
Abstract
Abstract
Background:
The development of palliative care in Peru remains limited, particularly for nononcological services, such as neurology. The goal of this study was to explore attitudes toward and knowledge about palliative and end-of-life care among patients, families, nurses, and doctors in a specialized neurological institute in Lima, Peru.
Materials and Methods:
We used a mixed methods approach consisting of 78 surveys and 21 qualitative, semistructured interviews that were recorded, transcribed, and analyzed using thematic analysis.
Results:
Surveys identified a substantial need for palliative care in the neurological institute (63% of doctors and 77% of nurses reported palliative care needs in >30% of their patients), and for training (82% of doctors and 69% of nurses reported inadequate palliative care education). The key themes emerging from qualitative interviews concerned transparency of communication about prognosis and end-of-life choices in neurological disease. Familiarity with advance directives was limited among both clinicians and families, and participants were divided about whether or not patients should be informed of serious diagnoses and prognoses, and who should inform them. Barriers to transparency in patient–physician communication included (1) expectation of cure; (2) physician's lack of training in communication and end-of-life care; (3) a paternalistic culture; and (4) the nature of neurological diseases.
Conclusions:
Our study highlights opportunities to enhance palliative care and communication education for neurology providers and the public in Peru, a country that currently has no palliative care training program and no legal basis for advance directives.
Introduction
P
Patients with neurological illness possess additional and unique palliative care challenges, and recent studies suggest a substantial need for palliative care research and training specific to neurology.4–7 While the field of neuropalliative care is still relatively young, 8 evidence is accumulating suggesting benefit of palliative care for several neurological illnesses.9–11 Palliative care in the United States initially developed in tandem with cancer care, and was only later applied to patients with nononcological diseases. This post hoc integration of the fields has led to difficulties that may perhaps be avoided in LMIC countries, such as Peru, where palliative care is still in early development.
Peru has 9.2 doctors per 10,000 people, and 0.42 palliative care inpatient units per million people, placing it at the lowest rate of provision of palliative care services in Latin America after Honduras. 12 In 2007, the Interdisciplinary Peruvian Coalition Against Cancer and the Ministry of Health declared the development of palliative care services for patients with cancer a national priority.12,13 However, no legislation or direction has been provided for noncancer patients. The goal of this study was to explore the attitudes of patients with neurological diseases and their families, as well as neurology health care providers (doctors and nurses) in Peru toward palliative care and palliative care education, especially as it relates to neurologic disease.
Materials and Methods
Ethical clearance for this exploratory, mixed methods study was obtained from the University of Washington (Seattle, WA) and the local Institutional Review Board of the Instituto Nacional de Ciencias Neurologicas (INCN) in Lima, Peru.
Setting
The INCN is a public tertiary care level institute for neurologic clinical care, education, and research under the Peruvian Ministry of Health. It is the only specialized neurological hospital in the country and is a national referral center for neurological disease.
Participant recruitment
All patients and family members were recruited from one of the hospital units dedicated to neurological intensive care, neurodegenerative diseases, neurovascular disease, or neuroinfectious disease. Two investigators systematically rotated between the different units reviewing the patient charts to determine whether patients fulfilled inclusion criteria: modified Rankin Scale >2 (at least moderate disability), and inpatient hospital stay of at least 5 days. The modified Rankin Scale was used to ensure a certain degree of illness severity while avoiding the stereotype that palliative care is limited to patients with poor prognosis. We deliberately included a broad range of neurological conditions to explore common themes across neurological disease. Eligible patients and family members were invited, and if they agreed, their nurses and physicians were approached to participate in qualitative interviews and a brief survey. Purposive sampling for the semistructured qualitative interviews was used across clinicians to ensure representation from various subspecialties of neurology and levels of training, and this sampling was similarly applied with patients and their families to achieve narratively active participants with a variety of neurological conditions. Interviews were continued until thematic saturation of communication and decision-making topics was reached.14–16
Surveys
The survey was developed in Spanish based on a literature review focused on similar previous surveys,17–20 discussion with Peruvian palliative care physicians, and pilot testing with five volunteer physicians to ensure clarity in wording and structure. All study participants completed a basic sociodemographic questionnaire. Physicians and nurses were asked additional questions exploring their attitudes toward palliative care.
Descriptive analyses using mean and medians for continuous variables and frequencies for categorical variables were completed for survey data.
