
Abstract
Background:
Simple methods to help teams identify patients with goals of care (GOC) conversation needs are lacking.
Objectives:
To develop a tool to identify hospitalized patients who may benefit from GOC conversations.
Methods:
The Preference-Aligned Communication and Treatment (PACT) Conversation Trigger Tool was implemented as part of a quality improvement initiative in 10 Illinois hospitals and validated in a cohort of patients admitted to the coordinating site's oncology unit (n = 135).
Results:
The tool was reliable and acceptable to clinicians using it across sites. Thirty percent (n = 40) of patients screened at the coordinating site's oncology unit triggered positive. These patients were more likely to have a do-not-resuscitate order (43% vs. 11%) and palliative care consult (53% vs. 20%) and had lower mean survival time (125 vs. 248 days) than those who did not trigger (p < 0.001).
Conclusions:
The tool is reliable, acceptable, and can identify hospitalized oncology patients who may benefit from GOC conversations.
Introduction
For patients with serious illnesses, optimal communication with clinicians is a key component of high-quality care.1,2 Goals of care (GOC) conversations between clinicians and seriously ill patients have been associated with improvements in patient experience, 3 reductions in anxiety and depression, 4 and possible reductions in health care spending.5,6 Frequently cited barriers to discussing GOC include prognostic uncertainty and limited physician time.7,8
Systematic interventions focused on stratifying those who have a short prognosis and may benefit most from GOC conversations are needed. A variety of tools are available for prognostication9–12 and identifying patients with palliative care needs.13,14 Many of these, however, are difficult to apply at the time of hospital admission due to need for laboratory results or physician input,15–17 creating missed opportunities for nurses or social workers to facilitate these conversations earlier in the hospitalization.
The Preference-Aligned Communication and Treatment (PACT) project was a quality improvement intervention designed to promote and standardize GOC conversations among a broad spectrum of clinicians in the inpatient setting. The PACT Conversation Trigger Tool was developed as part of this project to screen for GOC conversation needs on hospital admission. In this study, we describe the reliability and acceptability of the PACT Conversation Trigger Tool across sites, as well as its validity within a subpopulation of patients with advanced cancer at the coordinating site.
Methods
The PACT faculty (10 experienced palliative medicine physicians) reviewed publicly available screening criteria, with a goal of developing a tool that could be quickly and accurately completed by any admitting clinician without extensive chart review or specialized medical knowledge. The PACT tool was adapted from consensus criteria for consideration of palliative care consultation, with a focus on variables suggesting unmet communication needs, rather than symptoms. 18
Accordingly, the tool includes both medical comorbidities and markers of declining function. The faculty reached consensus about assigning points for each factor; two for each marker of functional decline and one for each major comorbidity. A total of three points was the threshold for triggering a GOC conversation because that would indicate at least one chronic illness with clinical decline or a combination of three or more chronic illnesses that would increase the risk of complications.
The tool was implemented at 10 sites as part of the PACT Project. For more information on the PACT process, please see Supplementary Appendix SA1. Teams at each site were provided education on the rationale and use of the tool through centralized training at an initial conference and web-based modules. The tool was completed within two days of admission, and patients who triggered positive were subsequently referred for a GOC discussion. The study was deemed exempt from review by the Northwestern University Institutional Review Board.
Reliability
To evaluate inter-rater reliability of the tool, 10 patients were double-scored using the tool at each site (n = 100). Each trigger criterion was evaluated for reliability using Cohen's kappa.
Acceptability
Acceptability of the tool was evaluated using an investigator developed 10-item survey derived in part from two published acceptability instruments.13,14 The survey was completed by clinicians who used the tool at each site. Participants used a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree) to rate the extent to which they agreed with each statement (e.g., “The tool is easy to understand.”).
Validity
As an initial assessment of validity of the tool, chart reviews were conducted on patients with solid tumors admitted to an oncology unit and screened with the tool at one site, an academic tertiary medical center, during the first six months of project implementation (October 1, 2015 through March 31, 2016), before initiation of GOC conversations. This single site was chosen because it was the coordinating site, and investigators had direct access to medical records.
Chart reviews were conducted between March and April of 2017. Data were collected on the index admission, subsequent readmissions (through December 2016), and patient mortality. Patient demographics were summarized using descriptive statistics and comparisons between groups were based on t tests and chi-square tests. Survival was evaluated using the Kaplan–Meier method. 19 Statistical analyses were performed using SPSS, version 25.
Results
Reliability
The PACT Trigger Tool demonstrated moderate to high (0.73–1) reliability scores across the risk indicators. “Frequent admissions” showed the lowest reliability at 0.73 (Table 1).
