
Abstract
Abstract
Background:
Living at home is an important factor for maintaining high quality of life among patients. Many studies have discussed parameters associated with place of death, but no studies have yet clarified which factors influence the length of stay at home during the end of life.
Objective:
The aim of this study was to identify factors influencing the amount of time spent at home during the final month of life among patients with advanced cancer.
Methods:
A retrospective chart review was conducted for 415 patients with advanced cancer. Multivariate multiple linear regression analysis was used to examine relationships between the length of stay at home during the final month of life and variables measuring patient's background (four indicators), family structure (three indicators) cancer type (four types), chief complaint at initial palliative care referral (seven indicators), and medical interventions (three factors).
Results:
The multiple linear regression predicting time spent at home in the last month of life yielded partial regression coefficients of 4.2 for past outpatient palliative care services (OPCS) (p < 0.001) and 3.3 for in-home nurse visits (p = 0.003).
Discussion:
The most influential factor for length of stay at home in the final month of life was a history of OPCS. Many patients with advanced cancer who receive chemotherapy without OPCS spend time as inpatients after an initial period at home. Palliative care interventions for outpatients effectively enable patients with advanced cancer to adapt and continue living at home.
Introduction
P
According to the Consciousness Survey on the Health of Elderly Persons, 49.0% of men and 35.2% of women hoped for in-home care, and 52.1% of men and 54.7% of women hoped to care for their partner at home. Moreover, 65.2% wished to be cared for by their partner when care becomes necessary. The percentage of elderly persons recuperating at home has not increased. 12
Most advanced cancer patients at Japanese cancer hospitals received the first anticancer treatment as inpatients. More than half of these patients received the second anticancer treatment as outpatients. 13 After anticancer treatments, most patients die in acute care hospitals, despite alternatives, including home recuperation and palliative care units. 14
Comprehensive palliative care to outpatients and inpatients allows advanced cancer patients to remain at home. Many studies examining outpatient palliative care services (OPCS),15–18 have indicated improved symptom control, higher patient satisfaction, and end-of-life care.17–19 Standard referral criteria for the timing and OPCS process are needed. 20 To the best of our knowledge, no previous studies have clarified which factors influence the length of stay at home at the end of life. This study identified factors that influence the length of stay at home during the final month of life among advanced cancer patients.
Methods
Kindai University Sakai Hospital is a 310-bed hospital without a palliative care unit. Outpatients can be referred to OPCS for management of pain or other symptoms and Advance Care Planning from within the hospital, or by other hospitals, nearby clinics, and communities. OPCS staff also visit inpatients. A palliative care specialist conducts an initial medical and psychosocial assessment (>60 minutes). Recommendations are made for symptom management and palliative care treatment, education, counseling, and home support. Referrals to home care and the community hospice are made as appropriate. Follow-up OPCS appointments are tailored to the needs of each patient. Urgent hospitalization if symptoms worsen is guaranteed.
A retrospective medical record review was conducted for 485 patients who were continuously treated by the Department of Palliative Care, Kindai University Sakai Hospital, from October 2007 to September 2015. Patients with consultations only (n = 63) or uncertain dates of death (n = 7) were excluded. We included 415 patients who died at the study hospital (n = 392) or at home or at other hospitals (n = 23). Figure 1 illustrates the study protocol. This study was approved by the Ethics Committee of Kindai University.
