
Abstract
Background:
Little is known about the provision of palliative care to people with dementia (PWD).
Objective:
To examine demographic and clinical characteristics of PWD versus nondementia serious illnesses receiving community-based palliative care.
Design:
Retrospective study of people 65+ receiving an initial consultation from a community-based palliative care practice between September 2014 and February 2018 using registry data entered by clinicians into the Quality Data Collection Tool for Palliative Care.
Setting:
Large not-for-profit organization that provides community-based hospice and palliative care services.
Measurements:
Demographics, consult characteristics, advance care planning, and caregiver support.
Results:
Of 3883 older adults receiving a first palliative care consultation from this organization, 22% (855) had a dementia diagnosis. Compared to those with nondementia serious illnesses, PWD were older with more impaired function; 36% had a prognosis of less than six months. More PWD than those without dementia had a proxy decision maker and documented advance directive. A quarter of PWD were full code before consultation; nearly half changed to some limitation afterward. Symptom characteristics were missing for 67% of PWD due to collection through self-report. Caregivers of PWD were responsible for significantly more activities of daily living than caregivers of people with nondementia serious illnesses.
Conclusions:
This is the first comparison of a large cohort of people with and without dementia receiving a community-based palliative care consult in the United States. Alternative measures of symptom burden should be used in registries to capture data for PWD. Understanding the unique characteristics of PWD will guide future services for this growing population.
Introduction
Over 5.7
International consensus recommends a palliative care approach for dementia, and PWD increasingly receive specialty palliative care services.3–7 At end of life, PWD often receive palliative care through hospice: 18% of Medicare hospice beneficiaries had a principle diagnosis of dementia in 2016. 8 In Veterans Affairs (VA) inpatient settings, 61% of PWD who died received palliative care consults. 9 Outside of the VA, however, little is known about the receipt of palliative care by PWD. The provision of palliative care is not consistently captured through claims data, so nationally representative secondary datasets like Medicare claims, Health and Retirement Study, or National Health Aging and Trends Study have limited or no reliable means to identify people who receive specialty palliative care consultations across care settings. 10 Registries that collect data on palliative care services and quality 11 are currently the principal way to obtain reliable data on receipt of palliative care.
Payers, policymakers, and palliative care organizations need to understand the characteristics of PWD entering palliative care, particularly as they differ from those without dementia, to assess and tailor palliative care services for this growing population. This study aimed to describe older adults with dementia who received palliative care and compare these to older adults with nondementia serious illnesses. To do so, we used registry data collected during initial palliative care consultations from a large community-based organization that provides palliative care and hospice services in all care settings.
Methods
Design
We conducted a study of all patients age 65 and older who received an initial palliative care consultation between January 1, 2014 and February 28, 2018 from Four Seasons Compassion for Life, a large community-based organization that provides specialty palliative care and hospice services. Patients with a diagnosis type of “dementia” were compared to patients with nondementia diagnoses.
Analyses used deidentified data collected using the Quality Data Collection Tool for Palliative Care (QDACT-PC), a web-based point-of-care quality assessment and reporting tool designed for providers to enter data that they observe or that patients report during palliative care clinical encounters. QDACT-PC includes real-time graphics-based feedback (e.g., a color-coded system reflecting high levels of unmet need for a particular symptom), ability to report more than 80% of all published palliative care quality measures, and aggregation into a centralized registry. 12 QDACT-PC was developed in collaboration with providers at the study site starting in 2008, tested for usability and acceptability, and subsequently expanded into more than 13 community and academic settings across the United States.11–14 The University of California, San Francisco Institutional Review Board considered this study to be exempt research as it used deidentified data.
