
Abstract
Background:
Primary care clinicians care for most persons with Alzheimer's disease and related dementias (ADRDs), yet lack dementia-specific skills in advance care planning (ACP).
Objectives:
To develop and evaluate a training toolkit for primary care clinicians to improve ACP communication for people with ADRD and their families.
Design:
Clinical practice outcomes assessment and pre–post-training evaluation. Intervention training toolkit addressed ACP skills by dementia stage: (1) advance directives in early dementia, (2) decision-making capacity in moderate dementia, (3) Physician Orders for Life-Sustaining Treatment (POLST) in late-stage dementia, and (4) hospice and hospitalization in advanced dementia.
Setting/Subjects:
Nonhospitalized clinical care sites, 51 clinicians in North Carolina, USA.
Measurements:
Data collection utilized structured chart abstractions and pre- and post-training surveys.
Results:
Of 51 participants trained, 33 had encounters with patients with ADRD in study period. Most participants were women (n = 42), white (n = 37), and physicians (n = 31). Participants increased documentation of surrogates (22.7% vs. 35.5%, p = 0.03), decision-making capacity (13.5% vs.23.2%, p = 0.04), and POLST completion (9.2% vs. 18.8%, p = 0.03). Training increased ACP documentation (6.4% vs. 14.5%, p = 0.031) and goals of care (GOC) decision-making discussions (17.0% vs. 31.9%, p = 0.005). In pre–post-comparisons, participant confidence increased in determining capacity, exploring dementia prognosis, GOC, eliciting surrogates, and leading family meetings (all p < 0.001). Most participants strongly agreed that the training addressed skills used in practice (n = 34), contained clear language (n = 40), took an appropriate amount of time (n = 32), and was designed effectively (n = 35).
Conclusion:
This video-based training resource increased the use of dementia-specific ACP communication skills and clinician confidence.
Introduction
Alzheimer's disease and related dementias (ADRDs) are incurable, progressive diseases with enormous impact on health care systems, and on people with ADRD and their families. Globally, prevalence of ADRD may increase from 47 to 75 million people by 2030. 1 Practice guidelines encourage advance care planning (ACP) communication to allow people with ADRD and their families to match care to goals and preferences. 2 People with ADRD and families must weigh treatment options based on numerous factors—information about diagnosis, prognosis and illness trajectory, symptom distress, prior experiences, financial considerations, and trade-offs between outcomes such as comfort, function, and life prolongation.3–5 Dementia complicates this challenging process enormously. 6
People with ADRD gradually lose decision-making capacity years in advance of the need for important medical decisions. Clinicians and families must discern when people with ADRD have capacity to express treatment preferences, and how to uphold people's values when decisional capacity is lost. 7 As dementia progresses, families become surrogate decision makers—often with limited knowledge of the older person's own preferences.8,9 Furthermore, several of the key decisions faced by families may seem like “usual care,”—nutritional support, treatment of infection, and repeated hospitalization—creating emotional and moral distress for surrogates.10,11
In the United States, most health care for people with ADRD is provided by primary care clinicians. Primary care clinicians lack high-quality training to support ACP in ADRD care. 12 They struggle with the challenges of ACP for people with ADRD, citing knowledge deficits, time constraints, documentation issues, and changing preferences.13,14 Evidence-based training in ACP communication skills exists, but does not address the unique issues for patients with ADRD.15,16 To fill this gap, we developed and evaluated a video-based toolkit to train primary care clinicians in dementia-specific ACP.
Materials and Methods
Training development
We recruited an advisory board comprising key stakeholders to ensure relevance to ADRD caregivers and primary care clinicians and consistency with ADRD best practices. With input from stakeholders, the research team developed four video-based modules and training content addressing ACP skills across stages of dementia. Stakeholders advised on the design of the intervention, provided feedback on the video-based scenarios, and the outcome measures of the study. This research was reviewed by the Institutional Review Board at the University of North Carolina at Chapel Hill (IRB# 17-2649) and deemed not human subjects research.
