
Abstract
Abstract
Background:
Conversations with seriously ill patients about their values and goals have been associated with reduced distress, a better quality of life, and goal-concordant care near the end of life. Yet, little is known about how such conversations are conducted.
Objective:
To characterize the content of serious illness conversations and identify opportunities for improvement.
Design:
Qualitative analysis of audio-recorded, serious illness conversations using an evidence-based guide and obtained through a cluster randomized controlled trial in an outpatient oncology setting.
Setting/Measurements:
Clinicians assigned to the intervention arm received training to use the “Serious Illness Conversation Guide” to have a serious illness conversation about values and goals with advanced cancer patients. Conversations were de-identified, transcribed verbatim, and independently coded by two researchers. Key themes were analyzed.
Results:
A total of 25 conversations conducted by 16 clinicians were evaluated. The median conversation duration was 14 minutes (range 4–37), with clinicians speaking half of the time. Thematic analyses demonstrated five key themes: (1) supportive dialogue between patients and clinicians; (2) patients' openness to discuss emotionally challenging topics; (3) patients' willingness to articulate preferences regarding life-sustaining treatments; (4) clinicians' difficulty in responding to emotional or ambiguous patient statements; and (5) challenges in discussing prognosis.
Conclusions:
Data from this exploratory study suggest that seriously ill patients are open to discussing values and goals with their clinician. Yet, clinicians may struggle when disclosing a time-based prognosis and in responding to patients' emotions. Such skills should be a focus for additional training for clinicians caring for seriously ill patients.
Introduction
People living with a serious illness may face added suffering due to poor communication, emotional distress, and discordance between the type of care desired and the care received.1–4 Historically, completion of advance directives (AD) has been promoted as one way to ensure that patients receive the care that they want at the end of life. 5 However, AD have not proved to be consistently effective in achieving this.6,7 In addition, focusing on their completion may lead clinicians to limit conversations to medical procedures rather than discussing patient-centered values, goals, and preferences.5,8–11
Therefore, experts increasingly emphasize the importance of discussing and recording patients' values and goals.1,12,13 Research demonstrates the feasibility and benefit of such conversations, with positive effects on quality of life (QoL), distress, and goal-concordant care near the end of life.14–17 Recommendations about best practices regarding such conversations include understanding the patient's view of his/her illness, exploring information preferences, sharing prognostic information, understanding fears and goals, exploring views on trade-offs, and impaired function as well as wishes for family involvement. 18 In addition, experts advocate the use of open-ended questions.19–21 Yet, training clinicians to have these conversations and ensuring that such conversations are of sufficient quality remains an important challenge.22,23
Previous work has shown that patients value honesty, good listening skills, and humanity in their clinicians when talking about serious illness and has also demonstrated that clinicians struggle when disclosing prognosis or discussing care options near the end of life.24,25 Little is known about the details illustrating some of these challenges during such conversations. 26 We therefore analyzed serious illness conversations, as informed by a structured conversation guide, between trained oncology clinicians and their patients to characterize the content and interactions of these conversations.
Methods
Trial design and setting
The Dana-Farber Serious Illness Communication trial has been previously described. 13 This cluster-randomized controlled trial assessed the impact of a multicomponent, communication quality improvement intervention in an outpatient oncology setting. Only clinicians and patients assigned to the intervention arm of this trial were eligible for inclusion in the current study. The goal of this intervention was to move serious illness conversations to an earlier stage in the course of illness, in an outpatient setting, and with the patient's usual clinician. We defined a serious illness conversation as a type of advance care planning that focuses on values, goals, and preferences about future care between a clinician and a seriously ill patient. The trial and this study were approved by the Dana-Farber Cancer Institute (DFCI) Office for Human Research Studies (IRB).