Setting
Four Seasons provides care in eleven predominately rural counties in Western North Carolina. The standardized palliative care program serves people of all ages in homes, outpatient clinic, long-term care facilities, and three small community hospitals and captures data on care provided in QDACT-PC. 15 The initial visit involves a palliative care-trained physician or nurse practitioner conducting a history and physical examination, symptom and medication review, functional assessment, discussion of goals and advance care planning, screening for spiritual and psychosocial needs, and assessment of caregiver burden and needs.16–18
Sample
Three thousand eight hundred eighty-three adults age 65 and older were enrolled in the Four Seasons palliative care program during the study period. Of these, 855 individuals had a diagnosis of dementia; 3028 had no dementia diagnosis and included those with nondementia neurologic disorders (e.g., Parkinson's disease and stroke). Older adults with no dementia diagnosis had the following top 5 primary diagnoses: heart failure (15.5%), chronic obstructive pulmonary disorder (13.1%), metastatic cancer (11.1%), pneumonia (8.7%), and stroke (8.5%).
Measurements
Sociodemographic variables included age at initial encounter, gender, race, marital status, and primary insurance type.
Palliative care consult characteristics included consult location: home, hospital, long-term care facility, or other (outpatient clinics, palliative care units, “other”). Functional status was assessed using the Palliative Performance Score (PPS), 19 which is an indicator of prognosis and illness severity and incorporates evidence of declining physical function, engagement in activities, oral intake, and cognition 20 (PPS categories: 10%–30%, 40%–60%, and 70%–100% 21 ).
Variables relevant to advance care planning included clinician-estimated prognosis of survival (hours to days, days to weeks, and one to six months combined and compared to greater than six months), relationship of health care proxy to patient (grouped as child, spouse or significant “other,” and other family or friend, parent, legal guardian, or other), advance directives, code status before consult (“full code,” indicating the use of all life-saving measures, compared to limitations like “do not intubate; DNI” or “do not resuscitate; DNR”), code status change, and code status after consult.
Caregiver variables represent family, friends, or proxy decision makers that interacted with the palliative care specialists or that the patient or proxy reported was involved in providing care in any care setting (grouped as family member, friend/guardian, multiple people, or missing data). We examined caregiver responsibilities from a list of five activities of daily living (ADLs) and nine instrumental activities of daily living (IADLs). In a subanalysis we stratified caregiver variables by location of care consult. We also evaluated a variable where the provider indicated that the caregiver had asked for or received help from others (caregivers both asked and received help vs. those who either did not ask or asked and did not receive help).
Edmonton Symptom Assessment Scale (ESAS) questions ask patients to self-report on their experience of each of 10 symptoms, rated on a scale of 0 (none) to 10 (most severe).22,23 We created three categories of ESAS answers: unable to respond, scores of 0–4 “no or mild symptoms,” and scores of 5–10 “moderate to severe symptoms.” Missing data are presented for all variables; they include, for example, “patient does not wish to answer” or “unknown,” unless otherwise noted.
Statistical methods
Patient-specific characteristics were summarized with means and standard deviations for continuous measures or tabulations and percentages for categorical variables. Univariate associations between diagnosis and patient characteristics were examined using nonparametric Wilcoxon tests (continuous variables) or chi-square tests (categorical variables) using SAS Version 9.4.
Results
Compared to older adults with nondementia serious illnesses, more of those with a diagnosis of dementia were older (57% age 85 and older vs. 39%, p < 0.001; not shown) or female (71% vs. 58%, p < 0.001); racial/ethnic distributions did not differ (Table 1). While over 90% of the sample used either Medicare Part B or Medicare Advantage as their primary insurance, PWD were less likely than those with nondementia serious illnesses to use Medicare Advantage or other sources such as Medicaid, Government, commercial insurance, or self-pay (p = 0.007). At the time of the initial consultation, PWD had greater illness severity as indicated by PPS of 30% or less (24% vs. 20%). In addition, PWD were more likely to receive the initial consultation in a long-term care facility setting (62% vs. 30%), while those with nondementia serious illnesses were more likely to receive their initial consultation in the hospital (50% vs. 17%); a similar portion of PWD as those with nondementia serious illnesses were seen at home (13.3% vs. 13.6%).
Demographic and Consult Characteristics of Older Adults at Initial Community-Based Palliative Care Consult, Comparing Diagnoses of Dementia and Nondementia Serious Illness
Based on Mann-Whitney test.