Training content and methods
Training content was structured into four modules to address different ACP elements by Global Deterioration Scale (GDS) stage.
17
Training methods were appropriate to adult learners, and included brief didactics, videotaped scenarios to illustrate ACP communication skills, and role-plays for practicing skills. Stage-specific resources such as copies of the Physician Orders for Life-Sustaining Treatment (POLST) form and weblinks to advance directives were included as indicated at the end of each module. The four modules addressed:
ACP in early dementia (GDS 2-3): This module focused on promoting goal-concordant care in the future as patients experience cognitive decline, including determining a preferred surrogate health care decision maker and considering completion of advance directives such as living wills. Decision-making capacity in moderate dementia (GDS 3-4): This module focused on how to assess decision-making capacity in a clinic setting and communicate with sensitivity and respect for the ACP needs of both the person with dementia and their family. Using the POLST in late-stage dementia (GDS 4-6): This module provided techniques to communicate around the issues of resuscitation, level of treatment, infection treatment, and nutrition decisions with families of people with late-stage dementia. Hospice and hospitalization in end-stage dementia (GDS 7): This module include communication techniques for discussing the choice of hospice and how that relates to ongoing hospitalization.
Each module included a 15-minute didactic portion comprising key dementia and communication evidence, a 5- to 10-minute video modeling ACP communication skills for that dementia stage, and a 15-minute role-playing session with clinical vignettes related to that specific stage of dementia. The videos included actors representing primary care clinicians, people with ADRD, and their families. Role-playing sessions allowed participants to practice dementia-specific ACP techniques they had just witnessed in the video to promote content uptake. 18 We paired participants, presented a patient scenario related to each stage of dementia, and asked one of each pair to practice as the “clinician” and one to role-play the “patient” (or family member). We also included clinical resources, such as a copy of the POLST form.
At the end of the training, we encouraged participants to fill out an action plan describing what they learned and how they were going to put that knowledge into practice. Each module took ∼45 minutes to complete; the entire training took four hours. Sessions including all four modules were held at private locations with space to accommodate 10–12 participants. Training sessions were delivered at different times, such as Saturday mornings or weekday evenings, to facilitate participation. Sessions were conducted by a physician with expertise in geriatrics and palliative medicine (C.E.K and L.C.H.) and one other investigator and a research staff member.
Participants and recruitment
We recruited primary care clinicians from a multicounty region in central North Carolina, with >50 primary care clinics representing an extensive geography and diverse communities. We recruited clinicians by contacting leaders within clinical sites and asking them to spread marketing materials inviting their colleagues to the training. Given that diverse disciplines may participate in ACP, we opened the training to physicians, physicians-in-training, advance practice providers, social workers, and nurses. Participants were not reimbursed for their time but received continuing education credits and a meal.
Measures
Data collection utilized pre- and post-training surveys to evaluate the effect of training on confidence in skills, and structured review of chart documentation of clinical encounters to evaluate effect on practice. Participants provided demographic and training data during the pretraining survey. Training evaluation items were modified from ACP communication training for critical care. 19 Survey items addressed participants' confidence in dementia-specific ACP skills (rated on a 4-point Likert-type scale, from “not very confident” to “very confident”), including determining capacity, exploring dementia prognosis, exploring GOC, eliciting surrogates, recommending self-care practices to families, leading family meetings about GOC, and leading family meetings about hospice.
Post-training, participants were asked four questions on perceived usefulness of training. Items were derived from usability testing principles and rated on a 5-point Likert-type scale, from “strongly disagree” to “strongly agree.” 20 Participants were asked to agree or disagree with whether the training addressed skills used in their practice, contained clear language, took an appropriate amount of time, and was designed effectively.
Participants had the opportunity to provide comments to each of these five usability Likert-type statements. We included two additional open-ended questions, “Of all that I learned during the training session, the most useful skill for my practice is”: and “Trainings sessions would be more effective to improve ACP for persons with dementia if”: At the conclusion of the training, participants who routinely saw patients with ADRD were asked if they would like a list of their patients to help identify those in need of dementia-specific ACP.
