
Abstract
Dear Editor:
The availability of palliative care services in the United States has increased, yet the uptake of palliative care remains disproportionately low for socially vulnerable patients with serious illnesses. This is, in part, due to persistent institutionalized barriers to care that hinder the acceptance of palliative interventions even when they are available. 1 The health care system unilaterally determines when, where, and how medical services can be accessed. Barriers include (1) a lack of accommodation for atypical living situations, cultural traditions, or family circumstances, (2) untenable out-of-pocket expenses or restricted insurance coverage, and (3) limited access, resulting in low acceptability. 1 Lack of access can reinforce deeply held mistrust of the health care system and often leads to delays in care seeking. Consequently, even when palliative care services exist, we as providers fail to engage socially vulnerable patients in palliative care programs, leaving them with a high burden of physical and emotional suffering.
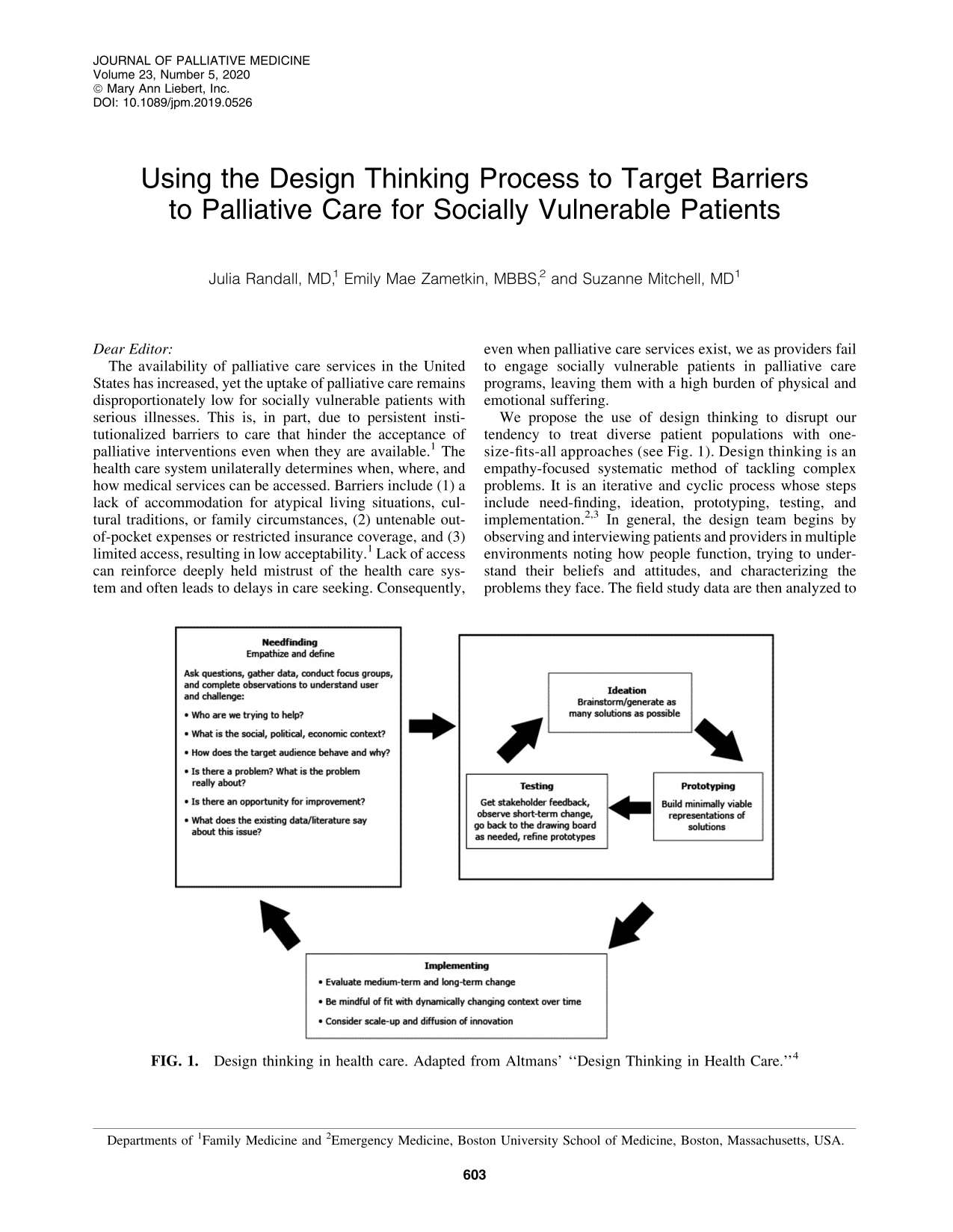
We propose the use of design thinking to disrupt our tendency to treat diverse patient populations with one-size-fits-all approaches (see Fig. 1). Design thinking is an empathy-focused systematic method of tackling complex problems. It is an iterative and cyclic process whose steps include need-finding, ideation, prototyping, testing, and implementation.2,3 In general, the design team begins by observing and interviewing patients and providers in multiple environments noting how people function, trying to understand their beliefs and attitudes, and characterizing the problems they face. The field study data are then analyzed to inform and reframe the precise problem statement that the team aims to address.2,3 The focus is on a population's unique attributes rather than deficits. For example, with a homeless population, focus is shifted from deficits such as mental illness or substance use to attributes such as advanced ability to problem solve, make quick decisions, in-depth knowledge of local geography, and strong social networks.