Based on chi-square test.
Other sources of insurance include Medicaid, government insurance such as Veterans Affairs or Federal Employees Program, Commercial Insurance such as Blue Cross Blue Shield, and Self-Pay.
Hospital settings include emergency department, intensive care unit, and general floor; long-term care facility settings include long-term acute care, skilled nursing rehabilitation, assisted living facilities, and nursing homes. Other settings include outpatient clinics, palliative care units, or “other.”
Palliative Performance Score range 0 (dead) to 100% (full independent function).
SD, standard deviation.
Relevant to anticipatory guidance and decision support, clinician-estimated prognosis and presence of decision-making proxies were similar between PWD and those with nondementia serious illnesses (Table 2). Thirty-four to thirty-six percent of the sample had a prognosis of less than six months (p = 0.011). Ten to twelve percent did not have a proxy or had missing proxy data. Those with dementia were more likely to have a child serving as proxy (53% vs. 45%, p < 0.001) and more likely to have a documented advance directive (50% vs. 36%, p < 0.001). They were less likely to have had full code status before the consult (26% vs. 41%, p < 0.001). However, among all older adults with a preference for full code before the consult, nearly half changed their preference to some limitation (e.g., DNI or DNR) after the consultation (105 of 219 individuals with dementia; 579 of 1253 individuals with nondementia serious illnesses).
Advance Care Planning Characteristics of Older Adults at Initial Community-Based Palliative Care Consult, Comparing Diagnoses of Dementia and Nondementia Serious Illness
Based on chi-square test.
Limitations include DNR/DNI, DNR not DNI, DNI not DNR, mostly DNR/DNI with other documented limitation, or other specified.
DNI, do not intubate; DNR, do not resuscitate.
