
Abstract
Introduction:
Peritoneal carcinomatosis (PC) afflicts women with advanced gynecologic cancers. Patients with PC often require ostomies, gastric tubes, or catheters to palliate symptoms, yet patients and caregivers report feeling unprepared to manage these devices. The purpose of this study was to develop and field test the Building Out Lifelines for Safety, Trust, Empowerment, and Renewal (BOLSTER) intervention to support patients and their caregivers after hospitalization for PC.
Materials and Methods:
We adapted components of the Standard Nursing Intervention Protocol with stakeholders and topical experts. We developed educational content; built a smartphone application to assess patients' symptoms; and assessed preliminary feasibility and acceptability in two single-arm prepilot studies. Eligible participants were English-speaking adults hospitalized for gynecologic cancer-associated PC and their caregivers. Feasibility criteria were a ≥50% consent-to-approach ratio and ≥80% outcome measure completion. The acceptability criterion was ≥70% of participants recommending BOLSTER.
Results:
During the first prepilot, BOLSTER was a 10-week intervention. While 7/8 (87.5%) approached patients consented, we experienced high attrition to hospice. Less than half of patients (3/7) and caregivers (3/7) completed outcome measures. For the second prepilot, BOLSTER was a four-week intervention. All (7/7) approached patients consented. Two withdrew before participating in any study activity because they were “too overwhelmed.” We excluded data from one caregiver who completed baseline measures with the patient's assistance. All remaining patients (5/5) and caregivers (4/4) completed outcome measures and recommended BOLSTER.
Conclusion:
BOLSTER is a technology-enhanced, nurse-led intervention that is feasible and acceptable to patients with gynecologic cancer-associated PC and their caregivers.
Introduction
Peritoneal carcinomatosis (PC) affects more than 50% of women with gynecologic cancers. 1 PC occurs when cancer spreads along the peritoneal surfaces, causing bowel obstructions and fluid to accumulate in the abdomen and lungs. Burdensome symptoms include nausea, vomiting, obstipation, pain, and dyspnea. 1 Nonsurgical management includes gastric decompression and removal of ascitic or pleural fluid through paracentesis or thoracentesis. Complications of PC recur in 35% to 77% of conservatively managed patients, requiring repeated emergency department visits and hospitalizations.2–5
Patients whose symptoms are not alleviated by conservative management often pursue palliative surgery. Palliative surgical procedures include ostomy formation or placement of venting gastric tubes for malignant bowel obstructions; nephrostomy tubes to relieve malignant ureteral obstructions; and indwelling peritoneal or pleural catheters to remove recurrent ascites or effusions.2,3,6 These procedures leave patients with complex self-care needs for which they and their caregivers receive little or no training or support. 7 Despite surgical intervention, patients with PC have a median survival of less than one year2–4 and often experience rehospitalization and recurrent symptoms.2,3 In this context, patient-caregiver dyads report distress, helplessness, and unmet needs for information.8,9
Compared to usual care, high-touch care management interventions improve health-related quality of life (HRQoL), symptom management, and survival in outpatients with cancer.10–13 High-touch care entails frequent interactions between patients and clinicians. 14 One example is the Standard Nursing Intervention Protocol (SNIP), in which advanced practice nurses visit patients with cancer at home.11–13 To our knowledge, high-touch interventions have not been tested among patients with complex care needs such as PC. Therefore, the purpose of this study was to develop and field test a scalable, high-touch care management intervention for patients with gynecologic cancer-associated PC: the Building Out Lifelines for Safety, Trust, Empowerment, and Renewal (BOLSTER) intervention. Herein, we describe our process for developing BOLSTER and report the results of two prepilot studies during which we field tested BOLSTER with the target population.
Materials and Methods
Conceptual basis for BOLSTER
BOLSTER was informed by the chronic care model (CCM).15,16 According to the CCM, changes in the domains of self-management support, delivery system design, decision support, and clinical information systems facilitate productive interactions between patients, caregivers, and clinicians. In developing BOLSTER, we aimed to address the four CCM domains (Fig. 1).