The intervention consisted of tools, training, and system changes designed to support clinicians in having a serious illness conversation. Intervention clinicians (physicians, nurse practitioners, or physician assistants) received a 2.5-hour skills-based training to use the “Serious Illness Conversation Guide” (SICG). Clinicians then systematically used the surprise question (Would you be surprised if this patient died within the next year) to identify eligible patients with advanced cancer whom they believed were at risk of dying within one year. 27 Directly after the conversation, clinicians reported on the duration of the conversation. Control clinicians received no skills-based training or systems supports and were not provided with the SICG.
Serious Illness Conversation Guide
The SICG (Fig. 1) is an evidence-based, clinician-facing framework for best communication practices. 13 It consists of eight components and supports clinicians in conducting patient-centered serious illness conversations, using open-ended questions and patient-tested language. This guide allows clinicians to explore a patient's view of his or her illness, information preferences, goals and fears, views on trade-offs and impaired function, and wishes for family involvement. This version of the SICG also suggests that clinicians tailor their time-based prognostic disclosure to a patient's individual information preferences.
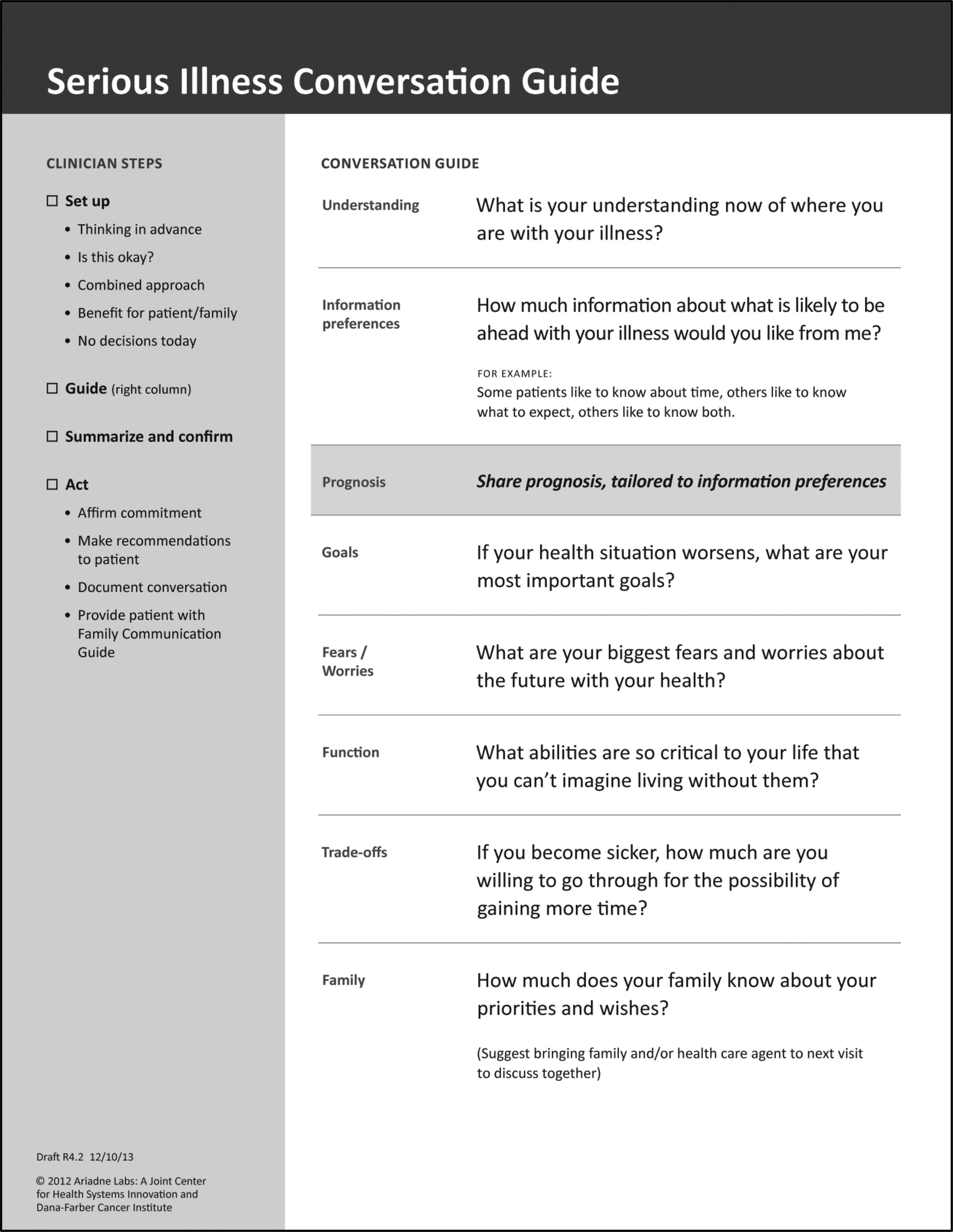
The Serious Illness Conversation Guide.