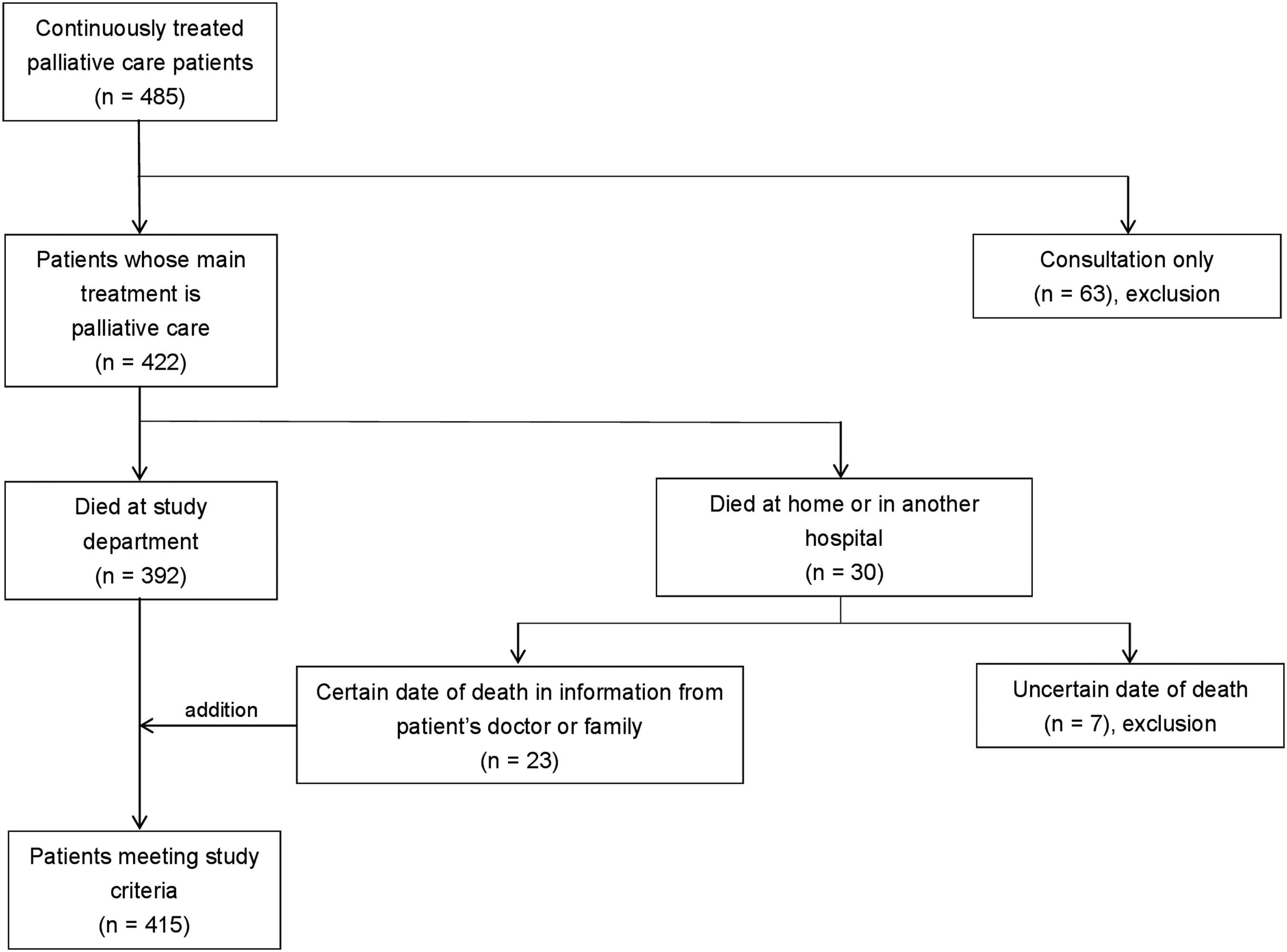
Flow diagram of the study protocol.
The primary outcome was the number of days stay at home in the final month (30 days) of life. The secondary outcome was the length of final hospitalization. For both outcomes, relationships were analyzed with 21 indicators, including the patient's background, family structure, cancer type, chief complaint at initial palliative care referral, and medical interventions. The family structure indicators assessed the potential influence of personal support. Cancer types with the most deaths in Japan in 2014 (lung, colorectal, and gastric cancer) were selected. 21 Small-cell lung cancer was distinguished because it has a short prognosis. The most frequent complaints recorded in the study department were selected as indicators of chief complaints at initial palliative care referral.
Statistical analyses were performed using SPSS, Version 22 (IBM Corp., Armonk, NY). Length of stay at home in the last 30 days of life and length of final hospitalization were the dependent variables in univariate and multivariate multiple linear regression models. 22 The independent variables were the aforementioned 21 indicators. A two-sided significance level of 0.05 was used.
Results
Table 1 shows the patients' characteristics. The sample included 250 males. The median age at death was 72.0 years. The median length of palliative care was 1.8 months (2.9 and 0.6 months for those with and without a history of OPCS, respectively, p < 0.001, data not shown). The median length of stay at home and of final hospitalization were 12.0 and 14.0 days, respectively.