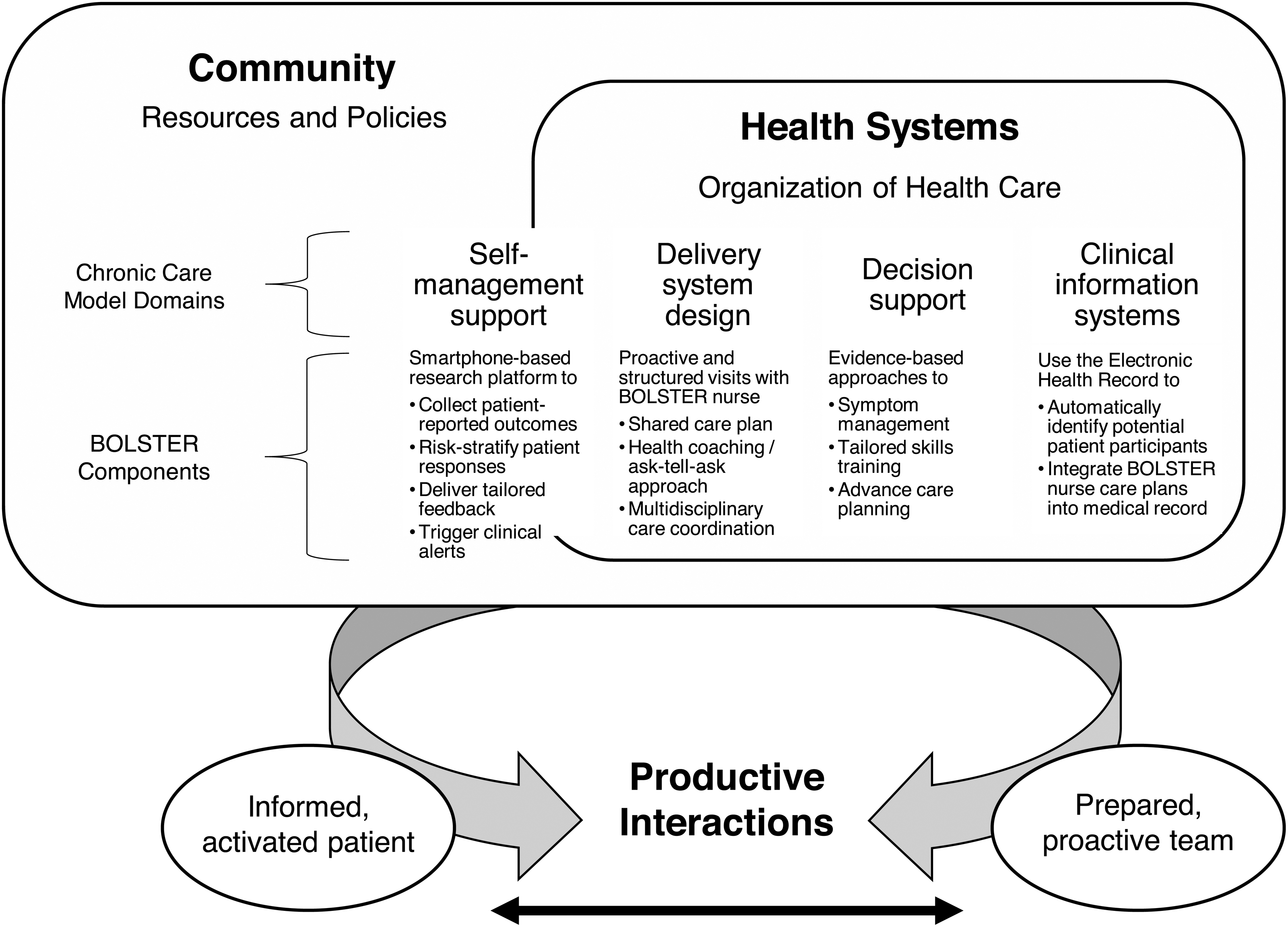
Chronic care model domains addressed by BOLSTER. BOLSTER, Building Out Lifelines for Safety, Trust, Empowerment, and Renewal.
