have accepted my illness” and “I am able to enjoy life” focus long-term aspects of external and internal coping with illness, which only marginally fit to the situation of palliative care patients. This is also reflected in a very low correlation of this subscale with the POS sum score. Consequently, correlation of our single item to functional areas of well-being of the FACT-G was lower compared to somatic and emotional areas. Our single item displayed the lowest correlation with the section social well-being of the FACT-G. In this section, the FACT-G asks for the emotional support from significant others. However, POS open questions demonstrated that palliative patients were rather concerned with the future well-being of significant others. Apart from that, some of our patients may have felt uncomfortable with FACT-G questions concerning social support (“I get emotional support from my friends”) or sexuality (“I am satisfied with my sex life”), mainly when they became aware of the absence of friends or sexual life. The perception of an inadequate intimacy of specific questions of the FACT-G decreased acceptance of this instrument in some palliative care patients. In these patients, the single-item measurement could be used without any problem, as each patient was allowed to decide individually which physical and emotional areas to include in the personal assessment.
Limitations
A limitation of most studies dealing with palliative care patients is the low inclusion rate due to impaired overall health status. Thus, we could include only 22.9% of palliative care patients on our palliative care unit. This rate is slightly lower compared to the 35% in the study by Stiel et al. 9 The validation in a sample of palliative patients in a relatively good condition suffering mainly from cancer is a limitation of the study that limits generalizability of findings. On the contrary, this finding confirms the rationale of our study that a large number of palliative care patients are not able to fill in longer and more complex questionnaires. Our study may be seen as a first step to confirm the validity of our single item in a palliative care population. Future studies should analyze its reliability, sensitivity to change, as well as further aspects of validity in cancer and noncancer palliative care populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.