A trained research staff member conducted structured chart reviews of patient encounters in the six-month window before and the six-month window after training. Each physician/advance practice provider (APP) participants' patient panel was screened to identify eligible patients using a computable ADRD phenotype modified to capture the spectrum of dementia during these windows. 21 Participants were ineligible for this portion of evaluation if they had no patients with ADRD during the study period, or if they were physicians-in-training. Investigators selected a random sample of up to five charts of patients with ADRD pre- and post-training to review for ACP practices. To ensure randomness, we developed a prespecified set of integers {a, a + 1, …, b} to denote days between selected patients. We then took the random list of integers to add sequentially to the seed number over the time period, thus selecting patients at random intervals throughout the six-month windows.
Structured chart abstractions captured data on ACP practices. Measures of ACP practice included (1) documentation of a chosen surrogate decision maker, (2) documented discussion of written advance directives including living will or health care power of attorney (HCPOA), (3) report of decision-making capacity for the patient with ADRD, (4) completion of a POLST form, (5) documented discussion of prognosis or future medical complications of dementia, and (6) presence of a goals of care (GOC) discussion about at least one major treatment. When a GOC discussion was present we coded for five common items: CPR/mechanical ventilation, hospitalization, treatments for infections, artificial feeding/hydration, and hospice. Finally, we assessed for emergency department visits and hospitalizations. Additional measures included demographic and dementia-related patient characteristics.
Analysis
Differences between pre- and post-training documented ACP practices were compared using either Fisher's exact tests (categorical) or Wilcoxon rank-sum exact tests (continuous; two-sided). Confidence responses were dichotomized as “not very confident” or “somewhat confident” (0) versus “confident” or “very confident” (1). Usability statements were presented as frequencies. Differences between clinicians' confidence pre- and post-training were compared by using Wilcoxon signed-rank tests in Stata 16.1 (Stator).
To identify ways to improve the training, we conducted a thematic qualitative analysis of open-ended comments in the post-training surveys. 22 C.E.K. and A.S.B. read and analyzed the phrases, sentences, or longer segments of text to generate codes. 23 Our team met to review the codes and achieve consensus on discrepancies. We then grouped codes into larger categories to reflect major themes.
Results
We conducted six training sessions from October 2018 to August 2019. We trained 51 participants with 6–13 participants per session; 33 had primary care panels of patients with ADRD and were included in the evaluation of ACP practices. Most participants were women (n = 42, 88%), white (n = 37, 77%), and physicians (n = 31, 61%) (Table 1). Settings were diverse, with 22 (49%) working in urban, and 13 (28%) in rural settings.
Provider Characteristics
Data collected through provider self-report at time of training (October 2018 to August 2019). Owing to missing data, observation counts range from 43 to 51 for all providers.
SD, standard deviation.
ACP practices
The 33 medical providers had 141 pretraining and 138 post-training ADRD patient encounters. Most patients with ADRD were female, white, and in their early 80s (Table 2). Compared with pretraining, clinicians post-training encounters demonstrated increased documentation of surrogate decision makers (22.7% vs. 35.5%, p = 0.03), assessment of capacity (13.5% vs. 23.2%, p = 0.04), and POLST form completion (9.2% vs. 18.8%, p = 0.03) (Table 3). No difference was found in the rates of living will/HCPOA discussions (29% vs. 30%) or discussion of medical complications of dementia (24% vs. 28%). Clinicians increased use of dedicated ACP notes (pretraining 9 [6.4%] vs. post-training 20 [14.5%], p = 0.031). Documented GOC decision making also increased, such that discussions of any of five major treatment decisions rose from 24 (17.0%) to 44 (31.9%), p = 0.005. We found no significant differences in emergency department visits.
Patient Characteristics, by Time
Patients represent those seen by 33 unique providers. Data collected through chart review by two trained abstractors (May 2019 to March 2020). Owing to missing data, characteristic observation counts range from 273 to 279.