Semistructured interviews
Interviewers participated in a 2-day qualitative research training session developed by experienced qualitative researchers from Peru and the United States. Initial interview guides with open-ended questions were developed with advice from U.S.-based palliative care experts and Peruvian neurologists, and modified over the course of the study to better explore areas of interest. Sample questions are presented in Table 1.
Representative Questions from the Semistructured Interview Guides
The questions below are translated from the original Spanish interview guide.
Interviews were audiorecorded and professionally transcribed.
Qualitative analysis
We used thematic analysis, a qualitative descriptive research method.15,21 Our analytic team consisted of a U.S.-based medical student, and two physicians with palliative care training, including a Peruvian geriatrician and a U.S.-based neurologist. After reading all the transcripts in Spanish individually and creating initial coding of the transcripts, the investigators met weekly to develop a codebook and discuss emerging themes. Once a codebook was agreed upon, codes were entered into Dedoose, a web-based qualitative data analysis software program.22,23 All transcripts were coded, and then excerpts from each code were reread and discussed by the team. The analysis was conducted in Spanish, with quotations translated into English and edited for clarity. Trustworthiness was established through member checks of the final results and triangulation, or checking the results from different sources or perspectives (i.e., patients, family members, and clinicians). 14
Results
Survey outcomes
We administered 78 questionnaires to 21 patients, 16 family members, 28 doctors, and 13 nurses. Participating patients had a mean age of 58.6 years, a mean hospital stay of 17.1 days, and two-thirds were women. Patients were located in the neurovascular (n = 7), neurocritical care (n = 7), neuroinfectious (n = 3), or neurodegenerative (n = 4) units. Among the family members interviewed, one-half identified as the children of the patient, and the remainders were spouses (12.5%), parents (18.8%), or siblings (18.8%). The majority of family members (62.5%) reported that their loved one could not make decisions independently. Participating physicians tended to be younger and less experienced than participating nurses (Table 2).
Characteristics of Enrolled Participants
One patient did not report religion and educational attainment.
mRS goes from 0 (no functional limitation) to 6 (death).
Only one in 10 doctors and one in 6 nurses reported having received some formal palliative care training. One quarter of doctors and less than one half of nurses knew what an advance directive was. None of the clinicians surveyed “definitely agreed” that they had received adequate palliative care training. While most clinicians found that a substantial proportion of their patients had palliative care needs (Table 2), only 25% of doctors and 46.2% of nurses “definitely agreed” that palliative or terminal care was a rewarding part of their work (Fig. 1; Supplementary Table S1, which is available at www.liebertpub.com/jpm).
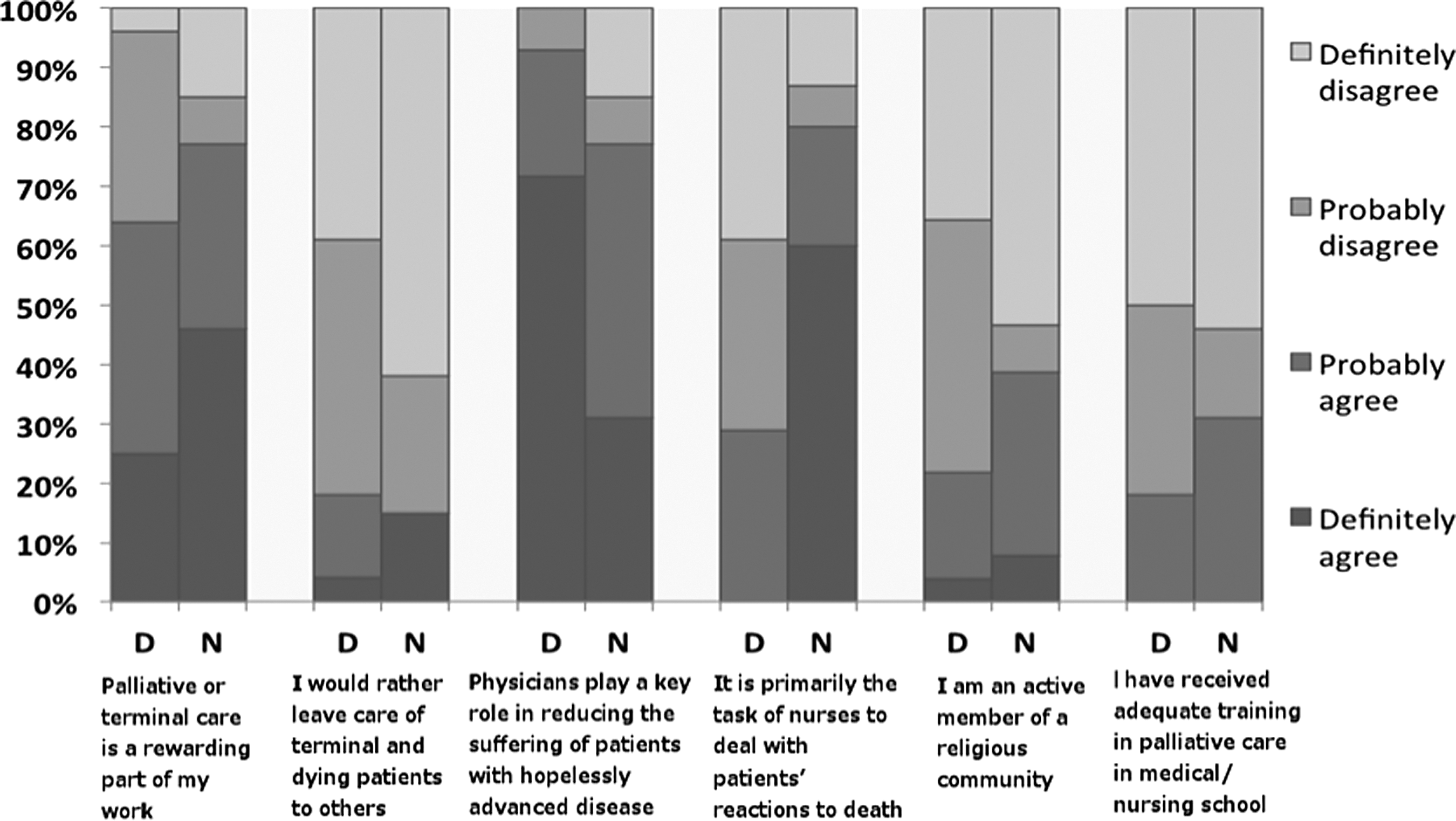