Length of palliative care: from palliative care referral to death.
Lung cancer patients included 11 cases of small-cell lung cancer.
CI, confidence interval.
Table 2 and Figure 2 present the results of the linear regression analysis. The most influential factor for the length of stay at home and of final hospitalization was a history of OPCS. For the length of stay at home, significant differences (p < 0.05) were found for three variables: there were 4.2, 3.3, and 2.1-day increases for those with a history of OPCS, those receiving in-home nurse visits, and males, respectively. In the multivariate model predicting the length of final hospitalization, the partial regression coefficients were −9.8 days for history of OPCS, −7.8 for dyspnea, and −3.7 for men.
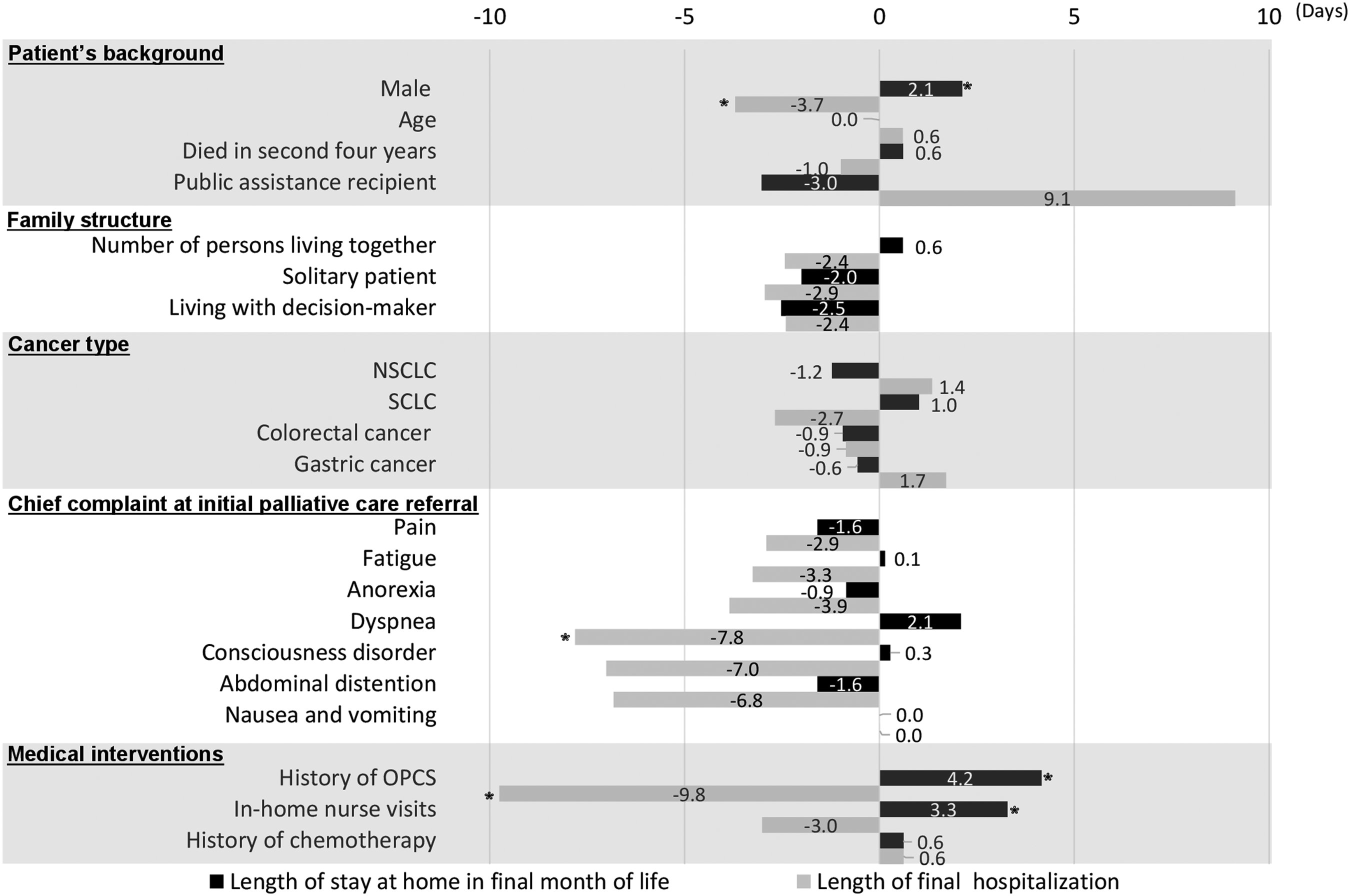
Partial regression coefficients for 21 indicators in multivariate models predicting length of stay at home in final month of life and length of final hospitalization.
