
Abstract
The family meeting is an essential component of effective palliative care (PC); however, medical students and junior doctors-in-training often consider leading a family meeting to be a daunting task. The old “see one, do one, teach one” axiom should not apply in preparing trainees to conduct a family meeting. After a review of the literature on established PC curricula, trainee perceptions of their PC educational experiences, and documented educational interventions in preparing trainees to conduct a family meeting, we have compiled a list of 10 tips for clinical educators to consider in assisting their students to feel better equipped to conduct productive family meetings.
Introduction
The family meeting provides an opportunity for the exchange of information regarding the patient's condition and clarifying goals of care between key family members and the interdisciplinary health care team. Thoughtful approaches to the family meeting have been associated with improved family satisfaction and mental health outcomes 90 days after the death of a loved one.1,2 Proactive family meetings may be an element of holistic patient care in many areas of health care, including critical care, pediatrics, geriatrics, and psychiatry, but are most often incorporated into the care of children and adults with life-altering or life-limiting conditions. The family meeting is an essential component of effective palliative care (PC) and can be especially helpful as the patient nears the end of life (EOL).
Facilitating family meetings is an important skill to be mastered by all physicians, nurses, and other health care professionals, but is particularly vital for those who care for patients with serious illnesses and their families. Conducting a family meeting requires the integration of many advanced skills, including group facilitation, counseling, providing a clear explanation of often complex medical and prognostic information, redirecting conversation, problem-solving, conflict resolution and mediation, and providing guidance in decision making. 3 Junior doctors-in-training often report feeling uncomfortable and unprepared to lead family meetings and to engage in difficult conversations about death and dying due to inadequate training in these domains. 4
As early as the mid-1990s, educators began discussing the inadequacies in PC training in undergraduate medical education 5 ; however, in the intervening years, there have been only a few published studies on the development of curricula to address communication, particularly pertaining to the facilitation of family meetings, even in fields in which this ability is an Entrustable Professional Activity.6–8 Although the development of a comprehensive curriculum is beyond the scope of this study, it is our hope that the following 10 tips will provide a foundation for how to provide worthwhile educational opportunities to trainees of all disciplines learning how to navigate family meetings.
Tip 1: Seek to Integrate PC Education Into Preexisting Curricula to Provide Learners with a Basic Fund of Knowledge of PC Communication Skills
Surveys of medical educators indicate that 75% of the faculty feels that EOL education is important for medical students and 93% agree that it is important for junior doctors-in-training. 9 When asked to describe one change that would most improve EOL care education, students and doctors-in-training most frequently cited inclusion of a formal curriculum and required rotations in hospice or PC, more trainee exposure to dying patients and their families in hospital, home, and hospice settings, direct observation and feedback from their supervisors, and opportunities to learn from PC specialists. 9 We would argue that education goes beyond just obtaining a “Code Status”; rather, all trainees need to have basic skills in three areas: delivering bad news including discussing prognosis, having goals of care conversations, and conducting a family meeting.
With the increasing prevalence of burnout among medical trainees already burdened with busy schedules and multiple competing interests, finding a place to incorporate elements of quality PC education may be difficult. Existing curricula need not be completely overhauled to include meaningful PC educational experiences. Models exist for integrating educational programs into relevant clinical rotations, such as geriatrics, allowing trainees to practice their learning in real patient situations. 10 In addition, the incorporation of brief educational interventions integrated into a medical intensive care unit (ICU) rotation resulted in improved physician trainee comfort and preparation in leading family discussions.4,8
Tip 2: Supplement Your Didactic Teaching with Experiential Learning Opportunities So Your Learners Can Practice Their New Skill Set
The traditional models of didactic teaching and role modeling are not ideal for trainees to develop the complex nuanced skills necessary to conduct a successful family meeting. Skills such as delivering bad news and giving prognostic information need to be practiced. These skills are best learned in an experiential format with formative feedback. 11 Feedback should be given around whether the learner responded to emotion or provided empathy.