Developing BOLSTER
We used the ADAPT-ITT Framework 17 to adapt an existing high-touch intervention. Table 1 summarizes the phases of ADAPT-ITT, our approach, and the adaptation outcomes. Briefly, we reviewed patient- and caregiver-facing resources for symptom management 18 and complex care skills. Next, we conducted interviews with patients, caregivers, and clinicians to prioritize content. We then assessed goodness-of-fit between the target population and two interventions: SNIP 11 and Educate, Nurture, Advise, Before Life Ends (ENABLE) II. 10 In both interventions, an advanced practice nurse provides education, care coordination, and a written guide to symptom management. However, only SNIP, which was developed to enhance patients' self-management skills following surgery, has been tested in patients with gynecologic cancers. 12 Given the parallels between the needs of our target population and that of SNIP, we chose to adapt SNIP directly, while using ENABLE II as an additional resource.
Developing the BOLSTER Intervention Using the ADAPT-ITT Framework 17
BOLSTER, Building Out Lifelines for Safety, Trust, Empowerment, and Renewal; PC, peritoneal carcinomatosis; PFAC, Patient and Family Advisory Council; SNIP, Standard Nursing Intervention Protocol.
We made three modifications to SNIP to reduce cost, streamline symptom assessments, and promote intervention scalability. First, we trained a baccalaureate-prepared nurse to deliver the intervention rather than an advanced practice nurse. In doing so, we sought to integrate the nurse into the existing care team rather than provide a separate channel for writing orders or prescriptions. Second, we developed a smartphone application to elicit patients' symptoms between visits. Third, we added the option to conduct visits over telehealth using a secure videoconferencing platform. We developed the intervention content in collaboration with patients, caregivers, and topical experts.
Field testing BOLSTER
To field test BOLSTER, we conducted a single-arm prepilot with our target population. Next, we revised BOLSTER in response to participant feedback. We then conducted a second single-arm prepilot to field test the revised intervention. The procedures for both prepilots were approved by the Dana-Farber Cancer Institute Institutional Review Board.
Participants
We recruited patients and their caregivers during acute hospitalizations. In the first prepilot, patients were eligible to participate if they had recurrent ovarian cancer; were receiving antineoplastic therapy; were hospitalized with a complex care need; and were able to identify a caregiver. In the second prepilot, patients were eligible regardless of recurrence status. Caregivers were eligible if they self-identified as the patient's family member or friend. All participants were required to be ≥18 years of age; English speaking; and willing to be audio recorded.
Procedures
Using the electronic health record, we created an automated dashboard to identify inpatients diagnosed with a gynecologic cancer. Each morning, a member of the study team reviewed patients' medical records to identify those with complex care needs. After confirming eligibility with patients' oncologists, a research assistant approached potential participants to describe the study and obtain written informed consent. Caregivers were identified by patients and approached in person or by telephone.
Data collection and measures
Preliminary feasibility
To assess preliminary feasibility, we recorded the number of patients who were screened, eligible, approached, and enrolled. Feasibility was defined as ≥50% enrollment among eligible patients and ≥80% completion of the post-intervention outcome assessments.
Participant characteristics
We assessed participants' demographic characteristics with self-reported age, race, ethnicity, marital status, educational attainment, employment status, annual household income, and religion.
Patient and caregiver outcomes
In the first prepilot, we delivered a 10-week intervention and assessed outcomes at baseline, week 4, and week 10. We subsequently reduced the duration of the intervention in response to patient feedback and due to high attrition to hospice. In the second prepilot, we delivered a four-week intervention and assessed outcomes at baseline and week 4.
We assessed patients' health status using the EQ-5D-5L, which includes five items related to respondents' perceived problems with mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 19 The EQ-5D-5L also includes a visual analogue scale (EQ-VAS) on which patients provide a global assessment of their health. Total scores range from 0 to 100, and higher scores represent better health status. 20
We used the Functional Assessment of Chronic Illness Therapy - Palliative (FACIT-PAL) to assess patients' HRQoL in the first prepilot. The FACIT-PAL is a valid and reliable 46-item measure comprising 5 subscales: physical, social/family, emotional, and functional well-being; and additional concerns in palliative care.21,22 The total FACIT-PAL score ranges from 0 to 184; higher scores indicate better HRQoL. In response to feedback on survey burden during the first prepilot, we used the shorter Functional Assessment of Cancer Therapy-General (FACT-G) to assess patients' HRQoL in the second prepilot. A 27-item measure, the FACT-G, comprised the first 4 subscales of the FACIT-PAL; total scores may range from 0 to 108.
