
Abstract
Background:
A major goal of hospice care is to provide individually tailored emotional and spiritual support to caregivers of hospice patients.
Objectives:
Examine the association between reported emotional support and caregivers' overall rating of hospice care, overall and by race/ethnicity/language.
Subjects:
We analyzed survey data corresponding to 657,805 decedents/caregivers who received care from 3160 hospice programs during January 2017–December 2018.
Measurements:
Linear regression models examined the association between caregiver-reported receipt of emotional and spiritual support (“too little” vs. “right amount” vs. “too much”) and overall rating of the hospice (0 vs. 100 rating). Interaction terms assessed variation in this association by race/ethnicity/language.
Results:
“Too much” emotional support was less common than “too little,” except for caregivers of Hispanic decedents responding in Spanish. “Too little” support was strongly associated with lower hospice ratings for all groups (compared to “right amount” of support, p < 0.001). In contrast, the negative association between “too much” support and hospice rating was much smaller (p < 0.001) among caregivers of white and black decedents. “Too much” support was associated with more positive ratings among caregivers of Hispanic decedents (p < 0.001).
Conclusions:
Receipt of “too much” support is a less common and much weaker driver of poor hospice ratings than receipt of “too little” support for all groups, and is not always viewed negatively. This suggests that for hospice evaluation, “too much” support should not be scored equivalently to “too little” support and that providing enough support should be a hospice priority.
Introduction
Over 1.4
Some family caregivers have reported not needing or wanting any emotional or spiritual support from the hospice, or receiving more outreach than desired (for example, repeated mention or suggestions of chaplaincy support after it had been previously declined); therefore it is important to distinguish too much support (i.e., more than desired) from desired levels of emotional and spiritual support. Recent estimates show that nearly 20% of Americans are neither spiritual nor religious, highlighting the potential undesirability of offered spiritual support for such caregivers. 6 Thus, given that caregivers will vary in terms of the degree to which they want hospice staff to provide spiritual and emotional support, individualized support is essential.
Previous work examining the receipt of emotional and spiritual support in hospice has demonstrated that receiving the right amount of emotional and spiritual support is significantly associated with caregivers' overall hospice experiences and their ultimate willingness to recommend a hospice to friends and family.7–12 However, little is known about the extent to which receiving too little support vs. too much support affects perceptions of overall hospice quality. Understanding the association between the amount of support received and overall hospice rating could inform hospices' quality improvement efforts in an area central to the hospice mission.
In addition, while caregivers often report receiving the right amount of support, there is room for improvement.12–16 Prior work has shown that caregivers of Hispanic and black decedents report receiving the right amount of emotional and spiritual support less often than caregivers of white decedents. 17 It is unclear whether these differences may, in part, reflect differences in cultural norms, expectations, or preferences. Insight into the complex relationship between the level of emotional and spiritual support that is desired by caregivers, and how this may vary by race/ethnicity, may help shed light on the reasons behind these observed differences, and inform hospice efforts to appropriately tailor provided emotional support to caregivers.
In this article, we examine the association between caregivers' overall rating of the hospice and the amount of emotional and spiritual support reported by caregivers using data from the Consumer Assessment of Health care Providers and Systems (CAHPS®) Hospice Survey.9,18,19 We additionally examine how this association varies by race/ethnicity. Importantly, these results prompted the Centers for Medicare & Medicaid Services (CMS) to make a nationally implemented scoring change for the publicly reported Emotional and Spiritual Support composite quality measure.20,21
Methods
Study sample
The CAHPS Hospice Survey was designed to be completed by the primary caregiver of the hospice decedent. Caregivers were eligible for inclusion if the decedent was 18 years or older at death and died at least 48 hours after their last admission to hospice care; additional eligibility details are described elsewhere. 17 Since April 2015, all Medicare-certified hospices are required to participate in the CAHPS Hospice Survey unless they are new or served fewer than 50 survey-eligible decedents/caregivers in the prior calendar year. Surveys were administered using mail-only mode, telephone-only mode, or mixed mode. Details of the mode protocols are specified elsewhere. 22
We analyzed CAHPS Hospice Survey data regarding decedents who died while in hospice care from January 2017 to December 2018; the survey response rate for this period was 32%. Caregivers who completed the survey in a language other than English or Spanish and caregivers with missing values for survey language (n = 296) were excluded. For analytic stability, hospices with fewer than 20 completed surveys over the two-year period (n = 477 hospices) were excluded. Therefore, we report on care experiences of 657,805 hospice decedents from 3160 hospice programs. This study was approved by the Institutional Review Board at the RAND Corporation.