Preference-Aligned Communication and Treatment Trigger Tool Reliability
Scores of ≥3 points were considered positive. Reliability was assessed using Cohen's kappa (k).
COPD, chronic obstructive pulmonary disease; PACT, Preference-Aligned Communication and Treatment.
Acceptability
One hundred eighty-five providers were surveyed (94.6% RNs); the completion rate was 77% (range 60–100%). The location where screening occurred (one per site) included general medical/surgical floors, cardiac telemetry, solid-tumor oncology, and intensive care units. Exploratory factor analysis with varimax rotation of the survey results yielded two factors reflecting the ease of completion and usefulness of the tool (Cronbach's α = 0.82 and 0.90, respectively). These factors demonstrated that providers found the tool useful (M = 4.07, standard deviation [SD] = 0.73) and easy to complete (M = 4.24, SD = 0.67).
Validity
One hundred thirty-five patients were screened at the coordinating site during the first six months of implementation, of which 40 patients (30%) triggered positive. Patient demographics are shown in Table 2.
Patient Demographics at Index Admission
SD, standard deviation.
On the index admission, patients who triggered positive were more likely to have a do-not-resuscitate order (43% vs. 11%) and palliative care consult (53% vs. 20%) than those who did not (p < 0.001). Of those who triggered positive, 35% died or were discharged with hospice support (6/40 died during hospitalization; 8/40 discharged to hospice), compared with 6% (1/95 died; 5/95 discharged to hospice) in the group that did not trigger positive (p < 0.001). No significant difference was found between groups in length of hospitalization or rate of ICU transfers. Patients who triggered positive had a significantly lower mean and median survival time (M = 125 days, Mdn = 69 days,) than those who did not (M = 248 days, Mdn = 240 days, p < 0.001; Fig. 1).
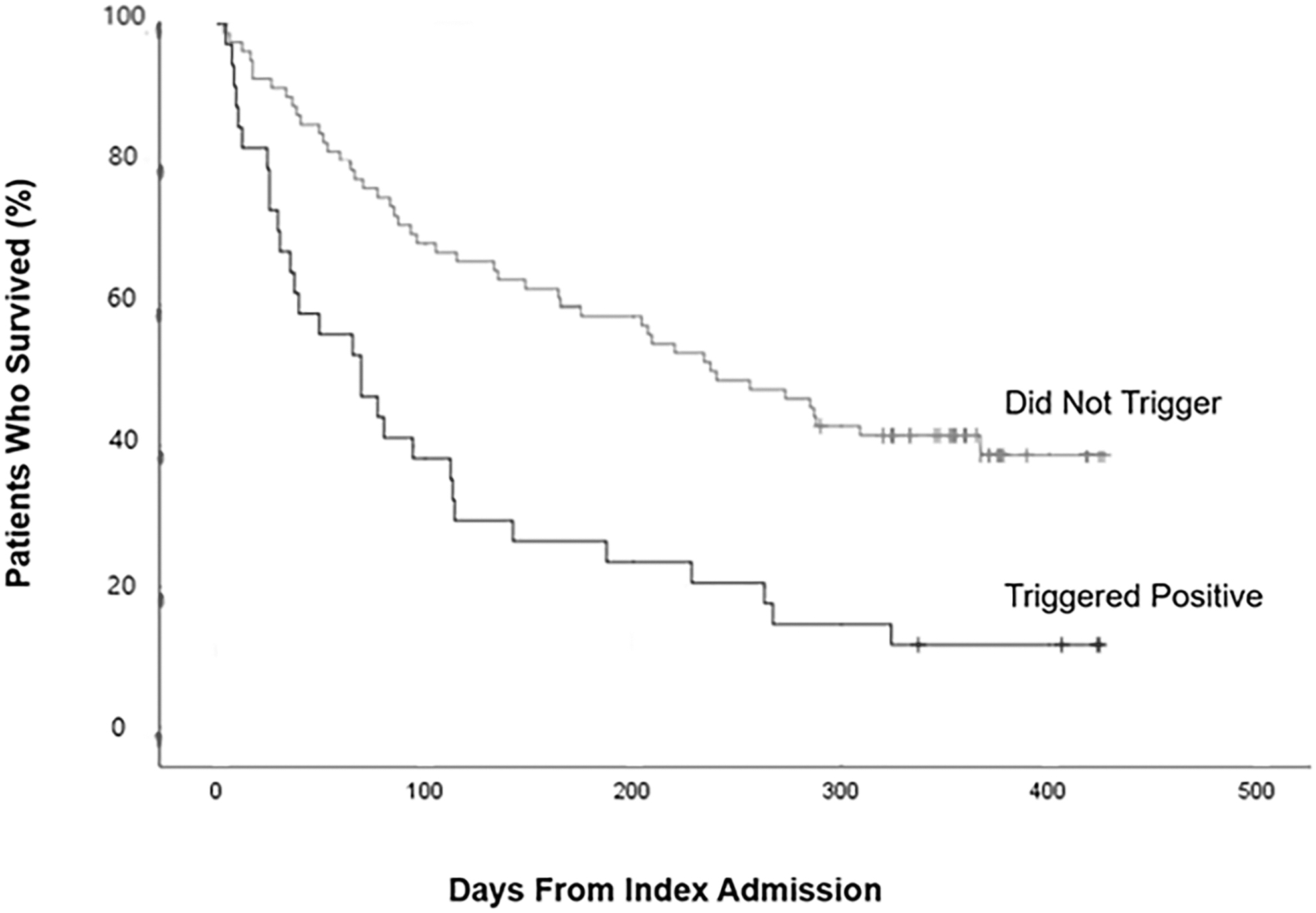
Overall survival of patients who triggered positive versus who did not trigger at the index admission. Shown are the Kaplan–Meier curves for overall survival. The tick marks indicate censored data.