We assessed caregivers' health status using the Short Form 12-Item Survey (SF-12). 23 The SF-12 is a reliable, valid measure of physical and mental health. Items pertain to physical functioning, role limitations due to physical or emotional problems, pain, fatigue, social functioning, and mental health. 24
We evaluated patients' and caregivers' mood with the Hospital Anxiety and Depression Scale (HADS), 25 a 14-item scale that is validated for screening for emotional distress in patients with cancer and their caregivers.26,27 HADS comprises an anxiety and depression subscale; scores range from 0 to 21 for each, with higher scores indicating higher symptom burden. We defined a borderline case as a score between 8–10 and a case as >10 on either subscale.25,26
We used the Caregiver Reaction Assessment (CRA) to assess caregiver burden. 28 The CRA is a valid and reliable 24-item scale comprising 4 subscales that assess the impact of caregiving on self-esteem, finances, family support, and schedule. 29 Subscale totals range from 1 to 5, with higher scores indicating a more positive impact on self-esteem and a more negative impact on finances, family support, and schedule.
Preliminary acceptability and perceived effectiveness
At the end of each prepilot, we asked participants about the extent to which they were satisfied with, perceived benefit from, and would recommend BOLSTER to other patients and caregivers.30,31 We defined acceptability as ≥70% of participants reporting they would recommend BOLSTER. Concurrent with these assessments, we conducted individual, semistructured interviews with participants to identify potential barriers to acceptability and implementation. Participants were prompted on the length of the assessments, visit format, educational materials, smartphone platform, and interactions with the nurse. Interviews were recorded, de-identified, and transcribed.
Data analysis
We summarized participant characteristics and measures of preliminary feasibility, acceptability, and perceived effectiveness using descriptive statistics. We did not compare outcomes preintervention and post-intervention in this underpowered prepilot study. Finally, we reviewed interview transcripts for participants' suggestions to improve BOLSTER.
Results
Prepilot I
Intervention
The first iteration of BOLSTER was a 10-week intervention comprising 12 nurse visits (Supplementary Data S1). The initial visit took place in the patient's home. Subsequent visits took place over telehealth, in the oncology clinic, or by phone. Caregivers were encouraged to attend. During each visit, the nurse set the agenda, assessed symptoms, provided tailored symptom education and skills training, guided the patient and caregiver to set goals for the next visit, and adopted a teach-back method to ensure comprehension. Afterward, the nurse e-mailed an update to the patient's oncologist and documented the visit in the medical record. Between visits, patients received daily prompts to report symptoms using the smartphone application.
The application advised patients with severe symptoms to contact their oncologist. To reinforce nurse teaching, participants received a study binder containing printed educational content, and access to a study website with electronic versions of the educational content and patient videos.
Preliminary feasibility
During screening, we identified 16 potentially eligible patients. Oncologists indicated 4/16 (25%) should be approached later and 3/16 (19%) did not have caregivers. Ultimately, 8 patients were approached, and 7/8 (87.5%) consented to participate. We excluded one enrolled patient who was unable to complete the baseline assessment due to cognitive impairment, leaving six patients and caregivers in the first prepilot. One patient transitioned to hospice shortly after enrollment, leaving 5/6 (83.3%) patients and caregivers to complete the four-week outcome measures. Two additional patients died during the study period, leaving 3/6 (50%) patients to complete the 10-week outcome measures and debriefing interview. Likewise, 3/6 (50%) caregivers completed the 10-week outcome measures. Four of six (67%) caregivers, one of whom was bereaved, completed a debriefing interview.