Patient Outcomes for Dementia-Specific Training Skills, by Time
Owing to missing data, outcome observation counts range from 278 to 279 for all patients. Patients represent those seen by 33 unique providers. p-Values compared pre- and post-training patient frequencies using Fisher's exact test (categorical) or Wilcoxon rank-sum exact test (continuous); two-sided.
Aggregate measure based on five individual items.
ACP, advance care planning; GOC, goals of care; HCPOA, health care power of attorney; POLST, Physician Orders for Life-Sustaining Treatment.
Confidence and training usability
Participants increased confidence in all categories of communication skills (p < 0.001) (Table 4). They reported increased confidence for determining decisional capacity, exploring dementia prognosis, exploring GOC, eliciting surrogate decision makers, recommending self-care, and leading family meetings on GOC and on hospice/hospitalization decisions. Although 25–41% of participants reported being confident or very confident in these topics pretraining, rates post-training ranged from 75% to 98%. Most participants agreed or strongly agreed that the training addressed knowledge and skills useful to clinical practice, had clear language, took an appropriate amount of time, and was an effective educational method (Fig. 1).
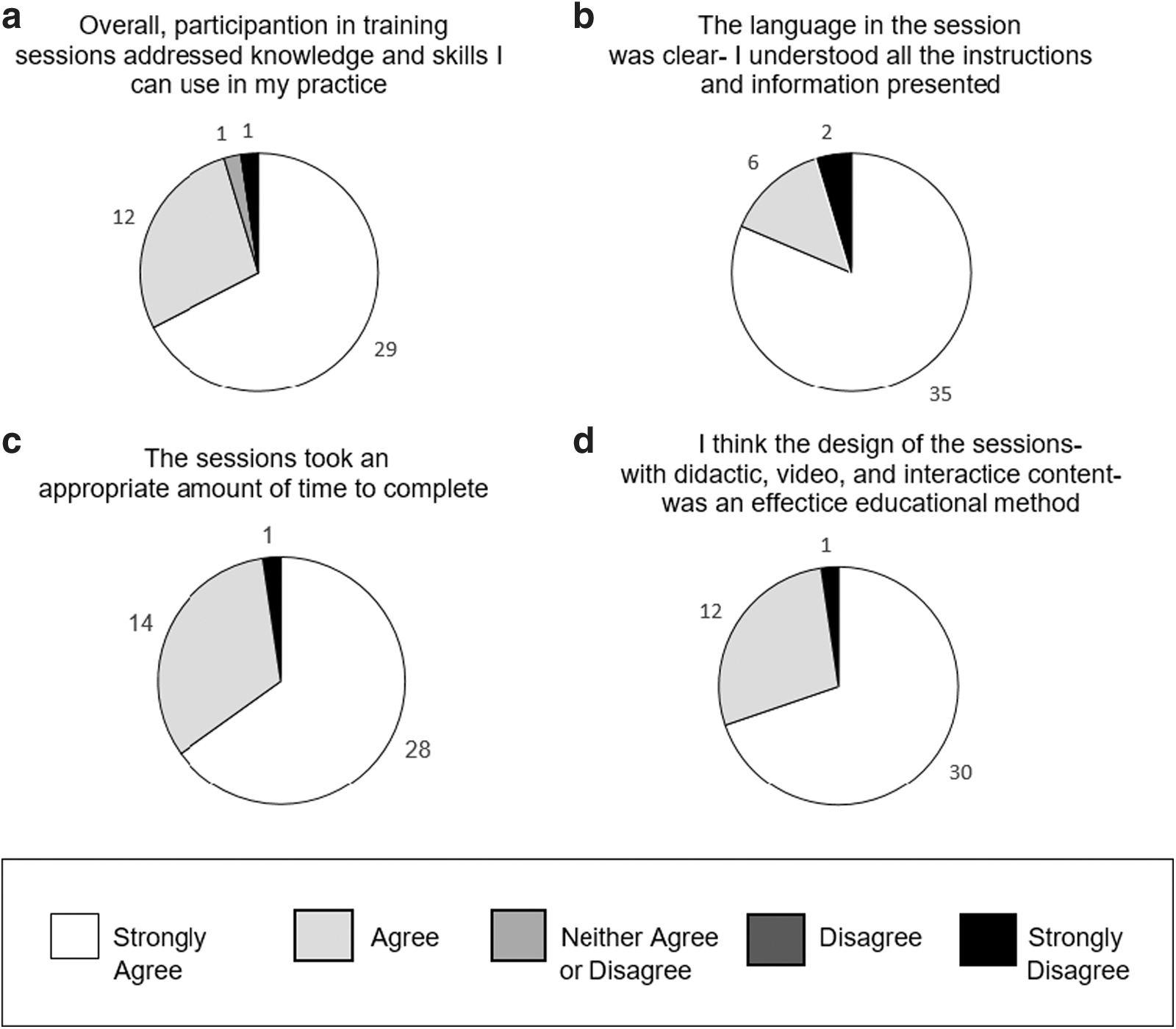
Primary care clinicians' perceived usability of training, N = 43.
