
Abstract
Abstract
Background:
The optimal level of palliative care (PC) involvement in left ventricular assist device (LVAD) therapy has yet to be determined.
Objective:
Describe the feasibility of PC intervention to elucidate patients' goals and values in LVAD therapy in both destination therapy (DT) and bridge to transplant (BTT).
Design:
Single center, prospective, single-arm study.
Setting/Subjects:
All patients who received mandatory PC consultation, using a semistructured script, before LVAD implantation (PreVAD evaluation).
Measurements:
We evaluated the feasibility of PreVAD evaluation and family awareness by analyzing responses and compared it between DT and BTT. We examined the association between withdrawal of LVAD therapy and family awareness in death cases.
Results:
Between January 2014 and September 2016, 112 patients (DT, 75; BTT, 37) underwent PreVAD evaluation. All patients could express what makes their life meaningful, and 101 (92.0%) could discuss possible complications. Seventy-nine patients (70.5%) could articulate their unacceptable health state. There was no difference between both groups. Family awareness increased significantly from 33.0% to 58.0% after PreVAD evaluation (p < 0.01). Five LVADs were deactivated among the 12 death cases, and they were all from the family-aware group (71.2% vs. 0%, p = 0.027).
Conclusions:
Integrated PC intervention was feasible for both BTT and DT patients. Such an intervention may increase family awareness of the patient's unique concerns and may have an impact on decision making at the end of life.
Introduction
L
However, complications of LVAD therapy, including bleeding, infection, device thrombosis, and cerebrovascular events, 3 can negatively impact patients' functioning and QOL, and can place an enormous burden on patients and their families, both physically and psychologically.8,9
According to a recent Joint Commission requirement and Centers for Medicare and Medicaid Services (CMS) Decision Summary for coverage determination, palliative care (PC) should be incorporated into the comprehensive care of LVAD destination therapy (DT) patients.10,11 However, the nature of and extent of PC involvement have not been clarified or critically examined. Swetz et al. report a “preparedness planning” approach for PC involvement, 12 but the optimal level of PC involvement in this population has yet to be determined. Furthermore, although patients for bridge to transplant (BTT) are hoping for transplant and their overall survival is better than that of DT patients, 7 they still experience similar complications which if severe, their LVAD become DT. However, data regarding PC involvement in BTT patients are scarce.
In our institution, we started mandatory PC consultation for both BTT and DT patients in 2014.
In this prospective, single-arm descriptive study, we reviewed our single center's experience of a PC intervention before LVAD implant in both BTT and DT patients. The study describes the feasibility of using a semistructured interview script to elicit patients' values and goals with respect to LVAD therapy and the difference between BTT and DT patients. We also reviewed how this intervention improves the family awareness of patients' wishes before LVAD implant and the effect of family awareness on the decision making at the end of life (EOL).
Patients and Methods
PC consultation before LVAD implant (PreVAD evaluation)
In January 2014, we started mandatory PC consultation for all patients before LVAD implantation. Initially, we evaluated DT patients only, but as of July 2014, we started to include BTT patients too.
Once a decision was made to proceed with LVAD, the PC team was automatically notified. The PC team is composed of board-certified PC physicians, nurse practitioners, social workers, and chaplains. The PC consultation before LVAD implant was routinely performed by a PC physician or a PC nurse practitioner. To address the specific concerns of patients associated with LVADs, and at the same time to minimize the differences between conversations among PC clinicians, we created a semistructured interview script (Table 1) based on the communication literature in PC13–20 and expert opinions from the Columbia University Interdisciplinary LVAD team, which includes PC clinicians, cardiothoracic surgeons, heart failure cardiologists, and cardiology social worker.
BTT, bridge to transplant; DT, destination therapy; LVAD, left ventricular assist device.