Survey instrument, measures, and scoring
The CAHPS Hospice Survey instrument
22
consists of 47 items and is used to calculate eight hospice quality measures. One of these measures is Getting Emotional and Religious Support, which is composed of the following three items:
While your family member was in hospice care, how much emotional support did you get from the hospice team? In the weeks after your family member died, how much emotional support did you get from the hospice team? Support for religious or spiritual beliefs includes talking, praying, quiet time, or other ways of meeting your religious or spiritual needs. While your family member was in hospice care, how much support for your religious and spiritual beliefs did you get from the hospice team?
Response options for all three items are “Too little,” “Right amount,” and “Too much.” We examine each response category individually.
The second quality measure used in our analyses is Overall Hospice Rating, which is obtained using the item “Using any number from 0 to 10, where 0 is the worst hospice care possible and 10 is the best hospice care possible, what number would you use to rate your family member's hospice care?” For public reporting of CAHPS Hospice Survey measure scores, responses are scored such that 9 and 10 are coded as 100 and all other responses are coded as 0; we use this coding in our analyses.
Caregiver and decedent characteristics
The primary characteristics used in our analyses were race/ethnicity and survey language. Race/ethnicity of the decedent, reported by the caregiver, was categorized as Hispanic, non-Hispanic black (hereafter “black”), non-Hispanic white (hereafter “white”), and other. All decedents other than Hispanic, black, and white decedents were categorized into the “other” category because of small sample sizes, and we do not present analytic results for this heterogeneous group. Survey language was either English or Spanish. We combined these two variables to create a variable with the following categories: white; Hispanic/English survey; Hispanic/Spanish survey; black; and other.
In keeping with protocols for calculation of publicly reported measure scores, characteristics known to be associated with how respondents answer CAHPS Hospice Survey questions were used for adjustment: decedent's age, primary diagnosis, and length of final episode of hospice care; payer for hospice care; respondent's age, education, and relationship to decedent; and response percentile (reflecting the length of time between decedent death and survey response). 23 While publicly reported measure scores are also adjusted for survey language, we do not adjust for language here as it is part of our primary variable of interest.
Statistical analysis
To examine the frequency with which each response option was used, we descriptively examined the unadjusted distribution of responses for each item within the Emotional and Religious Support measure, overall and by race/ethnicity/language. Second, to examine the association between the amount of support received and the overall hospice rating, we fit a mixed-effects linear regression predicting the overall hospice rating (0 vs. 100 rating) from the response to each support item (with “Right amount” as the reference), adjusting for the caregiver and decedent characteristics listed above, and the combined race/ethnicity/language variable (with white as reference), with random effects for hospices.
As stated above, while we do not present analytic results for the “other” race/ethnicity/language group, this group was included in all models to ensure their contribution to the main effect estimates for the support item response options. Finally, we added to this regression model an interaction between the support item response categories and the race/ethnicity/language variable. The purpose of this interaction term was to examine whether the association between the reported amount of support and overall rating differed across the race/ethnicity/language groups. To assist with interpretation and characterize the nature of any interaction effects, significant interaction terms were summarized at the level of the race/ethnicity/language groups.