Medical Provider Pre–Post-Training Confidence, N (%)
p-Value tests for paired difference in frequency for pretraining responses versus post-training responses using Wilcoxon signed-rank test. p < 0.001 for all comparisons; collected by provider self-report from October 2018 to January 2019. Owing to missing surveys, observation counts range from 44 to 45 participants.
Qualitative feedback on training
In response to our open-ended questions, comments were generally positive, including statements such as “Excellent overall should be mandatory for all PCPs,” particularly about the resource materials and the videos. Participants found different portions of the training session most useful. Participants stated that the dementia-related content (e.g., prognosis and stages of ADRD) and the communication aspects of the training (e.g., how to frame discussion and offer recommendations) were most useful. When asked about improvements, participants wanted more experience with the pragmatic work of doing an ACP note or filling out a POLST form. Participants noted the training should focus more on the role of social workers. Participants requested more interactive time, especially with actual older adults coping with ADRD or their family members. Finally, participants requested specific guidance around cultural/religious preferences.
Discussion
We developed the first interactive video-based training toolkit to enhance dementia-specific ACP skills for primary care clinicians caring for people across the spectrum of ADRD. Our initial evaluation impacted their actual ACP practices and demonstrated significant improvement in their confidence in their skills. The video-based training resource was effective in increasing primary care clinicians' confidence in and performance of dementia-specific ACP communication skills. Most participants positively evaluated the training as useful, clear, timely, and effective.
Our study draws on ACP communication efforts such as VitalTalk for other settings and populations; however, these resources do not address the unique ACP needs in ADRD.19,24 Across the trajectory of this condition, people with ADRD experience an early phase of illness in which they can (but often do not) participate in ACP, followed by an extended period of illness in which surrogate decision makers become increasingly involved. The approach to this transition, and the communication skills for inclusion of both patient and caregiver represent unique elements of ACP. Primary care practice is an ideal setting to address ACP for people with ADRD by providing multiple visits to deliberate on their GOC. Our chart review findings are consistent with outcomes that define successful ACP, focusing on surrogate designation and documentation, including discussions with surrogates, and documenting wishes and goal-concordant care plans such as the POLST. 25
Unfortunately, although significantly improved, the rates of documented dementia-specific ACP communication skills remained low. Only about a third of patients with ADRD had a documented surrogate decision maker post-training. These low rates are similar to the recent Dutch study that had less than a 50% implementation rate for any elements of ACP. 26 Both of these findings may be due to the short duration of follow-up after training but may indicate other barriers to ACP communication and documentation. In support for this supposition, our participants noted their appreciation of pragmatic support on how to complete ACP documentation in clinical practice.
