
Abstract
Background:
The Infant Maternal Perinatal Advanced Care Team program was launched in 2018 to enhance perinatal palliative care services in Toronto, Canada.
Methods:
Pilot patients were (1) carrying a fetus with a life-limiting diagnosis and (2) receiving care at the high-risk fetal center. Individualized care included opportunities for establishing goals, labor/delivery planning, grief support, and pediatric palliative care support.
Results:
A total of 107 patients were included during the two-year clinical pilot program. Of those who continued their pregnancy, 45% had care goals focused on comfort while 55% had goals focused on life prolongation. A significant proportion in both groups experienced a fetal or neonatal death. For babies who received comfort-focused care, one-third were transferred to hospice or home.
Conclusions:
A comprehensive perinatal palliative care pathway ensures that more families receive options of pre- and postnatal palliative care supports in varied circumstances where there is significant risk of fetal and neonatal mortality.
Introduction
As innovations in perinatal care allow for earlier diagnosis of fetal anomalies, interventions in utero, and improved intensive care postnatally,1,2 the care of families experiencing a life-threatening fetal diagnosis is increasingly complex. Despite promising interventions, fetuses with anomalies at the most severe end of the spectrum still have a significant risk of serious morbidity or mortality. 3 Perinatal palliative care has emerged as an approach to care that adds extra support for families facing these difficult circumstances.
The American College of Obstetricians and Gynecologists (ACOG) defines perinatal palliative care as a strategy that “comprises options for obstetric and newborn care that include a focus on maximizing quality of life and comfort for newborns with a variety of conditions considered to be life-limiting in early infancy”. 4 They acknowledge that this type of care has merit whether the plan of care is one that focuses exclusively on comfort or incorporates interventions aimed at life prolongation. 4
Government funding supported the creation of a perinatal palliative care pilot initiative in Toronto in 2018. Leaders in perinatology and pediatric palliative care came together to create a partnership among key organizations providing care for fetuses and babies with high-risk conditions: Sinai Health System (high-risk obstetrical/fetal center), the Hospital for Sick Children (tertiary care pediatric hospital), and Emily's House (pediatric hospice).
The objectives were to (1) provide equitable opportunities to support families experiencing a life-threatening fetal diagnosis regardless of their care choices, (2) optimize clinicians' and families' access to pediatric palliative care expertise, (3) maximize opportunities to explore alternative locations for end-of-life care for babies (e.g., hospice or home), and (4) increase capacity for grief/bereavement support pre- and postnatally.
Methods
Program development
An environmental scan, literature review, and stakeholder interviews formed a picture of the state of care before 2018. Input was sought from a design working group with representation from neonatology, genetics, cardiology, obstetrics, maternal–fetal medicine, palliative and hospice care, community providers, and bereaved parents. After input from the design working group, clinicians with perinatal and palliative care expertise came together to form the pilot clinical team (Table 1).
Infant Maternal Perinatal Advanced Care Team Clinical Role Descriptions
Program implementation
Peer education was a key area of focus across relevant groups at all three organizations to raise awareness about the relevance and availability of services. The Infant Maternal Perinatal Advanced Care Team (IMPACT) began accepting referrals from maternity and pediatric providers in April 2019. IMPACT clinicians (Table 1) were introduced to families taking a layered approach as appropriate (Fig. 1). Initial contact was made by the clinical nurse specialist (CNS) at the high-risk pregnancy center during a routine clinic visit. The program was introduced and discussions around goals of care were initiated.