The skills-based training included additional information, a role playing exercise, and explicit advice for clinicians to speak <50% of the time to support open-ended question use and successful patient engagement. In addition, clinicians were encouraged to follow the structure of the SICG, to respond to patient emotions and expressed concerns, and to de-emphasize decision making, so as to lessen anticipated anxiety for patients.
Qualitative study sample
Patients eligible for inclusion in the trial were 18 years or older, received their oncology care at DFCI, spoke English, and were without cognitive impairment. Full inclusion and exclusion criteria are described elsewhere. 13 Clinical and demographic characteristics of these clinicians and patients were compared to the intervention arm of the trial. Family members were allowed to be present during the conversation.
All serious illness conversations between randomized intervention clinicians (N = 48) and patients (N = 134) were eligible for audio recording. We initially approached one out of every four clinician–patient dyads. Using this approach, our response rate was low, and we subsequently decided to approach every dyad. Dyads were approached by enquiring directly after randomization whether their conversation could be audio recorded. Informed consent was obtained and obtained again directly before the conversation. In addition, all patients with metastatic melanoma, as well as clinicians caring for these patients, were approached. Since these clinicians had received the same skills-based training as the remainder of the intervention group, we included them in the current analysis. In total, we obtained and included 25 conversations (19% of all possible conversations), conducted by 16 clinicians.
Data analysis
A multidisciplinary research team with expertise in psychiatry, palliative medicine, pulmonary and critical care medicine, oncology, and qualitative methods developed and iteratively revised a preliminary coding scheme based on the content and flow of the SICG. This coding scheme also included codes to capture particular aspects of these conversations (e.g., discussions revolving around life-sustaining treatments). A subset of codes detailing on the patient–clinician relationship were also included in the coding scheme (e.g., positive affirmation or ambivalence). The set-up of the conversation was not included in the analysis. A subset of four randomly selected transcripts were read and coded using this preliminary coding scheme and, throughout this iterative process, new codes were added to reflect newly emergent themes. Trustworthiness of the data analysis was ensured through having two independent coders, a senior experienced clinician with expertise in palliative medicine and psychiatry as well as an expert on qualitative research methodology. Dependability was further ensured through the iterative development of a coding scheme capturing various aspects of the conversation. Conformability of the findings was ensured by not having any research staff present during the conversations.
Two independent researchers (D.J.L. and O.P.G.) subsequently coded each transcript. Neither of these researchers had an established relationship with the study clinicians or patients. Because of the exploratory nature of the study, an inductive coding approach was used and additional emerging themes or codes could be added throughout the coding process. Disagreements were first discussed among the two researchers and, if needed, resolved through a verbal consensus discussion with a third, independent researcher (S.D.B.). Coding was performed using the NVivo 11 Pro (QSR International) qualitative data analysis software, and we adhered to the Consolidated Criteria for Reporting Qualitative Research checklist. 28 We assessed the percentage of words spoken by clinicians using a word count. This is a relatively crude estimation of the percentage of time spoken by each interlocutor and does not account for silences or other important forms of nonverbal communication throughout these interactions. Finally, clinicians also reported on the duration of the conversation directly afterward. This estimation was used to calculate the median duration of the conversations.