In all regression models, the overall rating item was adjusted for mode of administration. 24 In addition, weights were used to account for sampling and nonresponse. Missing decedent and caregiver characteristics were imputed with hospice-level means. Missing responses to the support items and overall rating item (1.4–4.8%) were not imputed. P-values <0.05 were considered statistically significant.
Results
Characteristics for our analytic sample (n = 657,805) are shown in Table 1. Over half of the decedents were female; the majority were 65 years of age and older and had Medicare only as their payer for hospice care; 86% were white, 5% were Hispanic, and 5% were black. The most common primary diagnosis was cancer; most caregiver respondents were the hospice decedents' children.
Characteristics of Decedents and Caregiver Respondents (n = 657,805)
Percentages are weighted to account for sampling and nonresponse; missingness of decedent and caregiver characteristics were handled by imputing with the hospice-level mean.
Note that analyses throughout are restricted to those who responded in English or Spanish.
Chronic end-organ diseases include the following: congestive heart failure, other heart disease, chronic kidney disease, chronic liver disease, and noninfectious respiratory disease.
For all three emotional support items, the overall most common response was “right amount,” followed by “too little”; “too much” was the least common response option (Fig. 1). This pattern held for each race/ethnic/language group, except that caregivers of Hispanic decedents who responded in Spanish were more likely to select “too much” than “too little.” For all items, caregivers of Hispanic decedents using a Spanish survey were more likely to select “too much” (range of 17.8–22.6% across the three items) than all other groups; caregivers of white decedents were the least likely to select “too much” (range of 0.3–0.9% across the three items).
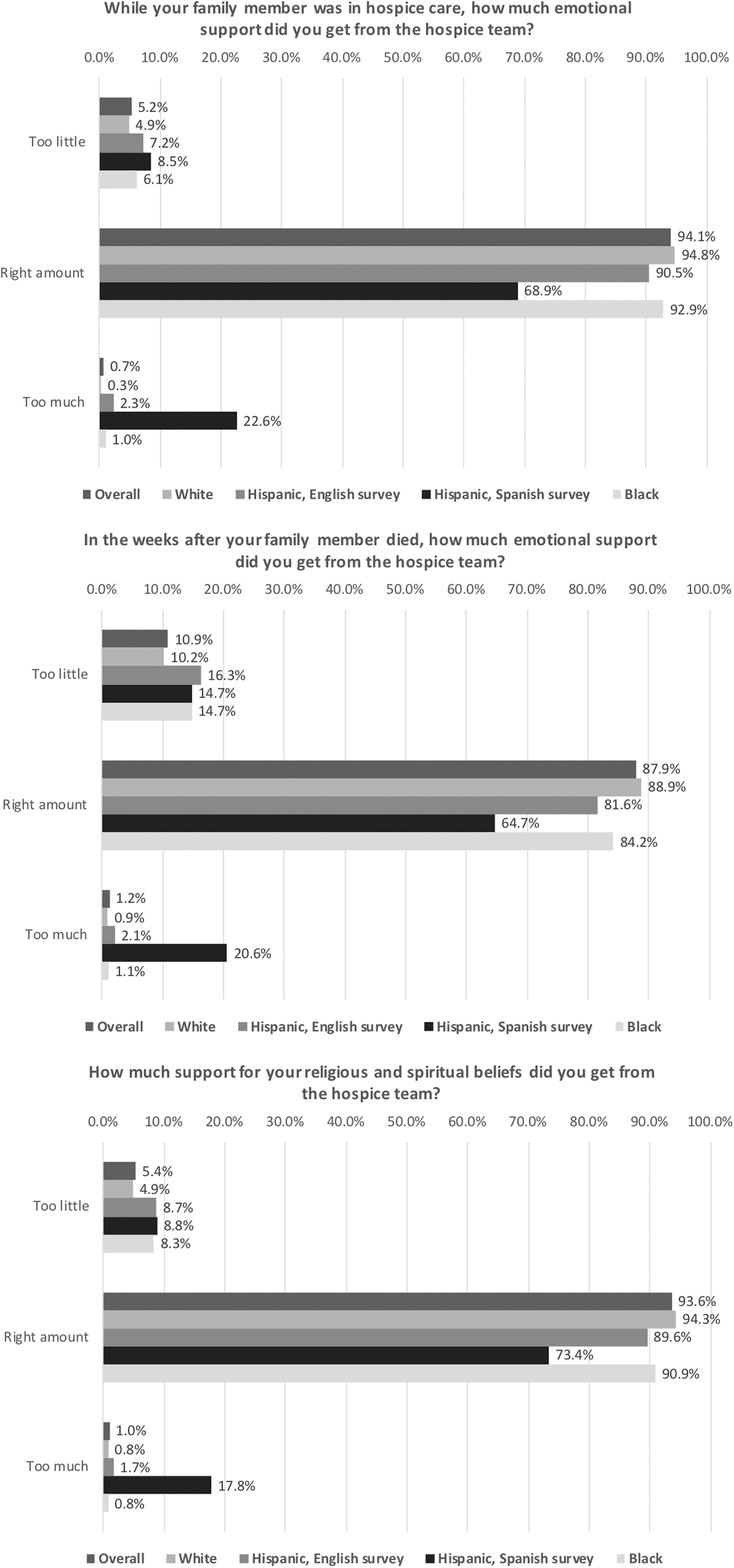
Unadjusted response distributions for the three items that compose the getting emotional and spiritual support measure. Percentages are weighted to account for sampling and nonresponse.
Regression results from the model with only main effects are shown in Table 2. Caregivers who reported “too little” support tended to rate the hospice lower than those who reported the “right amount” of support (68 points lower on a 0–100 scale, p < 0.001, for receipt of emotional support while receiving hospice care; 38 points lower, p < 0.001, for receipt of emotional support after death; and 47 points lower, p < 0.001, for support for religious and spiritual beliefs while receiving hospice care).