In the undergraduate medical education setting, Objective Structured Clinical Exams (OSCEs) have shown utility in teaching students how to lead a family meeting, with students noting that the simulated practice was useful considering their lack of experience delivering bad news and limited participation in family meetings during their clinical training. 3 Vital Talk has created a robust library of videos, which learners can access to see these skills first-hand. 12 Simulations can also provide a venue for assessing components of communication skills such as empathy, which are otherwise difficult to evaluate. 13
A study of junior doctors-in-training completing a rotation in an ICU who were randomized to a simulation or didactic educational experience suggested that trainees were more likely to report acquisition of new communication skills after a simulated family meeting and debrief as compared with a didactic session without simulation. 4 In addition, an internal medicine residency program deploying a communication skills curriculum that utilized an active learning model resulted in increased learner engagement as compared with a traditional lecture model. 10
Tip 3: Incorporate Creative or Unconventional Teaching Methods to Help Trainees Recognize Their Own Values and Biases
Game-style activities, 14 workshops simulating book club discussions, 15 scripted role-play, 16 and other unique approaches to self-reflection are reported to be effective in helping trainees gain insightful knowledge about their own perceptions of patient care. Go Wish, which is a set of 36 cards with short statements of factors that may be important to people affected by life-threatening illnesses, 17 has shown utility in both the clinical 18 and educational 19 settings. Specifically, second year medical students stated that completing a Go Wish activity helped them realize that values that they had considered to be universal were actually quite different from the values of their peers. 18 “Death over dinner” conversations incorporate humor and are well received by all age groups. 20
One model of an EOL workshop designed for Family Medicine intern physicians has had success in eliciting insightful conversations after asking attendees to anonymously fill out their own death certificate or durable power of attorney for health care paperwork. 21 This group also reported successful introspective conversations after viewing clips from familiar movies and TV shows demonstrating themes of terminal illness and dying, followed by discussion similar to that of a book club. Subsequent to participation in scripted role-plays, clinicians have reported increased understanding in how to conduct family meetings and how to deliver bad news. This experiential learning technique has proven especially useful for foreign medical trainees whose primary language was not English. 22
Tip 4: Choose a Nonconfrontational Learning Environment So That You Can Give Your Learner Feedback That Will Help Them Grow
Just as care should be taken to establish conditions to support a productive family meeting, the educational environment in which students are exploring sensitive topics and practicing family meeting skills should be optimized. 23 For example, give the learner space to ask questions and feel safe to explore their feelings, perhaps beginning with asking learners specifically how they thought the conversation went, what went well, or what part was most difficult. Faculty should facilitate a supportive environment, remaining alert to the fact that some topics may provoke an emotional response in students. For group activities, set ground rules that promote respect for self and others, encouraging both introspection and sharing. Asking observers to comment first on what the person running the simulated meeting did well can create a safe learning environment. Plan ahead to provide students time to prepare for the activities and to model appropriate group communication skills.
Tip 5: Interdisciplinary Educational Teams Are a Valuable Tool and Should Be Used As Often As Possible
Studies have specifically demonstrated the value of including a wide range of interdisciplinary input in family meetings to achieve primary goals such as facilitating shared decision making and providing emotional support to the family.24,25 Consider the benefit of the combination of skills and viewpoints of multiple disciplines in facilitating productive conversations. For example, the social worker and chaplain on the team can add a different perspective, helping to move the conversation in a different direction or hold space if clinicians are missing cues from the patient or family.
Forums for teaching trainees how to conduct a family meeting provide a range of opportunities for students to learn with and from members of different disciplines. An educational intervention comparing outcomes of a mixed group of medical and social work students with homogenous control groups revealed improved understanding of professional roles and collaborative behavior in the interprofessional group. 26 Engage colleagues from other disciplines in the institution such as nurses, social workers, therapists, and chaplains to explore options for collaboration.