Participant characteristics
Patients were an average of 64 (SD = 7.31) years old; White, non-Hispanic (6/6, 100%); married (5/6, 83%); college graduates (4/6, 67%); retired (4/6, 67%); earning at least $51,000 annually (4/6, 67%); and Catholic (4/6, 67%). Caregivers were an average of 64 (SD = 6.63) years old; White, non-Hispanic (6/6, 100%); married (6/6, 100%); college graduates (4/6, 67%); retired (4/6, 67%); earning at least $100,000 annually (3/6, 50%); and Catholic (3/6, 50%).
Participants' health status, HRQoL, mood, and caregiver burden at baseline are described in Table 2 and Figure 2. Briefly, 3/6 (50%) patients and 2/6 (33%) caregivers met case criteria for anxiety, while 1/6 (17%) patients met case criteria for depression. Patients' mean FACT-G physical well-being, emotional well-being, and functional well-being subscale scores were 17.20 (SD = 10.62), 11.80 (SD = 7.98), 12.40 (SD = 4.67), respectively, each of which are below the 25th percentile FACT-G subscale scores identified in a population-based sample of adult females with cancer. 32
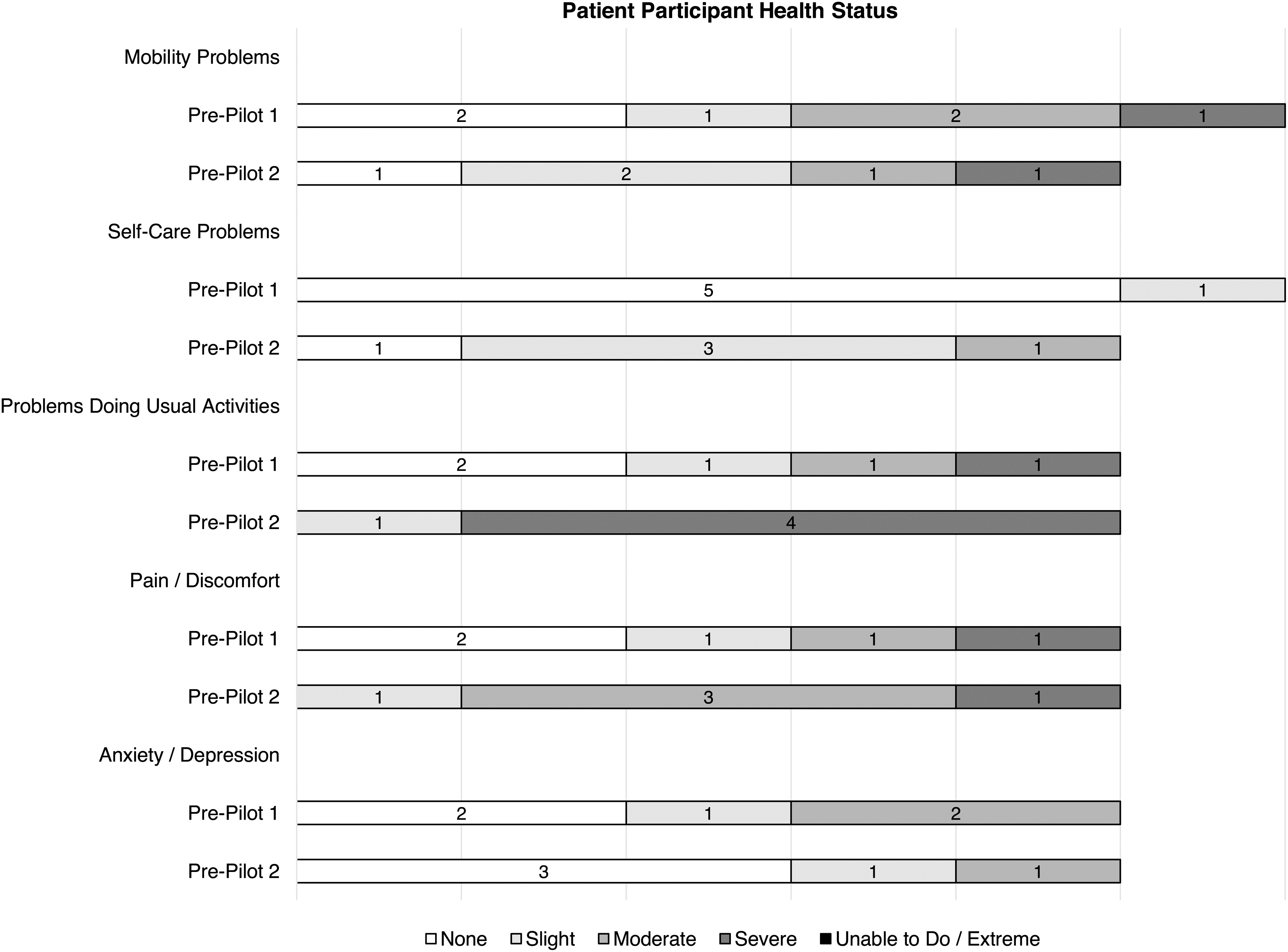
Patient participant health status at baseline as measured by the EQ-5D-5L.