Regression Results Examining the Association between Emotional and Spiritual Support Items and Overall Hospice Rating, without Interaction a
p < 0.001.
Regression results from mixed-effects linear regression models predicting the overall hospice rating (where 0–10 responses were scored such that 9 and 10 were coded as 100 and all other responses were coded as 0) from the response to the support item (with “Right amount” as the reference), adjusting for the combined race/ethnicity/language variable (with white as reference), with random effects for hospices and adjusting for decedent's age, primary diagnosis, and length of final episode of hospice care; payer for hospice care; respondent's age, education, and relationship to decedent; and response percentile; responses to the overall rating item were appropriately adjusted for mode of administration and weights were used in the regression model to account for sampling and nonresponse; missingness of decedent and caregiver characteristics was handled by imputing with the hospice-level mean; missing responses to the support items and overall rating item were dropped from the relevant regression model; “other” race/ethnicity/language group was included in the regression (so that this group contributes to the main effect estimates for the response options), but associated coefficients are not shown here.
SE, standard error.
In contrast, while respondents who reported “too much” support also tended to rate the hospice lower than those who reported the “right amount” of support, the magnitude was much smaller (8 points lower on a 0–100 scale, p < 0.001, for receipt of emotional support while receiving hospice care; 17 points lower, p < 0.001, for receipt of emotional support after death; and 18 points lower, p < 0.001, for support for religious and spiritual beliefs while receiving hospice care).
Joint tests of adding interactions between response options and race/ethnicity/language to each model were significant (p < 0.001), indicating evidence of significance variation in the association between the response options and overall rating by race/ethnicity/language. Regression results from the model with interaction effects are shown in Table 3. Examining the summary effect of the “too little” response option within each group, although there was variation in magnitude, the direction of the effect was the same for all groups, always indicating very negative associations between “too little” support and overall rating of the hospice.