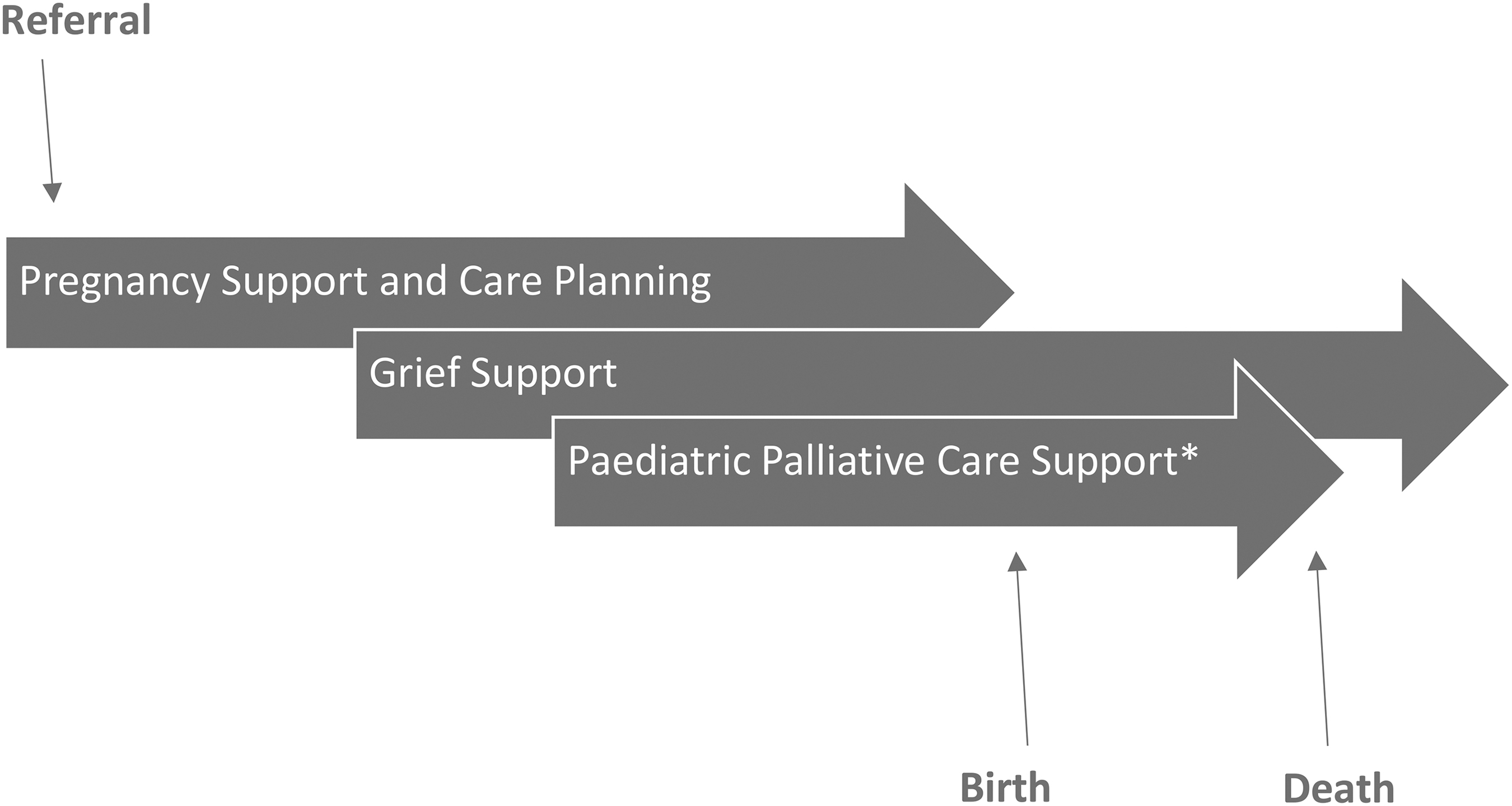
IMPACT care pathway.
Over subsequent visits, a written labor and delivery care plan was cocreated by the CNS and patient, including the wishes of parents with respect to honoring the life of their baby (e.g., memory making/bonding activities, spiritual care interventions) as well as medical intervention aligning with the individualized goals of care. Where the focus of care was not solely on comfort, palliative care plans were incorporated into the broader medical recommendations from other consulting pediatric providers.
Introduction to the IMPACT Grief Support Coordinator was made by the CNS who obtained verbal consent for their involvement after the initial meeting. Grief support included options for phone or video visits. A legacy creation kit was provided to assist families with storytelling activities during the pregnancy and delivery (Table 2). Grief support occurred throughout pregnancy/after birth and continued after pregnancy or infant loss for up to one year (or longer if the family reached back out for support).
Legacy Creation Kit Contents
One of each item/set provided; some intended to be used for more than one activity.
Consultation with a pediatric palliative care NP or MD was recommended for patients whose pregnancies progressed to the third trimester. Discussions were centered around reviewing goals of care and discussing after-birth care including the role of the pediatric palliative care team in different settings, including hospital, home, and hospice, as appropriate.
IMPACT was notified at the time of a patient's labor/delivery with individualized care provided as outlined in the patient's care plan. Pediatric palliative care support was available to assist with pain and symptom management or discharge planning as needed. For babies transferred to an intensive care environment, follow-up was handed over to the broader pediatric palliative care team.