Baseline Participant Health Characteristics
—, Not assessed; CG, caregiver; EQ-VAS, EQ-5D-5L Visual Analogue Scale; FACIT-PAL, Functional Assessment of Chronic Illness Therapy - Palliative; FACT-G, Functional Assessment of Cancer Therapy-General; HADS, Hospital Anxiety and Depression Scale; M, mean; PT, patient; SD, standard deviation; SF-12, Short Form 12-Item Survey.
Preliminary acceptability and perceived effectiveness
All (3/3, 100%) patients and 2/4 (50%) caregivers recommended BOLSTER, and 3/3 (100%) patients and 3/4 (75%) caregivers were satisfied with the BOLSTER sessions. One of three (33%) patients and 3/4 (75%) caregivers agreed BOLSTER improved the patient's symptoms. Two of three (67%) patients and 2/4 (50%) caregivers agreed BOLSTER helped the patient understand and cope with their illness; and 1/3 (33%) patients and 2/4 (50%) caregivers agreed BOLSTER helped the patient plan for the future. In debriefing interviews, several patients said the home visit was unnecessary because they were receiving home health services. Participants found the amount of information on the BOLSTER website overwhelming, and several patients wished they had been able to access BOLSTER earlier in their disease trajectory.
Prepilot II
Intervention
We reduced the intervention duration in response to patient feedback that the first month was most helpful, and due to high attrition during the first prepilot (Supplementary Data S1). The second iteration of BOLSTER was a four-week intervention comprising six visits (Fig. 3). In response to participant feedback, we eliminated the home visit, study binder, and website. We then modified the smartphone application to allow the nurse to deliver tailored educational content to patients after each visit.