Using the approach standardized in QDACT, clinicians used patient-reported outcomes to assess symptoms during the initial palliative care visit (Fig. 1). For more than two-thirds of PWD (67%) symptom data for all 10 questions within the ESAS were missing or marked “unable to respond”; in many cases, “unable to respond” was marked once and missing for all other symptom data. By comparison, only 24% of older adults with nondementia serious illnesses lacked information for all measures (p < 0.001). The level of combined missing and “unable to respond” responses on individual ESAS items ranged from 59.9% to 88.2% for individuals with dementia versus 21.4%–54.1% for those without.
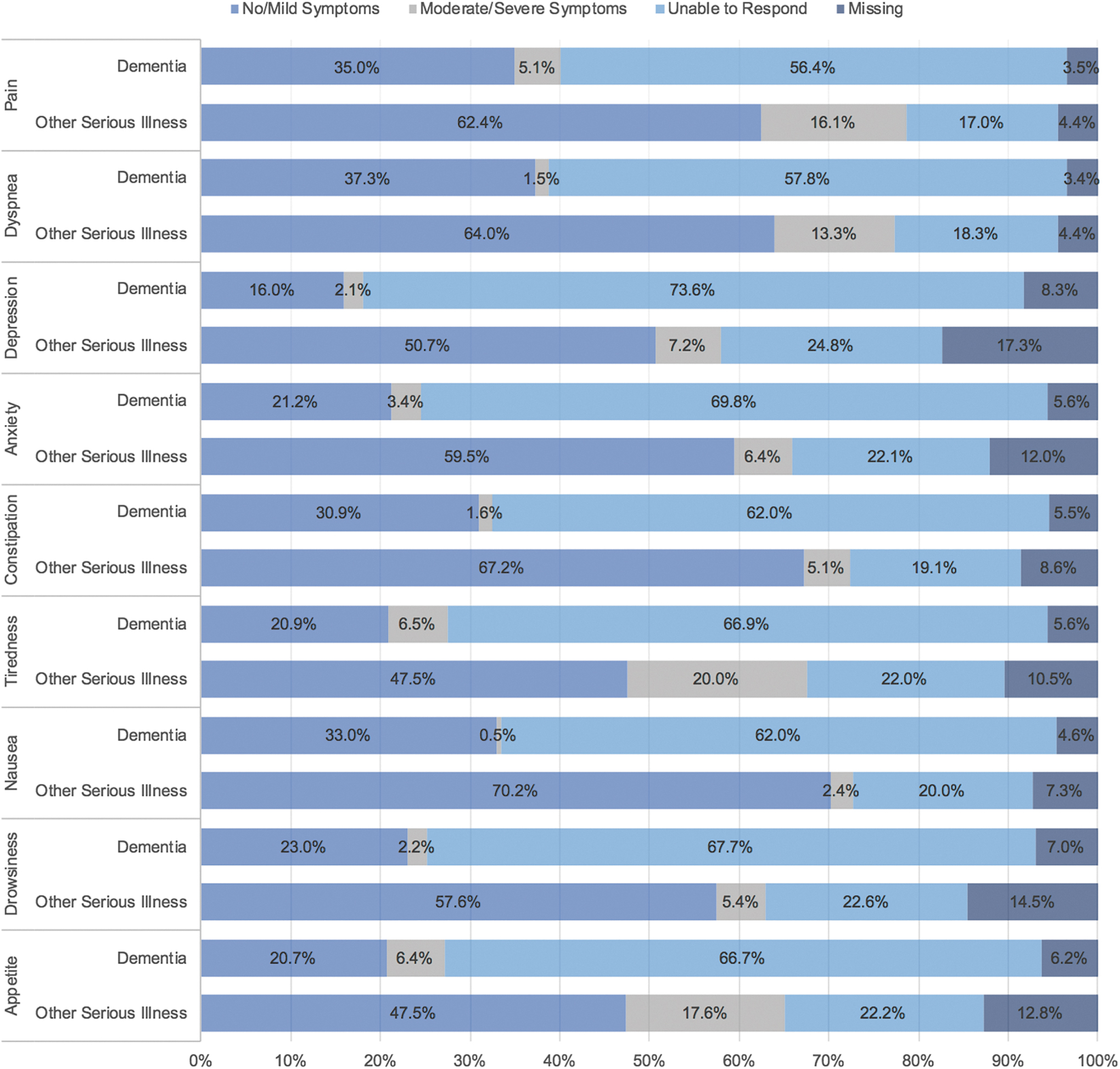
Patient-reported symptoms of older adults at initial community-based palliative care consult, comparing diagnoses of dementia and nondementia serious illness. Using the ESAS, clinicians ask a person to rate each of 10 symptoms on a scale of 0 (no experience of symptom) to 10 (most severe experience) or enter “patient unable to respond.” Some patient data show “patient unable to respond” for some ESAS questions and numeric data for others. In these cases, providers may have used their clinical judgment to make an estimate of symptom scores although the patient was cognitively unable to self-report. While clinicians are asked to enter data for each item, the system does not require answers, so in some cases “unable to respond” may be entered for one or two questions but left missing for the remainder. ESAS, Edmonton Symptom Assessment Scale.
Caregiver involvement was reported for 7 in 10 in the entire sample; the remainder had missing data (Table 3). Caregivers, usually one family member (60%), provided assistance with IADLs and ADLs for 64% of the sample. More IADL responsibilities were listed for caregivers of PWD than for their counterparts (mean 4.0 IADLs [SD: 2.8] vs. 3.5 [SD: 2.4], p = 0.009). Findings were similar for ADL responsibilities (mean 1.1 ADLs [SD: 1.8] vs. 0.7 [SD: 1.4], p < 0.001). Caregivers of PWD were more likely to be responsible for IADLs like decision making (60% vs. 45%, p < 0.001) and finances (46% vs. 29%, p < 0.001) and ADLs like dressing (17% vs. 12%, p < 0.001) and bathing (17% vs. 12%, p < 0.001; Fig. 2). Caregivers of PWD were also significantly more likely to have asked for and received help from others (30% vs. 26.5%, p = 0.002).