Health care provider survey results: palliative care attitudes and experience.
Qualitative interviews
Of the 78 survey participants, one quarter also participated in semistructured interviews (n = 21; 3 patients, 10 family members, 2 nurses, and 6 MDs). The key themes that emerged from our interviews centered on issues of communication, especially about end of life, prognosis, and treatment decisions. More specifically, we found an ambivalence concerning the transparency of communication: on the one hand, participants neither had much experience with advance directives or the concept of treatment choice, nor felt comfortable with end-of-life conversations. On the other hand, participants indicated that transparency around prognosis and end of life might be helpful, and several barriers to transparency were identified; these included a focus on cure, paternalism, lack of physician training, and conversation barriers specific to neurological disease.
Communication: Status quo
Inexperience with “the conversation” and advance directives
Few family members reported ever having a conversation regarding their health care preferences for end of life.
Fam3: He's never informed us that if for example he is hospitalized or if he … was feeling ill, to have something administered to relieve the pain…Like others could say, I don't want to suffer so much and it would be better if I am given something to rest eternally….no, he has not told us that.
They also did not have a good understanding of the term or concept of “advance directive” or “living will”(“directriz anticipada” or “testamento viviente”) and many confused advance directives with a material will.
Interviewer: Have you ever heard of advance directives or living wills?
Fam17: Yes…if a person say, has property and things, they can write a will saying to one person they leave one thing, to another…
Physicians also reported that advance directives were not routinely used.
Doc16: Here to be honest I haven't seen nor heard of this… it's a cultural issue. … I haven't seen much, except for some issues where sometimes because of religion… some do not want to be intervened on … in different ways, with transfusions…
One doctor described a lack of legal clarity for the use of advance directives or do-not-resuscitate orders and their documentation:
Doc17: Yes, living will…I know that term, but here, it generally does not apply. I think in our country there are actually no clear legal rules.
Discomfort with “the conversation”
Many patients and their families were reluctant to talk about the implications of serious illness or end-of-life issues both among themselves and during the interviews. Initial attempts to talk about poor outcomes or death in our open-ended interviews were thwarted by evasions, expressions of optimism, and seeming misunderstandings. Revealingly, it became necessary to utilize deliberate strategies and hypotheticals to elicit direct responses from participants about end of life.
Interviewer: Do you believe there are better and worse ways to end life?
Fam16: Ummm….
Interviewer: What should the care of a person who is very ill be like?
Fam16: I think … we are confident that from here on, he is going to improve.