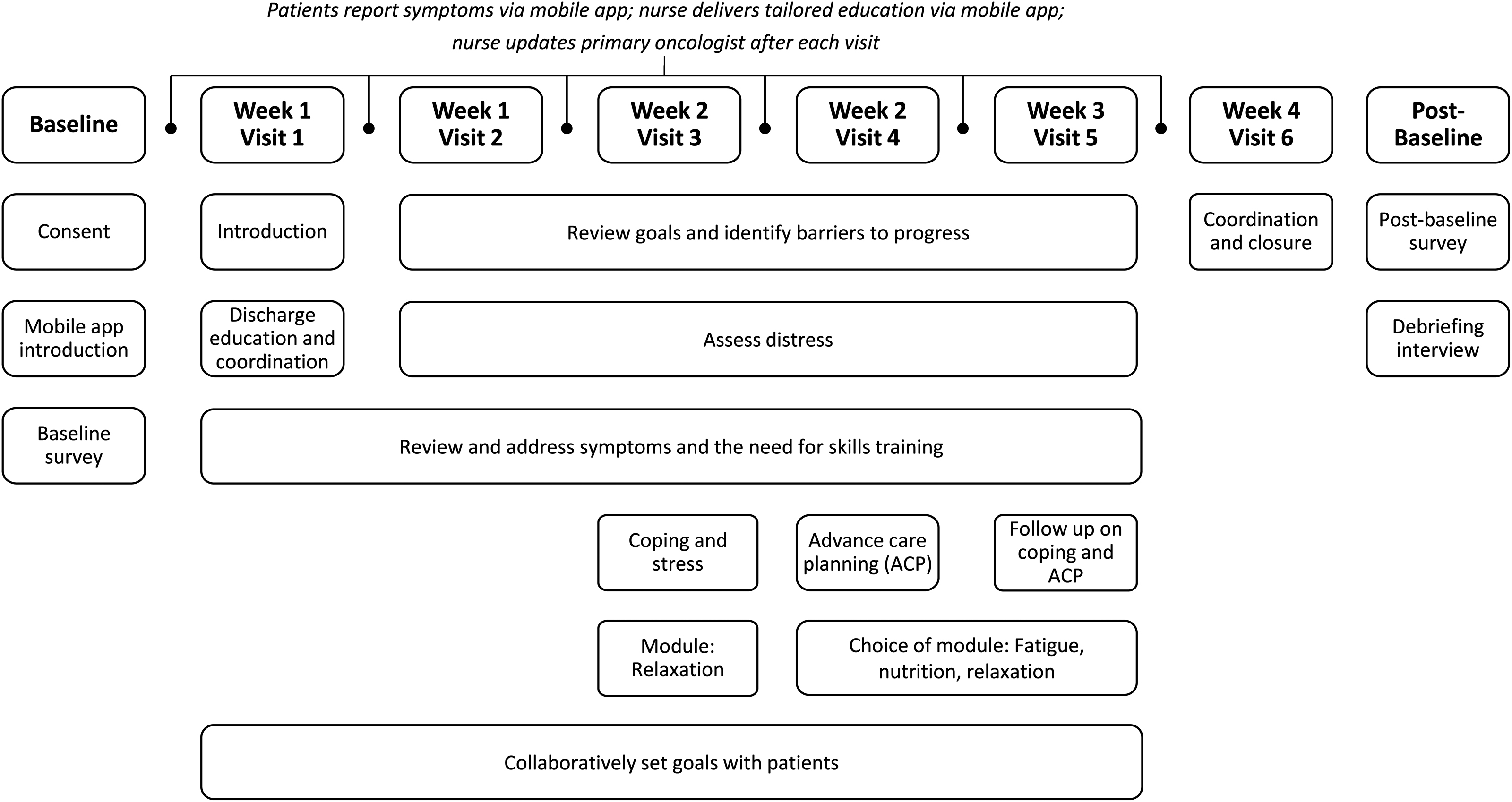
Final BOLSTER intervention schema.
Preliminary feasibility
During screening, we identified 16 potentially eligible patients. Of these, only 11/16 (81%) were eligible because 4/16 (25%) lacked a caregiver and 1 oncologist reported a patient was “too overwhelmed” to approach. Among the 11 remaining, 4/11 (36%) were discharged before they could be approached, and 1 was discharged to hospice. Ultimately 7/11 (64%) were approached and 7/7 (100%) consented to participate. Among consented patients, two of seven withdrew before participating in any study activities because they were “too overwhelmed.” Five patient-caregiver dyads completed the second prepilot. We excluded data from one caregiver who completed the baseline survey with the patient's assistance because the caregiver was illiterate. Among the remaining participants, the rate of instrument completion was high: 5/5 (100%) patients and 4/4 (100%) caregivers completed the four-week outcome measures and 5/5 (100%) patients and 3/4 (75%) caregivers completed a debriefing interview.
Participant characteristics
Patients were an average of 58 (SD = 14.03) years old; White, non-Hispanic (4/5, 80%); married (5/5, 100%); college graduates (3/5, 60%); retired (2/5, 40%); earning at least $100,000 annually (4/5, 80%); and Catholic (2/5, 40%). Caregivers were an average of 62 (SD = 12.48) years old; White, non-Hispanic (3/4, 75%); married (4/4, 100%); college graduates (3/4, 75%); working full time (2/4, 50%); earning at least $100,000 annually (2/4, 50%); and Catholic (2/4, 50%).