Results
Patient and clinician sample
Table 1 describes demographic and clinical characteristics of the patient sample (n = 25). Their mean age was 60.3 years (95% confidence interval [CI]: 54.3–66.5), 48% were female, all were white, and 48% of patients described their health as Relatively healthy and terminally ill. Table 2 describes demographic characteristics of the clinician sample (n = 16). Of these, 50% were female, most were physicians (69%), and physicians had an average 13.9 years of attending-level clinical experience. Characteristics of both patients and clinicians were compared to the remainder of the trial populations. This analysis revealed no statistically significant differences (data not shown) except for a lower percentage of patients insured through Medicare in the qualitative study sample (24% vs. 49%; p < 0.05).
Characteristics of Patients in the Qualitative Study Sample
These patients were part of a pilot trial and not included in the trial sample.
CI, confidence interval.
Characteristics of Clinicians in the Qualitative Study Sample
Description of conversations
A nurse practitioner or physician assistant conducted six conversations (24%) and physicians conducted the remainder. The median audio recorded duration of conversations was 14 minutes (range 4–37). On average, clinicians spoke 53% of the time (range 26%–70%), and 48% of clinicians directly asked the patient about any additional questions the patient had.
The final codebook contained 39 codes spanning seven topics (Supplementary Table S1). Our analysis revealed five key themes: (1) supportive dialogue between patients and clinicians; (2) patients' openness to discuss emotionally challenging topics with their clinicians; (3) patients' willingness to articulate preferences regarding life-sustaining treatments; (4) clinicians' difficulty in responding to emotional or ambiguous patient statements; and (5) challenges in discussing prognosis. We obtained data saturation after ∼22 conversations.
Supportive dialogue between patients and clinicians
Throughout most conversations, clinicians were quick to offer positive affirmation and demonstrated strong rapport with their patients by referring to their history together, joking, and asking questions about other family members:
Clinician: Yeah, well you have a terrific attitude, and it's definitely impacted how well you've done over the past five years. [Clinician #12]
Elements of such dialogue were also reflected through clinician reassurances, particularly as they pertained to talking with family members or other loved ones about disease status or progression. In most conversations, clinicians also reassured their patients and caregivers that patients would be kept as comfortable as possible throughout the disease process:
Clinician: Well, in terms of being in a lot of pain, we are sort of responsible for making sure that that becomes controlled. That we control that pain for you. And, and my job is to make sure that first of all, you know, you're safe. That's my biggest concern. [Clincian #7]
Although the language use and general tone of the conversations was interpreted as supportive dialogue, clinicians did not always adequately respond to emotional or ambiguous patient statements.
Patients' openness to discuss emotionally challenging topics
In the majority of conversations, patients offered open, personal, and direct responses to both questions of the SICG and clarifying questions beyond:
Clinician: … if your health situation worsens, what are your most important goals? Patient: That I don't make a fool of myself. That I handle it with dignity….You know, accept it, deal with it as best you can. Clinician: Have you found it difficult to accept? Patient: No, so far I've done it with some grace and good humor. [Clinician #13; Patient #20]
Only in one case did a patient specifically decline to answer a question by requesting a “pass.” Patients introduced the words “death” and “dying” more frequently than their clinicians, often in the context of talking about their fears (Umm…my biggest fear is, is dying. You know, basically, leaving my kids and my wife behind; Patient #22), or when describing their illness understanding. When asked about their most important goals, the majority of patients were realistic (You know, I'm not looking to climb Mt. Everest at this point; Patient #20). Most patients articulated the importance of being at home with family, making sure loved ones were provided for and not burdening others emotionally or financially:
Clinician: Do you have specific goals that you want to achieve? Patient: Just to spend time with the family. That's about it, you know. Uh, and be here as long as I can. I'm not looking for a miracle. I'm just looking for a little time. [Clinician #15; Patient #24]
Patients' willingness to articulate preferences regarding life-sustaining treatments
Preferences regarding life-sustaining treatments were discussed in most conversations (76%), although the SICG does not specifically address this. Of these 19 conversations, the topic was initiated more frequently by the patient rather than by the clinician. The majority of patients expressed a clear preference against the use of life-sustaining treatments:
Patient: I am not to be resuscitated… if I die, let me die. [Patient #13].