Some family members also stated that they felt it was important to discuss end-of-life issues ahead of time, but their family was too uncomfortable to engage with them.
Fam3: I talked to my daughter, but my daughter tells me to be quiet, not to talk nonsense, not to say that…”
Considering “the Conversation”
Despite not having discussed these issues with their respective families, some participants revealed that they had thought about the concepts of death and dying for themselves and showed some openness to the discussion. In response to questioning about what constitutes a “good death,” participants repeated that a death without suffering, or without pain, was a good death:
Int: What would be the worst way to die? Fam5: A good way to die would be to simply fall asleep and remain like that… [The worst way is] To suffer like this, with all these machines, suffering with oxygen.
We identified several instances in which participants suggested that openly discussing difficult topics might be helpful. Several participants became emotional during the course of the interview, but then ended by saying they found the discussion during the interview itself beneficial.
Fam3: I'd like to tell you that…I think the communication between you and me with this interview, with these questions….I feel a little more free.
At other times during the interviews, family members spontaneously expressed their wishes for themselves in ways that were similar in tone to end-of-life conversations.
Fam14: “I get here, and they [the patients] are suffering in bed, not speaking, and they are young. I tell you, … I would not want to be like that.”
Barriers to Transparency in Communication
Focus on cure
When asked about their priorities for end of life, many family members recentered their focus to the topic of a cure. Additionally, the strongest exemplars we encountered of family dissatisfaction pertaining to communication issues were due to lack of focus on a cure by the medical care team. In one case, a family member described how upset she was with the doctors who said her loved one's recovery was unlikely:
Fam17: it was very very cruel…while the other doctors told me to wait for a miracle and to have patience…this manner [of speaking or delivering news]…very very very grotesque.
Lack of physician training or interest
Physicians reported they were socialized to focus on curative care, with minimal emphasis placed on symptomatic relief at the end of life, end-of-life decision making, and communication of bad prognoses:
Doc17: They definitely do not teach you how to give information to the family member.
Some physicians also mentioned a lack of interest on the part of health professionals as an obstacle to improved palliative care.
Doc16: We are missing a little…not only trying to focus on finding the cure or the drug that improves or treats the multiple sclerosis, but also the drug that can decrease the intense pain that these patients can have…we have not been prepared to focus so much on this, and sometimes there is not so much interest from the health professional.
Other physicians admitted to avoiding difficult communication because it was unpleasant to cause families distress. Speaking of her first experience delivering bad news, a resident said:
Doc15: Uy, it was shocking, it sensitized me a lot…The family becomes vulnerable and in some way it affects you. I do not like it.
Protecting the patient
Some family members felt strongly that the patient, and sometimes even the patient's other loved ones, should be “protected” from knowing their prognosis.
Fam1: The [teenage] daughter of my sister…wants to come to see her, but I have forbidden it. It is shocking … imagine how it would affect this girl … to see her mom in conditions that … never, never. I think no one would want to see a family member in these circumstances …
Physicians feared that patients might feel abandoned if they gave them no hope for cure. Physician comments reveal the fear of emotional or inappropriate responses on the part of the family when confronted with difficult news at the end of life.
Doc14: When you talk to the family members about the fact that the probability of recovery for the patient is low…I've seen some sad cases where the family becomes entirely absent…they stop coming and the patient ends up alone, without family, and obviously this increases the suffering.
Various attending-level physicians suggested that the culture of medicine in Peru prescribed a predominantly paternalistic communication style:
Doc17: There is still this paternalistic concept by which we know what the patient needs and everything they should receive. Everything we indicate is correct and the best thing for the patient…We don't listen very much to the family…We listen less than we should.
Nature of neurological illness
When comparing palliative care of neurological and nonneurological patients, doctors emphasized the importance of addressing the consequences of severe neurological disability when providing neurological palliative care.
Doc17: We have patients who have sequelae of brain trauma, and we have patients who have permanent neurologic disability as a consequence of surgery…they do not have their autonomy. To return to society. I believe that all of these are or should be included in palliative care. And there is nothing, no? They are left up in the air.
Doctors also noted that the type of behavioral and cognitive problems faced by patients with serious neurological disease differed from other types of illness where pain is the overriding concern.
Doc 14: With both diseases, they can suffer pain…but neurologic patients have their own particularities, these patients sometimes may be awake, may be agitated, so they behave in a different way.
Doctors also reported that communication deficits in neurological disease complicated the patient–family relationship.