Tip 6: Teach Trainees to Ask About Cultural and Religious Beliefs and Practices That May Have Implications for Care
Student performance in family meeting OSCEs revealed that medical students were uncertain about addressing spiritual or religious issues, identifying a key area for improvement in current EOL educational experiences. 3 Trainees should understand the difference between spirituality and formal religious affiliation, including the knowledge that each patient may exist at different points along the spectrum of one or both concepts. Trainees can be taught when patients' issues should be shared with a chaplain and how to ask for help from other members of the team. Studies have shown that the majority of patients would like their medical team to support their spiritual needs, with an even greater percentage indicating that attention to spiritual health would result in improved overall satisfaction with care. 27
Inclusion of chaplains and formal spiritual assessments in patient care should be encouraged, but trainees should feel empowered to inquire themselves about their patients' spiritual concerns. The FICA (Faith, Importance/Influence, Community, Action/Address issues) Spirituality tool and the HOPE (sources of Hope, Organized religion, Personal spirituality, Effects on medical care and end-of-life decisions) tool can be especially useful in helping health care providers integrate these conversations into time-sensitive encounters. 28 In addition, the underutilization of PC services among ethnic minorities has been well described, and is often attributed to factors such as language barriers, religious differences, distrust of health care professionals, and physician discomfort. 29 Bringing attention to the need to address these issues among ethnic minorities early in trainee education could improve communication and allow for more meaningful interactions for both providers and patients.
Tip 7: Encourage Learners to Reflect on Their Own Feelings Before and After Conducting a Family Meeting
Just as it is important for clinicians to reflect upon their own feelings of grief, anxiety, or guilt before discussing EOL care with families, 30 encouraging trainees to examine their own values and biases as they learn how to conduct family meetings is crucial. Failure to self-examine may lead to clinicians avoiding discussions of death and other difficult topics. A qualitative analysis of barriers to using the word “dying” among junior doctors-in-training identified eight roadblocks: uncertain prognostication, fear of family reaction, discomfort with the word “dying,” family denial, family reliance on religion/hope/miracle culture, a specific patient characteristic such as young age, family lack of understanding, and fear of reducing family confidence in provider. 4 Poor communication, particularly around the time leading up to a person's death, is a well-documented area for improvement. 3 Equipping trainees with the emotional intelligence to identify and process their own feelings prepares them to engage in the emotional labor necessary to help families navigate their own emotional landscapes surrounding the time of a loved one's death. It also represents a space through which one can improve family satisfaction 24 and increase opportunities to broach difficult topics with patients and their families. 31 Formal opportunities to reflect, such as Schwartz Rounds, have been shown to promote interprofessional collaboration and well-being. 32
Tip 8: Provide Learning Anchors as a Framework for Learners to Recall Critical Elements on How to Conduct a Meeting or Give Bad News
Help students find a framework that assists with recall of critical elements of the task of conducting a family meeting. Mnemonics such as SPIKES 33 (Fig. 1) or REMAP 34 (Fig. 2) frame the complex process of family meetings in a concrete way that promotes recall in a high-stress situation. Guide students through the process of facilitating family meetings by encouraging preconference preparation, providing standardized note-taking templates to ensure all pertinent information is readily available, and promoting consistent postconference documentation.
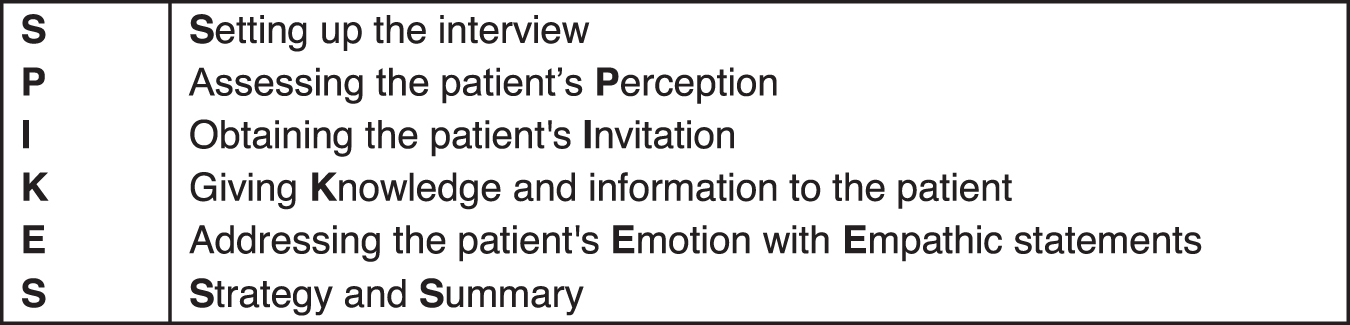
SPIKES mnemonic for delivering bad news.