Age and number of persons living together were analyzed as ratio variables. The other 19 indicators were analyzed as nominal scale variables. Boldface type indicates significant differences, p values <0.05.
Indicates significant differences, p values <0.05.
NSCLC, nonsmall-cell lung cancer; OPCS, outpatient palliative care services; PRC, partial regression coefficient; SCLC, small-cell lung cancer.
No significant differences were found by age, year of death, or receipt of public assistance. However, the partial regression coefficients for receipt of public assistance were −3.0 days for length of stay at home and 9.1 days for length of final hospitalization. There were also no significant differences by family structure or cancer type. As for the chief complaint at initial palliative care referral, the only significant difference was for dyspnea in the model predicting length of final hospitalization. In terms of medical interventions, the length of final hospitalization did not vary by in-home nurse visits, and neither outcome variable differed significantly by history of chemotherapy.
Discussion
History of OPCS was the strongest predictor of the length of stay at home in the final month of life, and receipt of in-home nurse visits was the second most influential factor.
Several studies have demonstrated the benefits of an oncology palliative care clinic for early palliative care patients in terms of symptoms. 15 The OPCS in this study regularly assesses and confirms the patient's chief complaint; disease state using physical examinations, blood examinations, and radiology; understanding of the disease by the patient and their family; presence of a decision-maker and caregiver; key elements of decision making, including the choice of recuperation location; and physical and psychosocial symptoms. It is unclear which OPCS factors extend the length of stay at home. However, based on anecdotal remarks of patients and their families, regular follow-up and the guarantee of urgent hospitalization if symptoms worsen are likely important determinants of length of stay at home during this period. In the final month of life, symptoms can change quickly, and patients and their families experience increased anxiety. Appropriate regular physical and psychosocial assessments are important when symptoms worsen.
Previous studies have examined the relative benefits of being at home or in palliative care units for end-stage cancer patients. 23 In Japan, it is especially important to determine how best to allocate decreasing medical resources among a rapidly increasing population in need of care. The development of cancer chemotherapies has improved the prognoses for cancer patients and extended the length of outpatient care,24,25 including chemotherapy delivery. Palliative care in Japan has been developed for delivery to inpatients through palliative care units and consultations with palliative care teams. However, outpatient care that includes palliative care may extend the length of stay at home during the final month of life. OPCS in medical institutions, including cancer hospitals, and health insurance incentives for OPCS are necessary. OPCS doctors require access to symptom control methods and systems that draw upon regional resources, including in-home nurse visits, to enable in-home recuperation.
This study revealed variables that affected the length of final hospitalization by at least one week. Public assistance recipients had a tendency toward longer hospitalization and may need more social and human resources to remain at home. Patients with dyspnea or consciousness disorder had a tendency toward shorter hospitalization. Patients who have these complaints at the initial palliative care referral often have poor prognoses and shorter final hospitalizations.26,27 In these cases, follow-up through home visits or urgent hospital admission when symptoms worsen is necessary.
This study's major strength is that it is the first to quantify and compare the determinants on the length of stay at home during the final month of life among advanced cancer patients. The study also had several limitations. First, this retrospective study was unable to determine the effect of the OPCS intervention. Second, these results may not be generalizable to other facilities because they were obtained from outpatients who received palliative care at the acute stage from one hospital. Third, it is unclear which elements of OPCS increased the time spent at home.
Conclusion
History of OPCS was the most influential factor for the length of stay at home in the final month of life. Many advanced cancer patients receive chemotherapy without OPCS and are hospitalized, but these patients are initially able to spend time at home. OPCS interventions effectively enable patients with advanced cancer to live at home.
Footnotes
Acknowledgments
I would like to thank the patients who participated in this study, as well as their families.
Author Disclosure Statement
No competing financial interests exist.