Results
Before 2019, approximately —five to seven patients received prenatal palliative care consultation in Toronto annually. During our pilot program (April 2019–March 2021), a total of 107 patients were followed by IMPACT. The distribution of fetal diagnoses by category is shown in Figure 2. Diagnoses within these categories were at the severe end of the spectrum with appropriateness for referral determined by the fetal medical providers who were providing counseling to families as per their usual standard of care. In total, 107 families were followed in the program with the outcomes for each group shown in Figure 3.
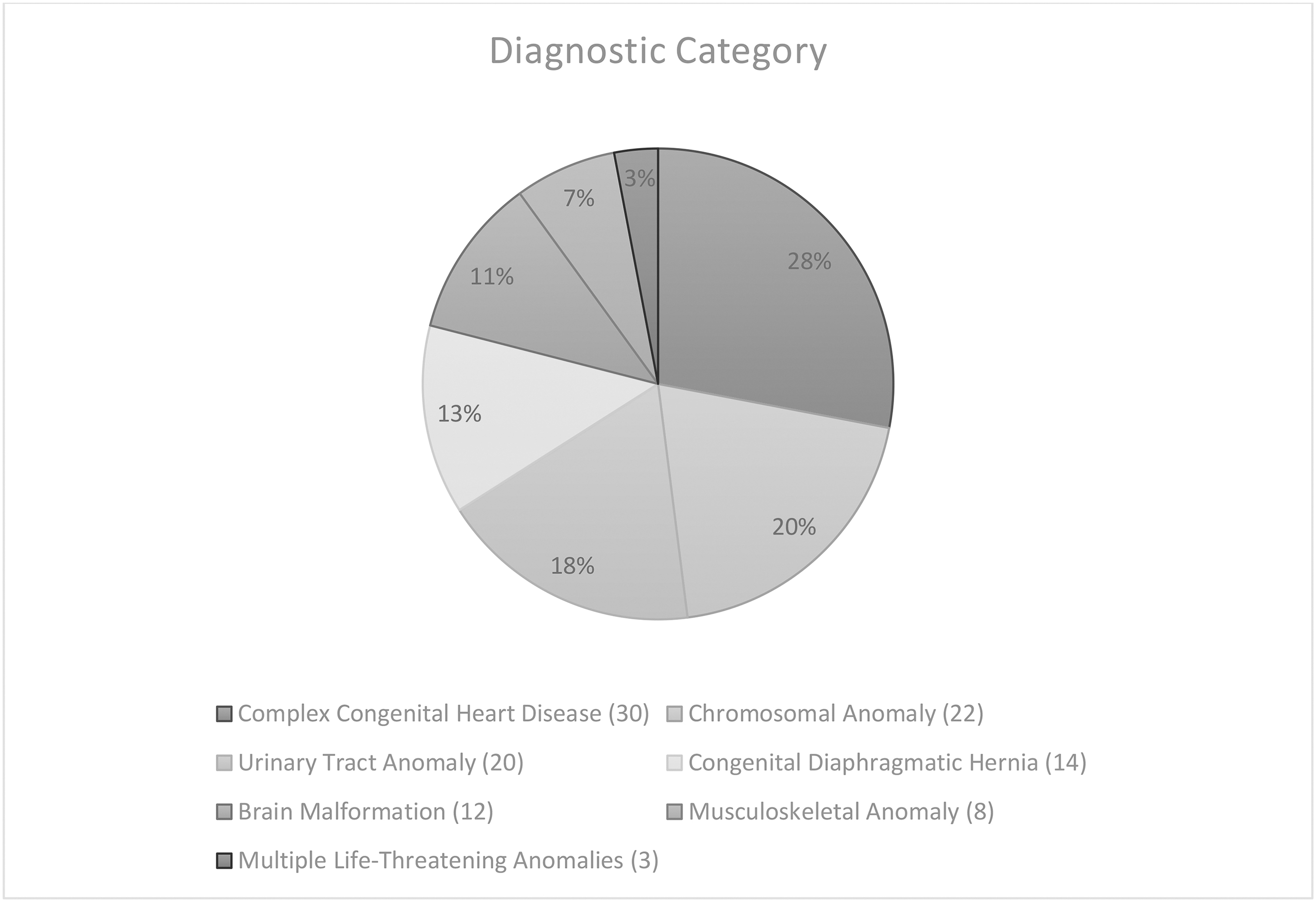
Pilot referrals by fetal diagnostic category. Number of cases are shown in parentheses.