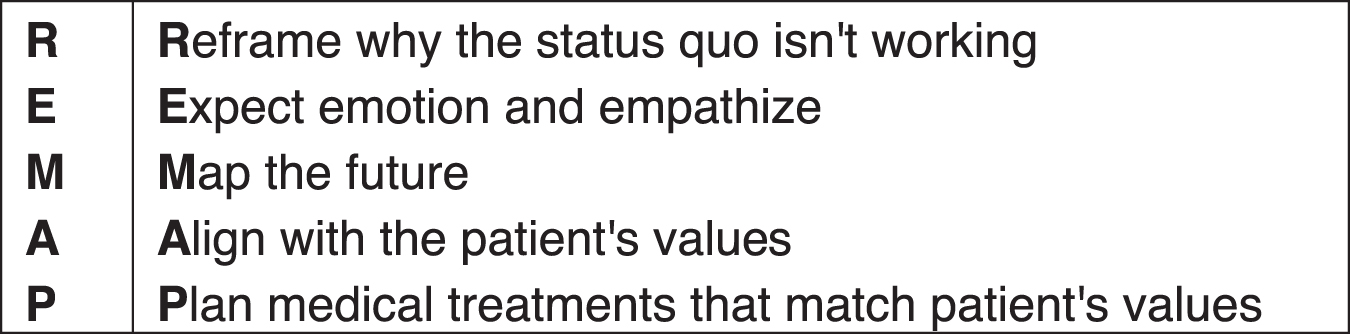
REMAP tool for addressing goals of care.
Tip 9: Remember to Debrief with Trainees After the Family Meeting and Provide Both Reinforcing and Corrective Feedback
The process of debriefing trainees on their performance in family meetings (real life or simulated) is integral to skill refinement; however, reports have shown that nearly half of all medical students and one third of junior doctors-in-training never received any feedback after EOL discussions with patients. 9 Feedback and debriefing can encourage self-reflection and help the trainee identify areas for improvement. Peer-to-peer feedback in the setting of prior peer-learning relationships can also provide an avenue for specific input about communication skills that may prove useful in group simulation or role-play settings. 35
In addition, it is important for medical educators to debrief among themselves after educational sessions with trainees to explore the effectiveness of the session and suggest improvements. An entire hour was devoted to debriefing at a three-hour train-the-educator workshop designed to help educators develop a customized communication skills curriculum to target their own learners' needs in PC or other specialties that engage in challenging family conversations. Following this component of the workshop, many participants highlighted their intention to begin debriefing among themselves as educators after they debrief learners who participate in a simulated family meeting, to share what went well and how to improve future training sessions. 11
Encouraging post-family meeting debriefings in the training environment can set the precedent for a useful habit of debriefing after real-life family meetings. Postmeeting discussions can provide an appropriate venue for team members to discuss any internal conflict, to align their future responses to any difficult or unexpected questions asked by the family during the meeting, and to assess team performance and make adjustments for future meetings. 36
Tip 10: Use Assessment Tools to Track Your Learners' Progress and Identify Areas for Them to Improve
Pre-/post-self-assessment in any educational intervention is recommended to follow up on self-confidence, comfort, preparedness, and knowledge of participants. 37 The SEGUE (Set the stage, Elicit information, Give information, Understand the patient's perspective, End the encounter) Framework 38 has been considered a gold standard for assessing communication. As the need for formal education in PC skills has received more attention in recent years, additional instruments tailored to specific clinical and educational settings have been developed and validated. Examples include the Family Meeting Behavioral Skills Checklist to assess the advanced communication skills of fellows in facilitating family meetings in the ICU, 39 the Family Meeting Assessment Tool to assess trainee's family meeting skills using standardized patients, 40 and the Communication Assessment Tool for assessing surgery trainees' interpersonal communication skills in a simulation of delivering bad news. 41
Conclusion
Conducting a family meeting is an essential clinical skill. Residents and students can be taught this fundamental competency and thus provide more comfort and communication to families and patients. Mastery of this skill is necessary for excellent patient and family care; these 10 tips should help educators provide more meaningful opportunities for medical trainees as they learn how to conduct a family meeting (see Table 1).
Summary of 10 Tips for Teaching Palliative Care Trainees
Footnotes
Acknowledgment
Thank you to Hannah Coyne for her wisdom and expert review.
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.