Discussion
The PACT Conversation Trigger Tool was shown to be reliable and acceptable to clinicians of multiple disciplines across 10 hospital sites and showed promising validity in a single site analysis. In a population of hospitalized patients with metastatic cancer, the PACT tool identified patients in the later stages of illness who may benefit most from a GOC conversation. A variety of prognostic tools have been developed previously, particularly for patients with cancer. However, these tools were developed for patients already known to be at high risk of short-term (30-day) mortality.9–11
Other tools have been developed to identify patients who may benefit from expert palliative care consultation, often with a focus on symptom management or end-of-life care.13,14,18,20,21 Therefore, the utility of these tools in stratifying hospitalized patients who may benefit from a GOC conversation is unclear. Even the simplest of screening tools—“The Surprise Question” (“Would I be surprised if this patient died in the next 12 months?”)—has potential drawbacks, 4 including its variable performance as a predictive tool for death, variable interobserver reliability, need for specialist input, and reluctance of some clinicians to answer. 22
The PACT tool may represent a promising addition to available tools, as it has several unique features. It is designed to be used for patients with an array of serious illnesses without the need for expert knowledge or familiarity with external guidelines.23,24 It can also be completed without the need for physician input and integrated into the electronic medical record (EMR) allowing for incorporation into admission workflow without laboratory testing or in-depth chart review. Using such a tool on admission can help identify patients who may benefit from targeted communication interventions during the hospitalization.
Although GOC conversations should be introduced earlier, they often are not,25,26 and hospitalization represents an opportunity to prompt discussion when clinicians and patients are available and a clinical change may prompt discussion. 27 Although one may argue that both groups in the validity analysis had a relatively poor prognosis, the tool identified patients with a significantly shorter prognosis who would benefit most from the limited resources to hold these discussions.
This study represents the practical experience with this tool and has several limitations. The cutoff for triggering positive was determined by expert discussion rather than empirical study. Reliability of one item (frequent admissions related to one of the aforementioned illnesses: ≥2 admissions within three months for the same condition/disease) was poor perhaps due to use of the “≥” symbol. This was changed on a subsequent version of the tool not included in this analysis.
This study only assessed validity using mortality and outcomes determined by chart review within one site; therefore, generalizability to other patient populations and settings is limited. Validation of the tool in patients hospitalized with noncancer diagnoses, as well as in the outpatient setting, will be necessary to understand its utility in these settings. Future research will assess the impact of these GOC conversations, with the hope of empowering patients and clinician champions to better align care with values at the end of life.
Conclusion
The PACT Conversation Trigger Tool was found to be reliable and acceptable across diverse hospital sites, and able to identify hospitalized oncology patients in the later stages of illness who may benefit from a targeted communication intervention. A larger validity study including other patient populations and evaluation of the impact of communication interventions on patient outcomes are needed.
Footnotes
Authors' Contributions
All authors made substantial contributions to the design of the project, data acquisition and analysis, drafting of the article and revisions. All authors have approved the final version.
Research Ethics and Patient Consent
The Northwestern University Institutional Review Board waived approval for this study as it was not considered research involving human subjects.
Funding Information
This study was supported by Blue Cross Blue Shield of Illinois. The funding source was not involved in the study design, in collection, analysis, or interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.