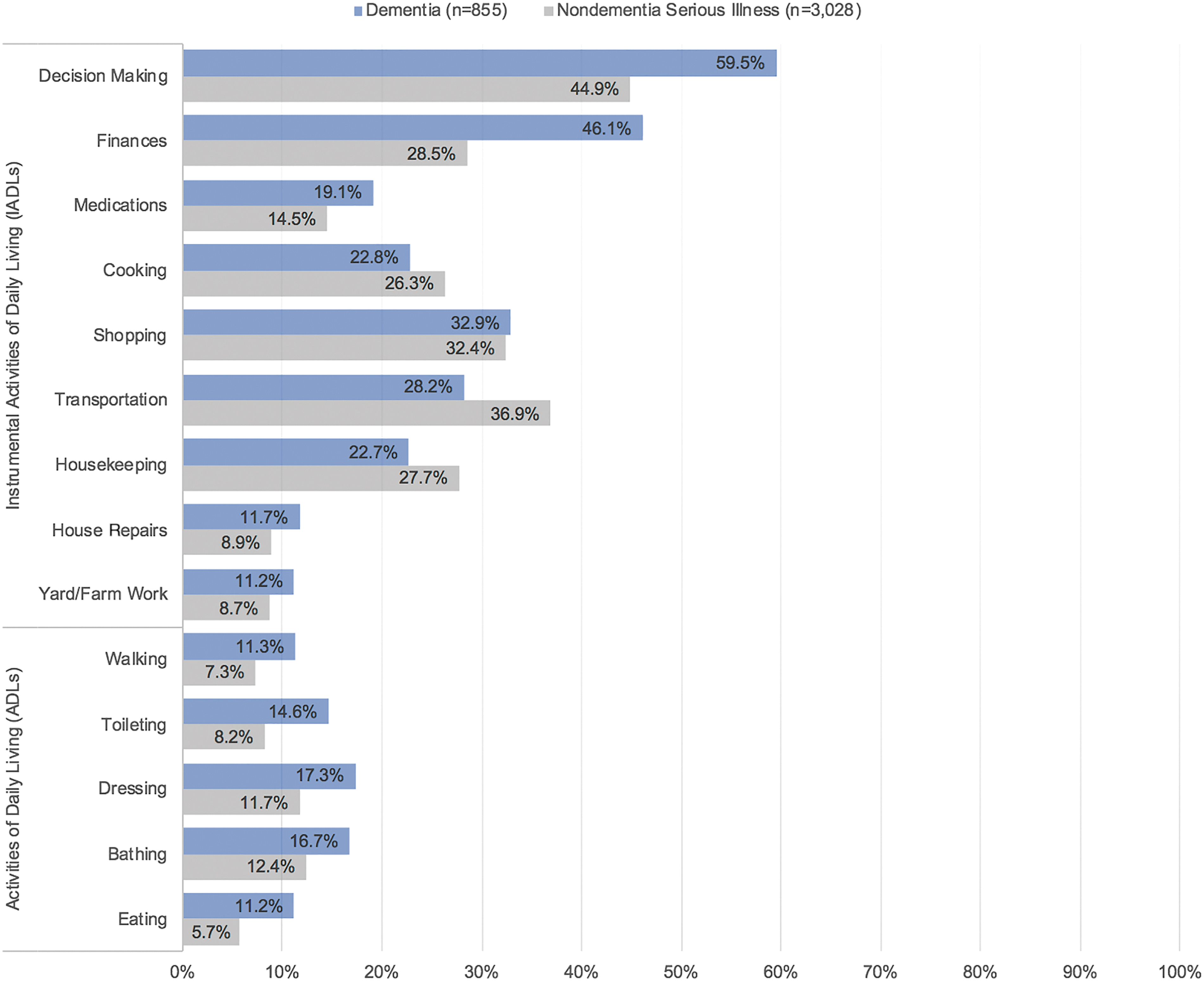
Caregiver responsibilities for providing assistance with IADLs and ADLs for older adults reported at initial community-based palliative care consult, comparing diagnoses of dementia and nondementia serious illness. All comparisons between older adults with dementia were significant at p < 0.05 with the exception of the shopping variable. ADLs, activities of daily living; IADLs, instrumental activities of daily living.
