
Abstract
Background:
Over the past two decades, the number of hospitals with palliative care has increased significantly.
Objective:
This study analyzes the availability of palliative care in U.S. hospitals and examines the variation by hospital characteristics, community-level socioeconomic demographics, health care markets, and geographic characteristics.
Methods:
Data were obtained from the American Hospital Association Annual Survey Database for 2017 and supplemented with 2016 for nonresponders, the United States Census Bureau's 2017 American Community Survey, the Dartmouth Atlas of Health Care's 2016 Spending and 2011 Hospital and Physician Capacity datasets, the National Palliative Care Registry™, state-level directories on palliative care, and web-based searches. Multivariable logistic regression and average marginal effects were used to examine predictors of hospital palliative care programs.
Results:
Seventy-two percent of hospitals with 50 or more beds had palliative care programs. Hospital and geographic characteristics were significantly associated with the presence of palliative care. Most notably, nonprofit hospitals were 24.5 percentage points more likely than for-profit hospitals to have palliative care, and metropolitan areas were 15.4 percentage points more likely than rural areas, controlling for other variables.
Conclusion:
This study demonstrates that availability of palliative care in U.S. hospitals is determined by where patients live and the type of hospital to which they are admitted. Equitable and reliable availability to quality palliative care must improve across the nation.
Background
Millions of people in the United States are living with a serious illness that negatively affects their quality of life and is burdensome in symptoms and caregiver stress. 1 In response to these unmet patient needs, palliative care has proliferated as a team-based specialty focused on improving quality of life and care during serious illness and has evidence of improving quality at lower costs than traditional hospital care. 2
We previously reported that 67% of U.S. hospitals with 50 or more beds had implemented a palliative care program by 2013. 3 Given the continued growth of palliative care and evolving health care market, we have updated and expanded our analysis of palliative care program prevalence and hospital and market correlates as of 2017. Understanding differences in availability of palliative care programs in hospitals across the United States is key to improving the care of those with serious illness and their families.
Methods
We conducted a cross-sectional study using data from the 2017 American Hospital Association (AHA) Annual Survey Database™ (response rate greater than 75% annually) 4 and supplemented with data from the 2016 AHA database for nonresponders. Hospitals self-report the facilities and services available in the hospital, including inpatient palliative care. We linked the AHA database to the United States Census Bureau's 2017 American Community Survey by county and the Dartmouth Atlas of Health Care's 2016 Spending and 2011 Hospital and Physician Capacity datasets by health services area to obtain health care market and geographic characteristics.
We limited our sample to hospitals with 50 or more beds and nonfederal, general medical and surgical, children's, cancer, heart, and obstetrics and gynecology hospitals within the 50 states and the District of Columbia. We corroborated the hospital's palliative care program status in the AHA database by comparing with existing data on hospital palliative care from the National Palliative Care Registry™, state-level directories on palliative care, health system palliative care contacts, and web-based searches. We estimated multivariable logistic regression models and average marginal effects to examine associations between the presence of inpatient palliative care programs and hospital characteristics, community-level socioeconomic demographics, health care markets, and geographic characteristics.
Results
Of the 2409 U.S. hospitals in our sample, 1723 (71.5%) had palliative care programs. Consistent with prior results, the availability of hospital palliative care significantly differed by hospital characteristics and geographic factors in the multivariable model (Table 1). The largest average marginal effects were for hospital ownership, with nonprofit hospitals 24.5 percentage points more likely than for-profit hospitals to have palliative care (95% confidence interval [CI] 18.6–30.3, p < 0.001). The estimated ownership effect differed significantly (p < 0.05) by hospital size (Fig. 1).