When articulating their specific preferences for or against such treatments, patients usually did so in response to the tradeoffs question: “If you become sicker, how much are you willing to go through for the possibility of gaining more time?” Patients also frequently used anecdotes related to past, personal experiences to justify such preferences:
Patient: I had somebody that I worked with and he had a massive stroke, and he can't do anything. Can't move, can't speak, you know, can blink his eyes, that's it. I don't think I'd want to… I wouldn't want to live like that. [Patient #4]
In response, several clinicians dissuaded the patient from making any decisions regarding the use of life-sustaining treatments at this time because their health status was too good or because preferences change and patients might feel differently in the future:
Clinician: This is not anything permanent right now that we're talking about. Patient: Right. Interviewer: This is more kind of to get the ball rolling… Patient: Yeah. Clinician: And you're in such wonderful health now! [Clinician #8; Patient #13]
Clinician: Because I think you're actually healthy enough that… as an otherwise healthy, what, sixty-seven year old? I don't know. So why don't you think about that and next time you come back we can talk about it again.
[Clinician #9]
Furthermore, among the patients who expressed their preferences regarding life-sustaining treatment, only one was encouraged to complete an AD or similar legal documents.
Clinicians' difficulty in responding to emotional or ambiguous statements
In the majority of conversations, patients explicitly stated that they understood their disease to be incurable. Several patients however, did articulate their hope for a cure or described that they thought their disease was in remission. In some of these cases, clinicians attempted to reframe a patient's expectations:
Patient: Well, I guess it's in remission. Which is good news. So, that's as much as I know. Clinician: Well, I think remission might be the wrong word. Patient: The wrong word. It's “holding steady,” I probably should've said [Patient #14]
In other conversations, rather than exploring or reframing their patient's (mis)understanding, clinicians expressed optimism or did not follow-up on such statements:
Patient: How I'm progressing, is it pretty…it's pretty standard? Clinician: Oh no. You're doing outstanding. You're outstanding. You're doing great! [Clinician #4; Patient #6].
Patients frequently expressed emotions or alluded to the struggles of facing a serious illness. Such statements, either implicitly or explicitly, revealed patients' unmet informational needs, emotional distress, or uncertainty about their current or future health status, QoL, or treatment. Clinicians' responses were frequently limited to “Okay” or “Uh huh” or clinicians did not explore such statements further:
Clinician: We'll mostly focus today on, you're in great shape! Patient: Right. Clinician: How can we keep you in great shape? Patient: So, I've been thinking of the other, inevitable, as well… Clinician: Okay, good. [Clinician moves on] [Clinician #3; Patient #5]
Patient: Quality of life is much more important to me than longevity.
Clinician: Okay.
Patient: I want both.
Clinician: I know… and we're working to give you that… but um…
Patient: I know that… I know that.
[Clinician #1; Patient #1].