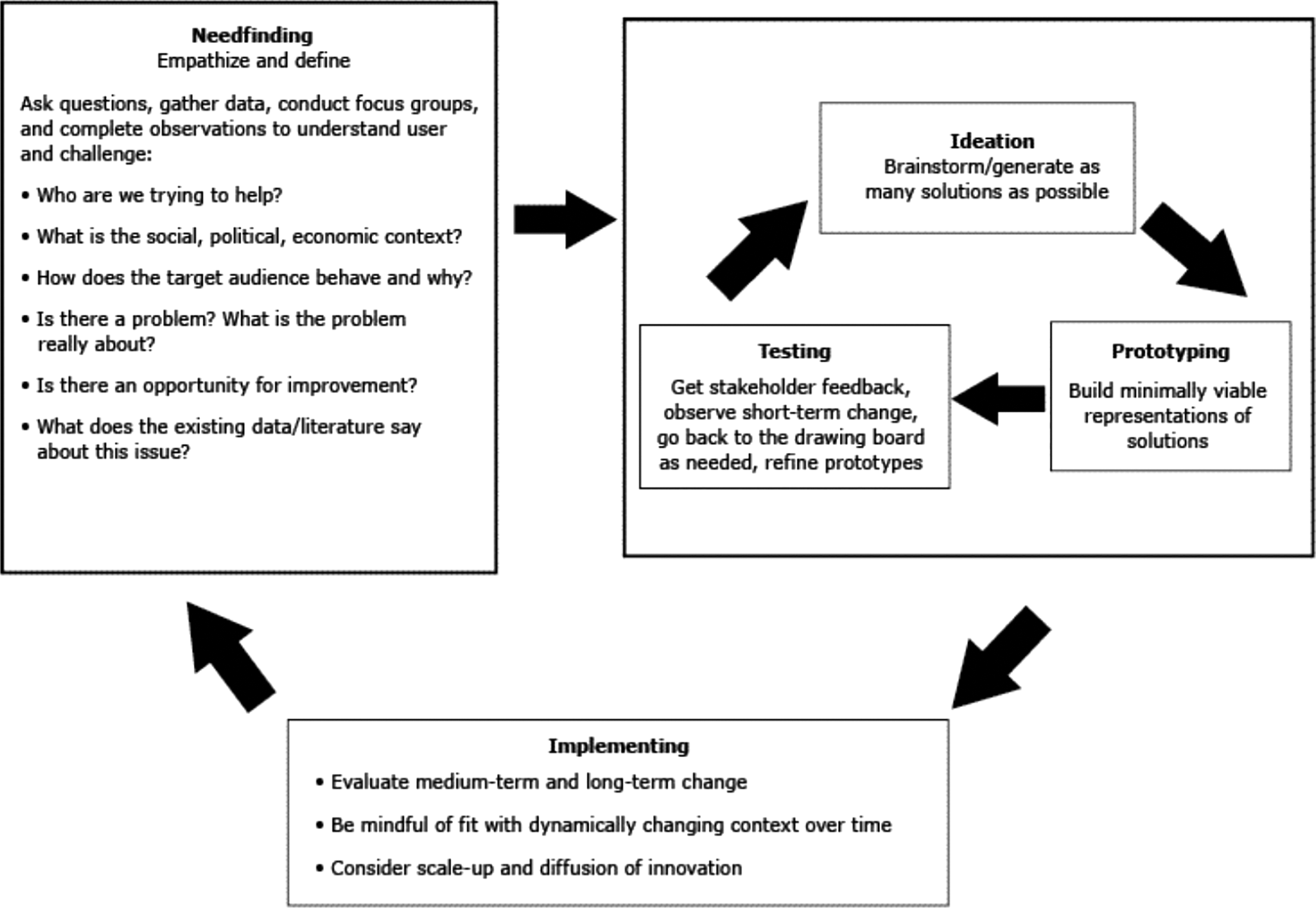
Design thinking in health care. Adapted from Altmans' “Design Thinking in Health Care.” 4
The team then brainstorms solutions to address the pressing need identified in the field study, with a focus on generating as many ideas as possible, keeping in mind the target consumer's strengths and attributes. Proposals are deliberated for value and viability and small-scale trials or prototypes are created. Frequent feedback from the target population is paramount at this stage to avoid investing too much time and resources to build an intervention that will not work. Prototypes are tested and refined often numerous times until an optimal intervention is created. 3 The desired outcome is a patient-centered health service design that delivers the care needed in a manner that is acceptable and accessible to the patient and provider of care.
The design thinking process can revolutionize the way we deliver palliative care by making it available, acceptable, and valuable to all people facing serious illness. Design thinking ensures that we solve the right service delivery problems and create strength-based solutions. To advance our field, we must endeavor to ensure that all patients with serious illness reap the benefits offered by palliative medicine's philosophy of care by taking advantage of the unique attributes of our patients. It is our responsibility to adapt to the needs of our patients through acknowledging and combating the barriers to care engrained in the way health care is delivered.
Footnotes
Acknowledgment
The authors thank and acknowledge the Boston University Institute of Health System Innovation and Policy for grant support for this project