Future efforts to improve ACP completion could focus on methods to increase the opportunity for primary care clinicians to use their skills, such as scheduled ACP planning visits led by clinic-based champions with ongoing audit and feedback. Although a recent editorial in this journal argued that ACP may be wasted breathe, 27 we believe the incremental progress made given the low intensity of this intervention bodes well for future efforts. In addition, our training did not improve several dementia-related outcomes. Despite the increased surrogate documentation, we saw no change in living wills or HCPOA discussions, nor were changes seen in the discussions of dementia complications or frequency of cognitive/functional assessments. Revisions to the training session will need to focus on these areas to provide more global dementia-related support.
Our findings add to the evidence that structured ACP training specified for dementia improves clinician confidence and perceived dementia ACP communication skills. 28 The training shares key features found in effective training for advanced clinical learners: it used problem-based learning, active participation, did not involve reading written materials, included time for discussion and debriefing, and was delivered by an experienced trainer.29,30 Unlike previously published training interventions that primarily focused on trainees, our intervention targeted practicing primary care clinicians and demonstrated measurable practice change.24,31–33 Although other ACP interventions in primary care, such as ACP interactive websites or group visits, are effective, these interventions are not specifically tailored to those with ADRD.34–36
Our intervention contains similar content to the Center to Advance Palliative Care's “Best Practices in Dementia Care and Caregiver Support” training that is longer in duration, broader, and encompass a wider array of dementia-specific issues, including more symptom management and psychosocial support. The focus of our intervention is targeted specifically on improved ACP communication with patients with ADRD and their families. In addition, our intervention used video-based scenarios to demonstrate the core communication skills, which will allow for participants to see these skills in action and will improve the intervention's reach.
Our results are similar to a small cluster randomized controlled trial of an educational intervention for Dutch general practitioners, which increased ACP initiation and discussions of nonmedical and medical preferences for patients with ADRD. 26 However, this intervention required two 3-hour workshops involving only physicians and nurses, and only targeted late-stage dementia after the involvement of a surrogate decision maker. Our training provides ACP guidance across the spectrum of ADRD and included team-based approaches, favored to increase efficiency and efficacy, by including social workers and nurses. 37 Our qualitative feedback highlighted the need to further focus on role-specific issues if future training is offered to diverse health care disciplines.
This study's limitations include that the training targets some but not all of the core competencies of dementia skills. 38 Although this study captured evidence for practice change, we did not assess patient and caregiver outcomes such as quality of communication, or satisfaction that they were heard and understood in the discussion. 39 We could not to assess the impact of the intervention on social workers or nurses directly and only examined physician/APPs' ACP practices. In addition, training was limited to only four hours, whereas the most efficacious clinical communication skills training averages eight hours. 29 Finally, only a limited number of clinicians, volunteering from a limited geographic locale, participated in the study. These clinicians reported on average 20% of their patient panel had ADRD, limiting generalizability.
However, the improvement in documentation of ACP practices and perceived usefulness does suggest that this toolkit may improve ACP in primary care for a more diverse sample of clinicians.
Conclusion
This article presents promising efficacy of the first video-based training in dementia-specific ACP skills for primary care clinicians. Although preliminary, it appears that primary care clinicians can be trained to conduct dementia-specific ACP. Future research will evaluate its effect on other ACP skills and in a larger population of clinicians. Possible modifications to the intervention may include remote training versions in a larger cohort of primary care clinicians.
Footnotes
Acknowledgments
We thank our advisory board for their invaluable assistance with this project: Wendy Anderson, MD; Tony Back, MD; Nicole Fowler, PhD, MHSA; Lisa Gwyther, MSW, LCSU; Susan Mitchell, MD, MPH; Lynnette Russell; Rebecca Sudore, MD; Alexia Torke, MD, MS; and Heather Young, PhD, RN. We thank Horizon Productions and VitalTalk for their support and efforts as well.
Funding Information
The Gordon and Betty Moore Foundation funded this study (Award #6419). We thank them for advice along the course of the project. The funding sources for this study had no role in design and conduct of the study, data collection, management, analysis, and interpretation of data, or in preparation, review, or approval of the article.
Author Disclosure Statement
No competing financial interests exist.