Regression Results Examining the Association between Emotional and Spiritual Support Items and Overall Hospice Rating, with Interaction a
0.01 ≤ p < 0.05, **0.001 ≤ p < 0.01, ***p < 0.001, #p = 0.003, ##p = 0.002, ###p = 0.035.
Regression results from mixed-effects linear regression models predicting the overall hospice rating (where 0–10 responses were scored such that 9 and 10 were coded as 100 and all other responses were coded as 0) from the response to the support item (with “Right amount” as the reference), adjusting for the combined race/ethnicity/language variable (with white as reference), with an interaction between the support response option and the combined race/ethnicity/language variable, with random effects for hospices and adjusting for decedent's age, primary diagnosis, and length of final episode of hospice care; payer for hospice care; respondent's age, education, and relationship to decedent; and response percentile; responses to the overall rating item were appropriately adjusted for mode of administration and weights were used in the regression model to account for sampling and nonresponse; missingness of decedent and caregiver characteristics were handled by imputing with the hospice-level mean; missing responses to the support items and overall rating item were dropped from the relevant regression model; “other” race/ethnicity/language group was included in the regression (so that this group contributes to the main effect estimates for the response options), but associated coefficients are not shown here.
In contrast, examining the summary effect of the “too much” response option within group, “too much” support was positively associated with overall rating of the hospice for some groups and negatively for others. Specifically, while the effect of “too much” support on overall rating was negative for caregivers of white decedents for all support items (23–25 points lower compared to “right amount”), the effect was significantly positive among caregivers of Hispanic decedents using the Spanish survey for all support items (7–8 points higher compared to “right amount”) and among caregivers of Hispanic decedents using the English survey for the item regarding receipt of emotional support, while the family member was receiving hospice care (5 points higher compared to “right amount”).
Effects among caregivers of black decedents were similar to those for white decedents for two of the three support items, with “too much” having a negative, but smaller effect on overall rating (10–12 points lower).
Discussion
Similar to prior studies examining the association between emotional support and overall hospice rating, we found that receiving the right amount of support is strongly associated with a caregiver's hospice rating, and specifically, that receiving too little support is associated with a much more poorer rating of the hospice.7–12 A unique contribution of this work is evidence that receiving too much support is not as strongly associated with a poor hospice rating as too little support and that “too much” support may be viewed positively by caregivers of Hispanic decedents.
A hospice's score on the Getting Emotional and Religious Support measure, composed of the items analyzed in this study, is publicly reported as part of CMS' Hospice Quality Reporting Program.20,21,25 The findings presented in this study resulted in a change in CMS' scoring of these items starting in August 2019, whereby responses indicating “too much” support are now not included in the publicly reported score. This scoring change directly reflects findings from this analysis—that too much support is not viewed as negatively as too little support and for some caregivers, is viewed positively. Our findings also indicate that hospices should not curtail emotional support out of concern for providing too much support, given that providing too little support is the most common departure from what caregivers desire and the one that may be most harmful to their overall hospice experience.
Importantly, while those indicating too much support are no longer included in the publicly reported score, keeping the described response option categories is necessary and provides valuable information for hospice quality improvement efforts. During development of the CAHPS Hospice Survey in 2012–2014, 19 cognitive testing of these items found that asking about receipt of emotional and spiritual support with a Yes/No or Yes, definitely/Yes, somewhat/No response scale did not adequately capture experiences where the caregiver felt they received too much support. Retaining the Too little/Right amount/Too much response option scale allows a hospice to examine the proportion of caregivers who report receiving too much support in their hospice program and if needed, tailor hospice services and training of hospice staff accordingly.
Our finding that receiving too much support appears to be viewed as a positive experience for caregivers of Hispanic decedents provides valuable insight into differences in end-of-life preferences and is an important contribution to the literature on this topic. Previous qualitative studies focused on differences in end-of-life beliefs and preferences have repeatedly demonstrated racial/ethnic differences with respect to these factors.26–31 This previous work has shed light on the implications of Hispanic/Latino cultural norms (shared expectations and rules that guide behavior of people within social groups) and scripts (commonly held assumptions about how people think about social interactions) on end-of-life care in this community.