Caregiver Presence and Activities for Older Adults at Initial Community-Based Palliative Care Consult, Comparing Diagnoses of Dementia and Nondementia Serious Illness
Based on chi-square test.
Includes those who indicated caregiver help with one or more specific ADL/IADL activities.
Based on Mann-Whitney test.
ADLs, activities of daily living; IADLs, instrumental activities of daily living; SD, standard deviation.
Analyses stratified by care setting indicate similar rates of caregiver presence for PWD and nondementia serious illness in the home (82% dementia, 82% nondementia), hospital (89% dementia, 81% nondementia), and long-term care (58% dementia, 59% nondementia; data not shown). In each setting the majority of caregivers provide help with IADLs or ADLs, but more help is provided in home settings: caregivers of PWD helped with a mean of 7.0 IADLs and 2.9 ADLs in the home and caregivers of people with nondementia serious illness helped with 5.3 IADLs and 1.5 ADLs. By contrast, caregivers of people in long-term care helped with a mean of 3.6 IADLs and 0.8 ADLs for PWD and 3.6 IADLs and 0.7 ADLs for people with nondementia serious illness.
Discussion
Our study provides insight into the characteristics of older adults with dementia who received an initial palliative care consult from a large community-based palliative and hospice care organization. Using a dataset of palliative care services, this represents the largest U.S. based study of this kind to date. We found that compared to those without dementia, PWD were more likely to receive an initial palliative care consult in a long-term care facility (65%), were significantly older, and had more severe illness. They were also significantly more likely to have a proxy decision maker, documented advance directive, and preference for resuscitation limitations. We could not compare symptom burden as QDACT-PC currently only includes patient-reported symptom assessment measures; 67% of those with dementia had missing data on all symptom measures. As expected, despite similar rates of caregiver presence in every care setting, caregivers of PWD were responsible for significantly more activities than were caregivers of older adults with nondementia serious illnesses. This finding was most dramatic among people receiving palliative care consults at home. Although not unanticipated, this is, to our knowledge, the first time the difference in caregiving responsibilities has been documented in palliative care registry data.
Our findings provide a first step to understanding the characteristics and needs of individuals with dementia and their caregivers as they begin to receive palliative care compared to individuals without dementia. Our research suggests that PWD are encountering palliative care during late-stage disease. One in four older adults with dementia in our study had a PPS 20 of 30% or less, and 36% had a prognosis of less than six months, indicating that they may have been hospice eligible. Studies have indicated that specialty palliative care is beneficial to individuals with late-stage dementia24,25 but its effect is not yet known for those at earlier stages. Providers like neurologists could address basic palliative care needs of PWD earlier in the disease process, but they are often not well-versed in palliative care and may lack confidence in communicating prognosis and eliciting treatment preferences. 26
This study highlights the limitations of advance care planning among PWD and their families. It is unsurprising that PWD in this study had higher rates of documented advance directives compared to those with nondementia serious illness and compared to their community-dwelling counterparts nationally. 27 The study setting had qualities associated with higher rates of advance care planning (older, more educated, affluent, and white 27 ). Moreover, nearly 80% of PWD in our sample received consults in facility settings (hospitals or long-term care) where advance directive documentation is required upon admission; palliative care consultations may have been requested by facilities for the express purpose of clarifying and documenting goals of care. Yet only half of PWD in our sample had a documented advance directive at the time of initial consultation, and one in ten was no longer able to complete the form. Moreover, the finding that nearly half of PWD shifted from full code to greater resuscitation limitations during the initial palliative care consult suggests that their documented plans no longer matched their preferences. Engaging palliative care earlier in the course of dementia to discuss care goals and preferences may facilitate the meaningful involvement of PWD before capacity declines and support the timely initiation and documentation of advance care planning. These steps may help PWD remain in the community until death to realize less aggressive and less expensive care at end of life. 28
Our study also highlights that using patient-reported symptom assessments alone results in substantial amounts of missing data for PWD. While patient-reported outcome measures are used to ensure patient-centered research and clinical practice, 29 such initiatives systematically exclude PWD who cannot self-report. Studies using self- or proxy-reported measures have identified meaningful symptom burden among PWD, yet these measures are not included in existing registries.30,31 In the future, registries capturing data on palliative care should include measurement tools designed for direct observation of nonverbal signs of symptom distress and validated for all types of dementia syndromes.32,33 This will ensure that registry data can be used to understand the full scope of palliative care needs (for clinical or research purposes) for PWD.