Challenges in discussing prognosis
Out of the 25 conversations, 2 patients explicitly stated that they did not want to receive any information about what was likely to be ahead with their disease as illustrated below:
Patient: Personally I like taking things a step at a time. So, I guess my feeling is that I don't like to be projecting too far ahead. I realize the outcome probably will be grim at some point. But I think the business of working with it as it is, at least in my mind, satisfying. [Patient #18]
All other patients either wanted to be fully informed (72%) or receive some information but not all (20%). Subsequently, clinicians disclosed prognosis, as recommended in the SICG and reinforced in the skills-based training, in 10 of the conversations. When broaching the topic of prognosis, both clinicians and patients often expressed a need for optimism. Of those clinicians who provided a prognosis, only three provided a time-based estimate of prognosis (e.g., how long the patient is expected to live). Instead, clinicians commonly focused on future treatment options, often in relatively lengthy monologues containing highly medical language:
Clinician: Then there are subgroups of patients, and then one of the subgroups that has a better and more favorable prognosis are those patients with the EGFR mutations and so, and we do know that their, their median survivals in places like here… those are the people we now hope our patients can be. And then there are some patients that have those much more slowly growing cancers, and then we don't know whether you're going to fit into that fourth category in terms of a response […] We've seen the metastases to the brain and so that's telling us that it's probably not one of those very, kind of indolent lung cancers. It's been in the lungs for many, many years, but we don't know, yet, because you haven't had the EGFR inhibitor, whether you're gonna be one of the group that can have a more prolonged response to those kind of certain things. [Clinician #10]
In other cases, clinicians described an uncertain prognosis, characterized by disease that could remain stable, other medical problems that could ensue, or details on how the cancer could suddenly progress and lead to complications. The likelihood of various trajectories, however, was often not addressed:
Clinician: The scan today, compared with the one from four months ago, shows very little change, and, that's great, it is possible that you could be alive for years in this state. In this current state is it possible something bad could happen—could it spread to another site, you know, the brain? Similar to that, a bleeding into the tumor, or, small vessel rupture related to the tumor, those things could happen. It could take your life, you know, much more rapidly? But of course, people of your age could have a stroke, as well. These things could happen, also, independent of your cancer. [Clinician #7; Patient #11; Age 77]
Finally, a minority of clinicians, although articulating that the disease was indeed incurable, used ambivalent and confusing language to do so:
Clinician: No, it's good. I mean, you do have stage 4 disease, that's never gonna change. Patient: Right. Clinician: But after you had that surgery recently… that rendered you disease-free. Patient: Right. Clinician: So, your stage 4 is no evidence of disease. [Clinician #8; Patient #13]
Discussion
The aim of the current study was to provide a descriptive overview of serious illness conversations conducted using a structured conversation guide. Our analysis of 25 audio-recorded and guide-led serious illness conversations between oncology clinicians and patients with advanced cancer revealed several insights. First, among these is the warmth and comfort of patient–clinician relationships. Clinicians in our sample provided space for patient-centered conversation and focused on what was important to patients, as supported by the finding that clinicians spoke approximately half of the time. Furthermore, their patients appeared to be open to discussing emotionally challenging topics and usually had clear preferences regarding their future care. Previous literature has suggested that similar conversations either do not take place, happen late in the disease course, or focus primarily on symptom control and preferences regarding life-sustaining treatments, while failing to adequately address patients' personal values and goals.9,29–31 We found that training and a systematic framework allows clinicians to engage in these challenging conversations, provides space for patients to express their thoughts and feelings, and explores basic values and QoL-issues while engaging patients in planning for the future.