For example, familismo (a strong orientation toward the family), simpatia (a pattern of social interaction emphasizing courtesy in interpersonal relationships), machismo (in this context, men feeling the need to serve as protectors and providers for the family), and respecto (respect) are fundamental cultural scripts for many Hispanic/Latino families, and hospices must ensure that end-of-life care aligns with these scripts.30,32–34 In light of these cultural differences, it is possible that a level of emotional and religious support provided by hospice staff that would be regarded as a “right amount” to caregivers of non-Hispanic decedents may be regarded as intrusive and inappropriate among caregivers of Hispanic decedents, thus resulting in their indication that they received too much support and potentially explaining our observation that caregivers of Hispanic decedents, particularly those using a Spanish survey, were much more inclined to indicate they received too much support for all support items.
However, while described as “too much” support by these caregivers, it does not translate into an overall poor experience with the hospice and in fact, our results show, may correspond to a better rating of the hospice. It is possible that these support efforts are viewed by caregivers of Hispanic decedents as indications of the hospice staff's good will. These results highlight complex differences in various aspects of end-of-life preferences among different caregivers and the need for hospice staff, and hospice care generally, to attend to cultural norms and preferences and to tailor supportive needs as much as possible.10,30,33–37
Although the tendency to both report too much support and associate too much support with a better overall rating was observed among caregivers of Hispanic decedents using either a Spanish or English survey, these findings were more pronounced among those using a Spanish survey. Importantly, the translation of “too much” support in the Spanish version of the survey was “demasiado,” a common translation of this phrase. During cognitive testing with Spanish speakers, conducted as part of the survey development, “demasiado” tested well among participants, except for one participant who interpreted “demasiado” as conveying “plentiful,” with a more positive connotation than “too much” generally does in English.
Thus, further cognitive testing may shed light on potential subtleties in the interpretation of this phrase and potential variation in interpretation by region or origin. Nonetheless, these findings regarding “too much” support are observed regardless of survey language among Hispanics and thus imply that these effects, at least in part, must be attributable to cultural differences rather than language alone.
Our study has some limitations. First, our analyses were restricted to survey respondents in hospices large enough to be required to participate in the CAHPS Hospice Survey and with at least 20 respondents over two years of survey administration. Therefore, our results may not be representative of decedents and caregivers receiving care among all hospices nationally, particularly small hospices. Regarding the restriction of our analysis to survey respondents only, however, previous work suggests that adjusting for differences in case-mix, as is done here, adequately addresses any nonresponse bias.38,39
Second, caregiver race/ethnicity was unavailable, and thus our interpretation of results regarding cultural norms relies on the assumption that the race/ethnicity of the decedent is a reasonable proxy for that of the caregiver. While we are unable to confirm this assumption, the majority of the caregivers are family members of the decedents (Table 1). Finally, given small sample sizes, we were unable to examine more refined subgroups such as caregivers of Hispanic black decedents or multiracial decedents; future work examining receipt of emotional support within these groups is warranted.
Conclusion
Receipt of “too much” support is a less common and much weaker driver of poor hospice ratings than receipt of “too little” support for all groups, and is not always viewed negatively. These results suggest that for hospice evaluation, “too much” support should not be scored equivalently to “too little” support and that providing enough support should be a hospice priority.
Footnotes
Funding Information
The data collection and analysis on which this publication is based were sponsored under contract numbers HHSM-500-2016-00022G and 75FCMC19F0026, entitled, “National Implementation of the CAHPS Hospice Survey,” funded by the Centers for Medicare and Medicaid Services, Department of Health and Human Services. The content of this publication neither necessarily reflects the views or policies of the Department of Health and Human Services nor does the mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
Author Disclosure Statement
No competing financial interests exist.