Doc17: In patients with cancer, the family member accompanies them, the family member is there…the patient communicates, expresses himself…however, unfortunately in neurologic diseases, they cannot communicate with the family anymore… there is worsening of the family relationship as well.
Neurological deficits of expression hindered patient–physician communication as well.
Doc17: In patients who have…for example, aphasia, and it is not possible to communicate adequately with them… we cannot have all the information that we want.
Doctors and family members alike also perceived that severe neurological disease, particularly cerebrovascular disease, had a higher degree of prognostic uncertainty than nonneurological disease (Table 3).
Examples of Participant Quotes
Doc, doctor; Fam, family member; Int, interviewer.
Fam14: Cancer advances more quickly…for example with a hemorrhage or stroke, you can be quickly be left like a vegetable…Or it can last many more years.
Discussion
Effective communication is a cornerstone of palliative care and fundamental to the care of people facing a serious illness and an uncertain future for themselves or someone close to them.3,24–26 For example, studies in high-income countries have suggested that most patients wish to know their diagnosis and prognosis.26–30 However, physicians are often hesitant to tell a patient about the presence or severity of their illness, because they see truth telling as detrimental to their goal of maintaining hope, protecting the patient, or avoiding uncomfortable emotions 26 even though realistic expectations of life expectancy do not preclude hope or a spiritual approach to illness. There is also substantial regional and cultural variation in physician attitudes regarding truth telling, 31 with one study showing that 93% of Canadian physicians vs. only 18% of South American physicians believed that their patients would want to know of a terminal illness. 32 It is less clear whether these numbers correlate with attitudes in the general population.
In this single-center study in a neurological institute in Peru, we identified a variety of perspectives concerning the communication about end of life, prognosis, and treatment decisions as well as four important barriers to transparency in patient–physician communication. These barriers were a focus on cure, lack of physician training, a culture of protecting the patient, and the nature of neurological illness. In general, patients, family members, and clinicians felt inexperienced and uncomfortable considering these conversations. Neither clinicians nor families had a clear understanding of advance directives, leading to lack of discussion and documentation of patient's treatment preferences. When advance directives are not documented, patients are at risk of receiving undesired care. 33 Participants seemed divided about whether or not a patient should know about their serious diagnosis and prognosis, preferring to focus on cure. Finally, participants also noted the particular challenges of dealing with neurological conditions because of patients' cognitive or communication impairments, as well as the substantial prognostic uncertainty.
Surveys identified a high proportion of palliative care needs in patients and their families concurrent with a lack of palliative care education and training in the neurological institute. Providers felt uncomfortable with basic palliative care skills such as initiating difficult conversations or breaking bad news. Because these skills are fundamental to developing a trusting clinician–patient relationship, the inclusion of basic palliative care and communication training into the Peruvian health system needs to be a priority. Peru has no legal frameworks for advance directives or living wills, no official accreditation in palliative care available, and no national standards or guidelines for the development of palliative care, 34 lagging behind peer countries such as Chile, Argentina, or Colombia. 35
This study suggests an urgent need as well as a desire among both the public and health professionals to advance palliative care in Peru and identifies barriers to high-quality palliative care provision, laying the groundwork for future interventions in palliative care education, research, and implementation.
Footnotes
Acknowledgments
The authors thank Miguel Inca-Martinez, Indira Tirado, Karina Milla-Neyra, Maryenela Illanes-Manrique, Danny Barientos-Iman, Carlos Abanto, and Diana Salazar Sauñe for logistical support with conducting the study. They thank Ximena Salazar Lostaunau for help with the qualitative interview training, and guidance in qualitative methodology. They also thank Sol Salazar for performing the interview transcriptions, and Angelica Gamarra for her role in participant recruitment and qualitative interviewing. The authors thank Joseph Zunt for critical review of the article, and guidance throughout the project execution. This project was supported by the NIH [Research Training Grant #R25 TW009345] funded by the Fogarty International Center, the NIH Office of the Director, Office of AIDS Research, the NIH Office of the Director Office of Research on Women's Health, the National Heart, Lung, and Blood Institute, the National Institute of Mental Health, and the National Institute of General Medical Sciences.
Author Disclosure Statement
Dr. Anastasia Vishnevetsky received funding from the NIH. Dr. Carla Zapata del Mar, Dr. Juan Luis Cam, and Dr. Mario Cornejo-Olivas reports no conflicting interests. Dr. Claire Creutzfeldt received funding from the Cambia Health Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.