Participants' health status, HRQoL, mood, and caregiver burden at baseline are described in Table 2 and Figure 2. Briefly, 0/5 (0%) patients and 2/4 (50%) caregivers met case criteria for anxiety, while 1/5 (20%) patients and 1/4 (25%) caregivers met case criteria for depression. Patients' mean FACT-G physical well-being, emotional well-being, and functional well-being subscale scores were 18.40 (SD = 4.45), 16.00 (SD = 3.46), and 13.60 (SD = 4.28), respectively, each of which is ≤25th percentile FACT-G subscale scores identified in a population-based sample of adult females with cancer. 32
Preliminary acceptability and perceived effectiveness
Of the participants who completed a debriefing interview, all patients (5/5, 100%) and caregivers (3/3, 100%) recommended BOLSTER, were satisfied with the BOLSTER sessions, and agreed BOLSTER helped the patient understand their illness. Four of five (80%) patients and 3/3 (100%) caregivers agreed BOLSTER improved the patient's symptoms and helped the patient cope with their illness, while 4/5 (80%) patients and 2/3 (67%) caregivers agreed BOLSTER helped the patient plan for the future.
Discussion
Guided by the ADAPT-ITT Framework, we modified SNIP's content and delivery characteristics in response to feedback from patients with gynecologic cancer-associated PC and their caregivers. Our experiences highlight the importance of an iterative approach to intervention development for patients living with serious illness.33,34 Field testing BOLSTER allowed us to modify the visit schedule, format, content, and mode of delivery in response to participant feedback. During the first prepilot, we experienced high rates of attrition related to hospice referral. In response to patient feedback and to improve retention, we shortened the intervention from 10 to 4 weeks and expanded our eligibility criteria to include patients experiencing PC across the disease trajectory. With these changes, we achieved our preliminary feasibility benchmark of ≥80% completion of the post-intervention outcome measures during the second prepilot.
Challenges related to recruiting and retaining research participants with serious illness are not uncommon.35–37 Published recommendations include using broad eligibility criteria 10 ; screening the hospital census or clinic schedule daily 37 ; clear messaging 37 ; dedicating personnel to communicate with clinicians 35 ; and flexibility in recruitment, intervention delivery, and data collection.35,37 Each of these strategies proved essential. In the second prepilot, our expanded eligibility criteria led us to recruit a sample of patients who reported better overall HRQoL than patients in the first prepilot. Nevertheless, patients in both prepilots reported baseline physical, emotional, and functional well-being scores at or below the 25th percentile for females with cancer. 32 This finding suggests it is possible to recruit patients with PC who are well enough to complete a longitudinal intervention, but still highly burdened by illness.
The 4-week iteration of BOLSTER proved more acceptable than the 10-week iteration. Participants in the four-week iteration were more satisfied, more likely to recommend BOLSTER, and more likely to report that BOLSTER was effective. In the four-week intervention, nurse visits and educational content were highly tailored to meet the immediate needs of patients and caregivers. Patients who are highly burdened by illness may prefer an efficient and immediately relevant approach to care management.
Our preliminary acceptability data support the use of telehealth visits and electronic symptom reporting in the care of patients with serious illness. Telehealth visits improve HRQoL and survival across chronic conditions,10,38–40 while electronic assessment of patient-reported outcomes improves HRQoL, health care utilization, and survival in outpatients with metastatic cancer.41,42 In future research, we will assess the extent to which BOLSTER improves these outcomes in our target population.
The principal limitation of this study is its small and relatively homogenous sample. Although we engaged stakeholders in the development of BOLSTER, the findings from our field tests may not generalize to other populations or care settings. Additional research is warranted to assess the extent to which BOLSTER is feasible to deliver and acceptable to patients and caregivers from diverse cultural, socioeconomic, and linguistic backgrounds. In addition, participant-reported survey burden during the first prepilot led us to revise our outcome measures and may have contributed to missing data.
Conclusion
BOLSTER is a multicomponent intervention designed to provide tailored information, resources, and support to patients with gynecologic cancer-associated PC and their caregivers. The results from our field tests suggest BOLSTER is feasible to deliver and acceptable to patients and their caregivers. A randomized controlled pilot trial to assess the feasibility of conducting a full-scale efficacy trial is underway.
Authors' Contributions
The authors affirm that they have each met criteria for authorship as defined by the International Committee of Medical Journal Editors.
Funding Information
This research was funded by a grant from the National Cancer Institute (R21CA223684).
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.