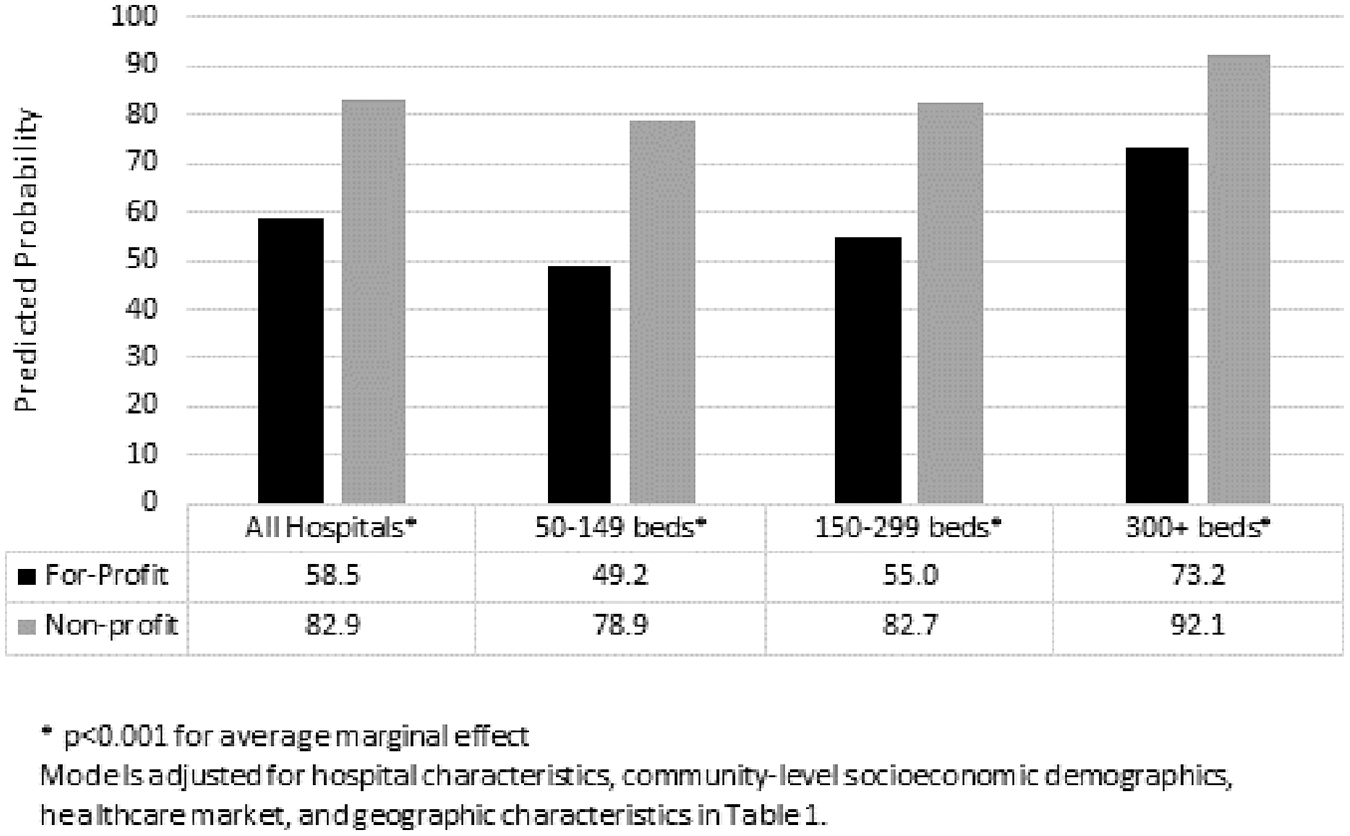
Predicted probability of having a palliative care program by hospital size and ownership. Predicted probability of having a palliative care program by hospital size and ownership. Average marginal effects adjusted for the hospital characteristics, community-level socioeconomic demographics, health care markets, and geographic characteristics included in Table 1. *p < 0.001 for average marginal effect.
Characteristics of U.S. Hospitals (50 or More Beds) with and without Palliative Care Programs, 2017
Other variables included in the multivariable regression equation that were not statistically significant included children's hospital, rural referral hospital, sole community provider hospital, overall Medicare spending in the HSA, physicians per 100,000 Medicare beneficiaries in the HSA, specialist physicians per 100,000 Medicare beneficiaries in the HSA, the percentage of non-Hispanic whites in the county, and the percentage living in poverty in the county.
Statistically significant at p < 0.05.
CI, confidence interval; HSA, health services area.
Notably, availability of hospital palliative care significantly differed between urban and rural areas with metropolitan areas 15.4 percentage points more likely than rural areas to have palliative care (95% CI 0.3–30.4, p < 0.05), adjusting for all measured covariates.
Discussion
We found that although 72% of hospitals with 50 or more beds have palliative care programs, there is marked variability in program prevalence by hospital type. Although these results demonstrate growth in the availability of hospital palliative care since 2013, similar disparities persist. Specifically, only one-third of for-profit hospitals have palliative care programs, and ownership differences in program availability were most apparent for small hospitals. Although for-profit hospitals remained less likely to have palliative care programs than nonprofit or public hospitals, the prevalence of palliative care in for-profit hospitals was 12 percentage points higher than in 2013. Similarly, hospitals in the west south central region remained one of the least prevalent regions for palliative care, but had the largest percentage point growth regionally with an 8 point increase since 2013. Possible explanations for variation in palliative care program availability include inadequate palliative care workforce, insufficient financing and incentives, lack of accountability for access to palliative care, and continued lack of knowledge about palliative care. Our study only assessed the presence of palliative care programs and did not examine the quality, composition, nor size of the service, which is known to vary significantly across palliative care programs. 5 Limitations withstanding, these findings suggest that strategies to close gaps in availability of hospital palliative care are required to meet the needs of millions living with serious illness, and their families.
Footnotes
Acknowledgments
The authors thank the staff of the Center to Advance Palliative Care and National Palliative Care Research Center who contributed to the development of the 2019 State-by-State Report Card on access to palliative care in U.S. hospitals (reportcard.capc.org).
Funding Information
This study was supported by the Gordon and Betty Moore Foundation, the National Institute on Aging (Grant Number AG060270), and the National Palliative Care Research Center.
Author Disclosure Statement
No competing financial interests exist.