This descriptive study has specific strengths. It reflects data from a single standardized and published model of palliative care, in contrast to prior studies that used registry data across organizations with heterogeneous models of palliative care. 15 Analysis of registry data is currently the only way to examine palliative care consults received by older adults across all possible care settings and multiple insurance types because there is not a specific or consistently-used billing code for palliative care. These data therefore offer one of the only sources for critical information to more accurately characterize palliative care recipient needs and expand services. Other strengths of registry data include the ability to examine palliative care directly with both patient-reported and provider-observed data and inclusion of all insurance types.
Study limitations include the fact that registry-based datasets include fewer variables and higher rates of missing data than data sources like claims data or nationally representative surveys. The QDACT-PC registry dataset did not include information such as the specific type of dementia syndrome, degree of cognitive impairment or disease severity, reason for palliative care consult request, or other clinical variables that provide prognostic guidance. In addition, the data represented individuals within one large hospice and palliative care organization. This means some findings may not be nationally or internationally generalizable, particularly to populations with greater socioeconomic, racial, or ethnic diversity or with different levels of access to long-term services and palliative care. Compared to national data, our sample has a higher prevalence of PWD (22% in our study vs. 9.9% among community-dwelling Medicare beneficiaries 34 ) and higher prevalence of people age 85 and older with dementia (57% age ≥85 in our study vs. 37% of people with Alzheimer's dementia nationally 1 ). Finally, caregiver data (along with all other data) were provider reported rather than patient- or proxy reported, which may have yielded inaccuracies. However, as the largest examination of community-based palliative care consultations provided to a population of PWD in the United States, and as a study situated in a more rural setting than is typically studied, this study represents an important step forward in describing this model of care.
In summary, this study provides an important step in describing the characteristics and needs of PWD compared to people with nondementia serious illnesses. More work is needed to understand how the patterns demonstrated in this study relate to other regions of the country and more urban or more rural settings. A better understanding of the characteristics and needs of this growing population is essential for developing evidence-based dementia palliative care interventions. This work has begun in nursing home settings35,36 where population needs are better described,37–39 but substantial gaps remain for PWD living in residential homes and other community settings. Finally, this study identifies a profound need for more effective, appropriate, and validated tools to measure palliative care needs among verbal and nonverbal PWD. Future trials of dementia palliative care interventions will require patient- and family-centered outcomes to assess the impact and optimal timing of palliative care across multiple care settings.
Footnotes
Disclaimer
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. The funders had no role in development of the study, data acquisition, data interpretation, writing, or editing of article.
Funding Information
Four Seasons received a Centers for Medicare and Medicaid Innovation award in 2015 to standardize and develop a payment model for their model of community-based palliative care; this award provided additional support for data collection and service capacity. Analyses were conducted with support from the National Center for Advancing Translational Sciences, National Institutes of Health, through UCSF-CTSI Grant UL1 TR000004. K.L.H's time was supported, in part, by a National Institute of Aging-funded Reserach Fellowship (T32AG000212); Atlantic Fellowship of the Global Brain Health Institute; UCSF Hellman Fellows Award; pilot award from the UCSF Claude D. Pepper Older Americans Independence Center funded by National Institute on Aging (P30 AG044281); Career Development Award from the National Center for Advancing Translational Sciences of the NIH (KL2TR001870); National Palliative Care Research Center Junior Faculty Award; and National Institute of Aging Mentored Research Scientist Development Award (K01AG059831).
Author Disclosure Statement
No competing financial interests exist.