This PreVAD evaluation addressed the following: (1) patient comfort, (2) patient and family understanding of LVAD therapy, (3) patient goals and expectations, (4) spiritual needs, (5) possible complications and unacceptable conditions, and (6) decision-making and information sharing preferences. Especially, we used “preparedness planning” as a main reference,12,13 but to avoid overwhelming patients and family who are expecting LVAD implantation in a few days we made our questions focus more on the conditions rather than their thoughts on each medical complication. 14
Of note, we made it clear that deactivation of the LVAD is an option at any future point of time when addressing possible complications and unacceptable conditions. We attempted to do this PreVAD evaluation with the presence of some family members whenever possible, but it was sometimes not achievable due to scheduling problems.
The content of the conversations was documented in the medical record descriptively. Documentation of these conversations was reviewed retrospectively. To measure the feasibility of this intervention, we looked at if patients could respond to questions of domains (3) and (5) in Table 1.
To determine family's awareness of patients' unacceptable health state, we examined two questions and family's presence during the conversation (Fig. 1). We determined the patient's family to be aware of what the patient would consider an unacceptable health state when both of the following conditions were met: (1) the patient was able to articulate an unacceptable health state clearly, and (2) patients self-reported that they have discussed this with the family in the past, or they have not discussed this with the family, but the family was present during the PreVAD evaluation. If patients were not able to articulate clearly, we did not count patients' self-report of the past discussion or family presence during the PreVAD evaluation as family awareness (Fig. 1).
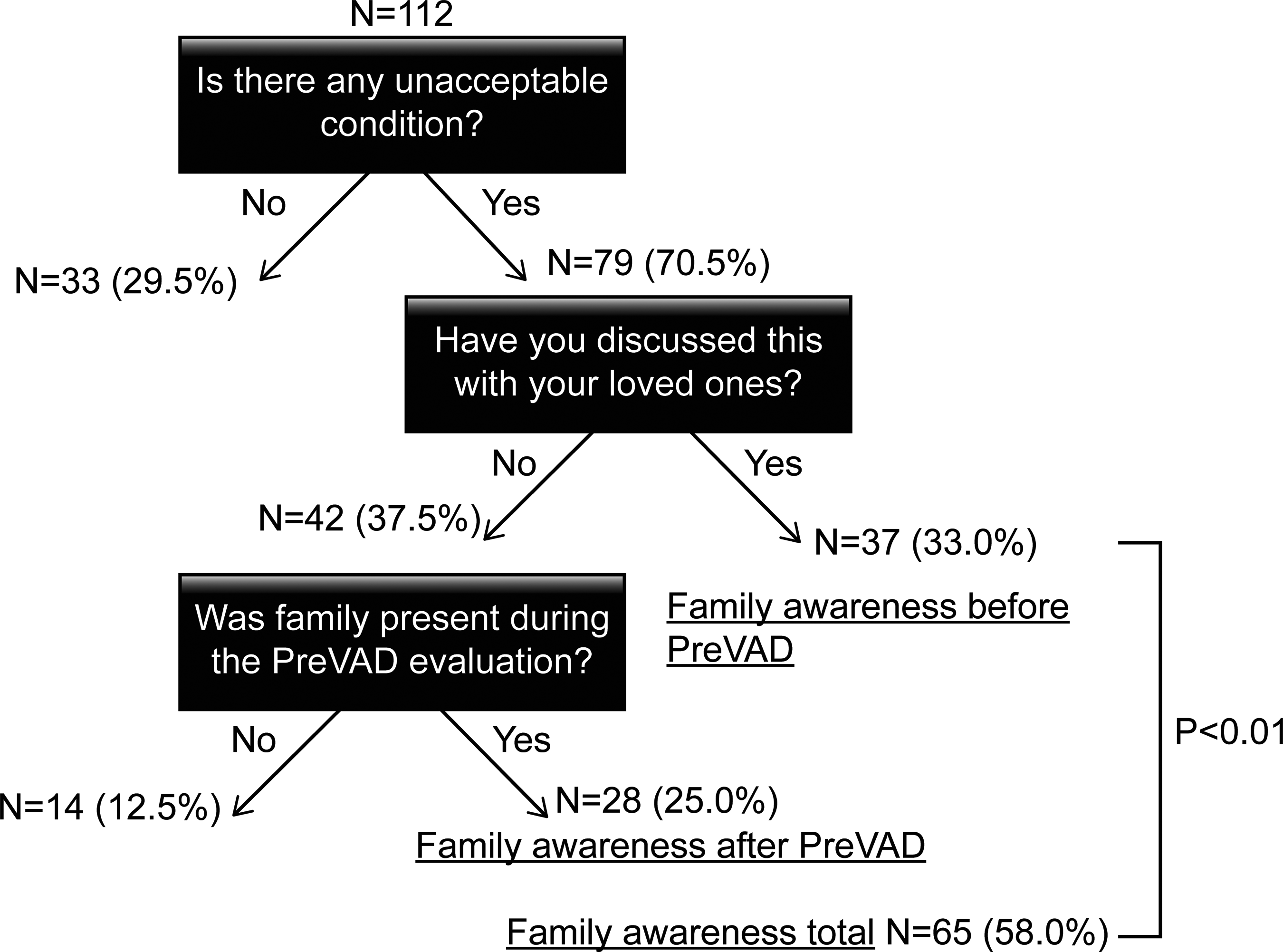
Flowchart depicting the family awareness of patients' unacceptable health status. Among the 79 patients (70.5%) who could articulate what would be their unacceptable health state, 37 patients (33.0%) reported that they had discussed this with their family (family awareness before PreVAD). Among 42 patients (37.5%) who had not discussed this in the past, 28 family members were present during the PreVAD evaluation (family awareness after PreVAD). Family awareness increased from 37 (33.0%) to 65 (58.0%) (p < 0.01).