Yet, we also demonstrated that clinicians, despite (or because of) their warm and comfortable relationships with their patients, frequently did not meet this standard, especially when discussing prognosis. Emotional discomfort on part of both the clinician and patient is likely to contribute to this pattern. Moreover, clinicians sporadically followed up with patients about their expressed preferences regarding life-sustaining treatments. Discussing the future with seriously ill patients can be an emotional experience, and often elicits anxiety, sadness, and fear.3,9,32,33 Because clinicians experience strong positive feelings for their patients, they too may experience distress when discussing these issues.34,35 Clinicians' emotional discomfort may manifest as avoidance, ignoring the patient's concerns, or excessive optimism.36,37 Although clinicians may avoid these discussions to be kind or protective, such avoidance may lead patients to feel isolated with their concerns, or contribute to care that misaligns with patient preferences. 34
Furthermore, we observed a prognostic discussion in approximately half of the conversations and few clinicians provided patients with a time-based estimate (12%) even though the skills-based training suggested that clinicians tailor their prognostic disclosure to individual patient preferences. Instead, clinicians primarily focused on treatment options or discussed prognosis indirectly. Previous, predominantly quantitative research, has shown that clinicians regularly fall into one of the following pitfalls when communicating a patients' prognosis: excessive optimism, a focus on medical treatments without conveying a specific time-estimate, or the use of vague language to avoid distress in patients or caregivers.26,38,39 These behaviors may reflect previous findings that over 70% of medical oncologists report inadequate or no communication training on prognostic disclosure and 88% feel ill-equipped to conduct these conversations. 38 Nonetheless, nearly all (96%) do believe that it should be part of their training.40,41
Discussing prognosis with patients does not appear to be intrinsically harmful to the patient–clinician relationship and may even strengthen therapeutic alliance. 42 Although not a new observation,43,44 this suggests that disclosing a time-based prognosis may be challenging and might lead us to think about different ways to train clinicians (e.g., by framing prognosis as a worry about functional decline or concerns about an unlikely, but possible rapid deterioration without time for future planning). Such ways could allow clinicians to better tailor the type of prognostic disclosure used to individual patient preferences. In addition, clinician need training in specific communication competencies focused on: (1) titrating difficult information to in-the-moment observations of the patient's emotional responses to avoid burdening patients with emotionally overwhelming information that can be more than desired, or for which the patient is not ready, 45 and (2) discussing uncertainty in ways that acknowledges realities and supports appropriate hope. We think of both of these key clinical competencies as “gentle directness.”
Our findings should be viewed in light of a self-selection bias since both patients and clinicians had to consent twice before the audio recording of the conversations. It is thus likely that patients in this subsample may have been more comfortable talking about these issues than other patients and were well prepared by the consent process to have the conversation. We also assume that clinicians who consented to be audio recorded might be more comfortable than those who did not; the behavior we observed here may therefore be a relatively positive representation of how clinicians conduct such conversations. In this analysis, the lack of a control group in which clinicians were not trained and did not use the SICG precludes conclusions about how conversations may have been similar or different without the intervention. Furthermore, patients were drawn from a single institution, predominantly highly educated and white. Cultural or racial factors are important during these interactions,46,47 but could not be adequately explored in the current study.
Despite these limitations, this study has several strengths. Our analysis resulted in thematic saturation before we had analyzed 25 conversations thereby making it unlikely that we missed key themes. 48 Furthermore, although we were unable to capture nonverbal communication through video, these audio recordings provide a great deal of information about what happens in a real clinical encounter. All clinicians in this study received the same skills training, and most adhered to the systematic structure of the SICG. This allowed us to compare a group of relatively homogeneous conversations and to more closely examine variations in how the conversation topics were handled by the clinicians and patients. 49
If our findings are supported by further research, they suggest several pathways to improving care. Patients generally expect their clinicians to initiate serious illness discussions. 39 Although some clinicians fear that these conversations might “take away hope” or be distressing for patients, 24 patients in our study responded positively to the questions in the SICG and frequently initiated conversation about difficult and personal topics. If clinicians ask appropriate, open-ended questions, patients may perceive that their clinicians are more open to other patient-initiated conversation and be more willing to bring up their concerns and preferences.
In conclusion, the clinicians and seriously ill patients in our study were receptive to, and engaged by, conversations in an outpatient setting using a structured framework. Moreover, the quality of these conversations is aligned with expert recommendations to use open-ended questions, focus on basic values and goals, and for clinicians to speak no more than half the time. Yet, even when clinician–patient relationships are strong and conversations adhere to these standards, clinicians still experienced challenges in sharing prognostic information aligned with patient preferences, addressing emotions, clarifying concerns and preferences, and in following up on treatment limitations. Further research to better understand the mechanisms behind such challenges may enable clinicians to evolve such skills and help develop new approaches to deliver high-quality, serious illness care.
Footnotes
Acknowledgments
We are deeply grateful to all patients, family members, and clinicians who have provided their time and support to this study.
Author Disclosure Statement
Dr. Susan Block is employed by UpToDate as an editor for their Palliative Care section. All other authors have no conflict of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.