After PreVAD evaluation, PC was consulted whenever needed throughout the clinical course when the LVAD team had concerns about the overall medical condition (i.e., repeated hospitalizations or declining functional status), or when there were catastrophic events and goals of care had to be clarified, and patient and family needed psychosocial support. The PC team was usually involved when patients with LVADs were at the EOL. In case of death, we reviewed the associations between family awareness of patients' unacceptable condition at the PreVAD evaluation and LVAD withdrawal at EOL in the medical record. We followed up the patients by the end of November 2016. Follow-up was finished when patients passed away or received heart transplant during this period.
We obtained informed consent with written documentation from all the study participants. This study was approved by the Columbia University Institutional Review Board.
Statistical analysis
T test, chi-square test, and Fisher's exact test were used, as appropriate, to test for significant differences between BTT and DT patients. A p-value less than 0.05 was regarded as statistically significant, and all reported p-values were two tailed. Statistical analysis was performed using Microsoft Excel 2011 (Version 14.4.2; Microsoft, Redmond)
Results
PreVAD evaluation
From January 2014 to September 2016, 164 patients received a PreVAD evaluation. We excluded 14 patients who did not receive LVAD by the end of September 2016. Our institution participated in multiple investigational device exemption trials, and 38 patients who received study devices, which have not been FDA approved yet, were also excluded. In total, we included the remaining 112 patients in our analysis. During this period, there were 32 patients who underwent LVAD implantation but did not receive a PreVAD evaluation—inadequate time before LVAD implantation in 18 patients, LVAD for BTT before July 2014 in 8 patients, impaired mental status or clinical condition prohibiting a PreVAD evaluation in 2 patients, and unknown causes in 4 patients.
Baseline characteristics of the 112 patients are shown in Table 2. Patients were predominantly males, and most conversations (92.9%) occurred while they were inpatients. There was no difference in INTERMACS levels between DT and BTT patients, which reflects hemodynamic profile and level of target organ damage. 21 Conversations happened 3.0 days (median, range 1–130 days) before LVAD implantation. In 81 patients (72.3%), these conversations took place with family members present. There was no significant difference between DT and BTT patients. Median follow-up period was 365 days (range 3–966 days). After PreVAD evaluation, patient had 3.5 PC visits on average (range 0–46). Nineteen patients received heart transplant, and 14 patients died during this period.
t Test.
Fisher's exact test.
Chi-square test.
INTERMACS, Interagency Registry for Mechanically Assisted Circulatory Support; Level 1, critical cardiogenic shock—“Crash and Burn;” Level 2, progressive decline despite inotropic support—“Sliding on Inotropes;” Level 3, stable but inotrope dependent—“Dependent Stability;” Level 4, resting symptoms; PC, palliative care; SD, standard deviation.
The feasibility of PreVAD intervention is summarized in Table 3. All patients were able to answer, “What makes your life meaningful?” and 101 patients (92.0%) were able to discuss possible complications. There was no difference between DT and BTT patients. Seventy-nine patients (70.5%) were able to clearly articulate their unacceptable health state, and more patients were able to do that in DT than BTT, but the difference was not statistically significant (76.0% in DT vs. 59.5% in BTT, p = 0.07). Among those who could articulate clearly, there were seven patients who articulated that there was no state that was unacceptable.
Fisher's exact test.
Chi-square test.
Family awareness of patients' unacceptable health state is summarized in Figure 1. Among 79 patients (70.5%) who were able to describe their unacceptable health state, 37 patients (33.0%) reported that they had discussed this with family in the past. Among 42 patients (37.5%) who had not discussed this in the past (hence family was not aware of their unacceptable health state), 28 patients (25%) had family present during PreVAD evaluation (hence family became aware after PreVAD evaluation). Thus, family awareness increased from 37 patients (33.0%) to 65 patients (58.0%) and this increase was statistically significant (p < 0.01). This increase in family awareness was significant in the DT group (32.0% to 64.0%, p < 0.01) (Supplementary Fig. S1A; Supplementary Data are available online at www.liebertpub.com/jpm), but not significant in the BTT group (35.0% to 45.9%, p = 0.34) (Supplementary Fig. S1B).
Family awareness and withdrawal of LVAD at EOL
During the follow-up period, 14 deaths were identified. Two patients died outside the hospital, and the details were not known. The clinical course of the remaining 12 patients, including patients' expressed unacceptable health state, family awareness, and withdrawal of LVADs, is summarized in Table 4. Except one patient, who died three days after the implantation, PC team was actively involved in the care of all 11 patients, in terms of symptom management, assisting in decision making, and providing psychosocial support.
MOF, multiple organ failure.
LVADs were deactivated in five patients (42%). While all the five deactivated LVADs were among seven of family-aware group (71.4%), none of them was among family-not-aware group (0%), and this difference was statistically significant (p = 0.027).
Discussion
In this prospective, single-arm feasibility study, we examined the single-center experience of PC intervention in 112 patients who underwent LVAD implantation. This study is unique because it included both BTT and DT patients and evaluated family awareness of patients' goals and values before LVAD implantation.
The most important finding in this study is that this intervention was feasible; patients were able to have an advance care planning conversations and discuss both benefits and concerns about LVAD therapy even during difficult times in their illness. Even though they were sick as shown in INTERMACS profile numbers and the encounter was right before the LVAD implantation, all patients were able to express what makes their life meaningful, and the majority of the patients were able to discuss severe complications. This was the case for both DT and BTT patients. Although physicians and patients often feel uncomfortable talking about the possibility of death and tend to avoid these conversations,22–24 patients who engaged in EOL discussions did not have worse psychological outcomes, 25 and such conversations can positively enhance, rather than diminish, patients' hope. 26 Our findings suggest that when faced with significant healthcare decisions, advanced heart failure patients are able to discuss their preferences and will likely benefit from these advanced care planning discussions.
The second important finding is that patients' values, especially about what would be considered an unacceptable health state, were not well communicated to their family members, but PreVAD evaluation significantly increased family awareness as per our definition. For patients to receive the care concordant with their values and goals following a catastrophic event, it is desirable that family members are well aware of patients' goals and values. 27 In our data, only 33% of patients had communicated what would be an unacceptable health state. We attempted to include family members in PreVAD evaluations, so that if patients had not considered or discussed their unacceptable health state, family members would become aware when patients articulated it in front of them.
Of note, our data suggest that patients in the family awareness group were significantly more likely to have their LVADs deactivated at the EOL. Data were only available from 12 patients, and with this extremely small sample, this finding may just be by chance. However, this might suggest that dyads who are congruent in patients' goals and values have the clearer understanding of the role of LVADs in their healthcare goals, so that once it turns out that LVADs cannot achieve that goal, it could be less difficult for them to make a decision to deactivate their LVADs. Studies have shown that patients' unacceptable condition could evolve over time.28,29 In our institution, PC continues to get involved after the implantation when patients' clinical condition deteriorates or when there is a catastrophic event. In these instances, PC has conversations similar to PreVAD evaluations using questions in Table 1 and this includes family members. One possible explanation is that for families who are aware of patients' value at LVAD implantation, it is more likely that it continues to be shared throughout their clinical course even if their goals evolve over time. One study has shown that 47% of LVAD patients had advance directives (ADs), but none of them explicitly mentioned the LVAD or withdrawal of LVAD support at the EOL. 30 Explicitly documented ADs would likely be helpful to reduce family stress in case of catastrophic situation or at the EOL, although ADs may nonetheless have some limitations as one cannot describe every possible scenario. 20 Accordingly, it is important that patients' goals and values be shared in advance care planning conversations among family and clinicians.
The strength of this study comes from both BTT and DT patients and comparing both groups. The importance of PC in DT patients has been already discussed in the literature,12,13,31 and both the Joint Commission and CMS have thus far required PC involvement for DT patients. In BTT patients, LVADs are supposed to be temporary, and they have better survival than DT patients. 32 Therefore, the goals, expectations, mindset, and overall comorbidity status of each group could be different. However, only 31% receive heart transplant in one year, 7 and adverse events do occur in BTT patients too. 33 In our data, BTT patients had more difficulty articulating their unacceptable state than DT patients, even though it was not statistically significant. One possible explanation is that, unlike DT patients, BT patients might regard LVADs as only the temporary bridge, and therefore, it is harder for them to prepare for the possible negative events caused by LVADs, in which case, both patients and family, being less prepared, could be more devastated in a catastrophic event. Thus, we believe that both populations benefit from PC interventions from the very beginning of LVAD therapy.
There are several limitations in this study. First, this study was done in a single institution and our findings are therefore not generalizable. Second, our results are descriptive; we did not have a control group and, therefore, could not directly compare the effect of this PreVAD evaluation with those who did not receive it. Third, we defined family awareness as described, but we did not ask the family about their awareness directly. In addition, we defined the effect of PreVAD evaluation on family awareness as their presence in the PreVAD evaluation, which was achieved in 72.3% only. This could have effected the lack of significant increase of family awareness after PreVAD evaluation in BTT patients. However, if there were more family presence, more family would become aware of patients' wish, and therefore, family awareness after PreVAD would only increase, and therefore, we do not think that it influenced our conclusion.
Conclusions
In conclusion, this prospective, single-arm study in a single center illustrated that an integrated PC intervention focusing on PreVAD evaluation is feasible for both BTT and DT patients to express their goals, values, and concerns. Furthermore, such an intervention may increase family awareness of the patient's unique concerns, which may improve surrogate decision making at the EOL. Thorough conversations with patients and families before LVAD therapy could be tremendously important. In the future, further studies are needed to evaluate the more appropriate timing and duration of PC interventions. Also, more importantly, the clinical outcome of these PC interventions, such as patients' QOL, resource utilization, and caregiver burden, need to be investigated.
Footnotes
Acknowledgments
We thank the Adult Palliative Care Service at New York Presbyterian Hospital/Columbia University for the care they provided to the LVAD patients in this study.
Author Disclosure Statement
Dr. Nakagawa and Dr. Naka received consulting fees from Thoratec. All other authors have nothing to disclose. All authors have approved the final article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.