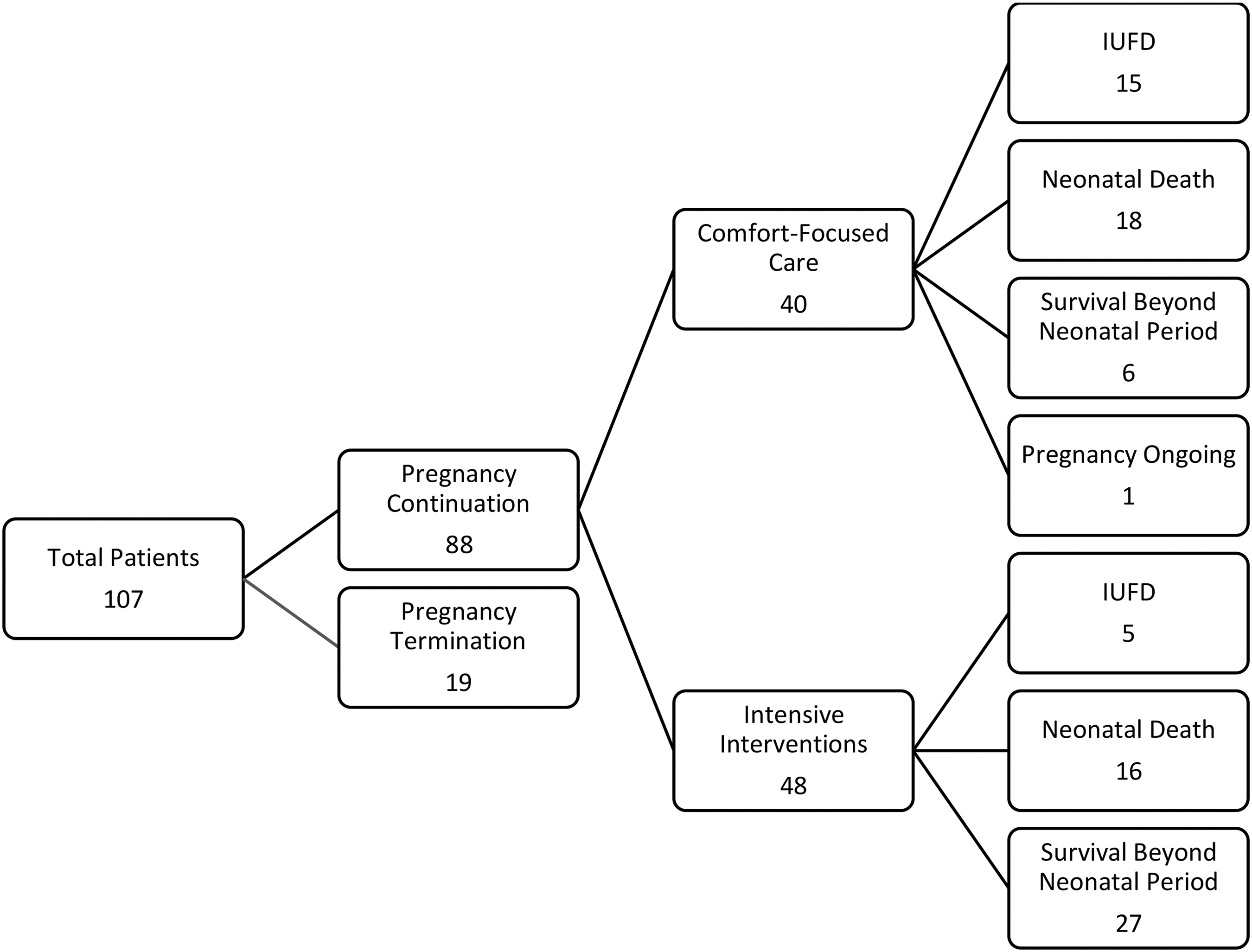
Pilot patient outcomes.
Of the 24 families who delivered a live-born infant with goals of care focused on comfort, 16 babies died in the delivery hospital within 24 hours of life; 5 were transferred home with ongoing community palliative care; and 3 were transferred to Emily's House. All 8 of the babies receiving comfort care who survived long enough (beyond 24 hours) for hospital discharge were transferred to the parents' preferred location. Six of these babies survived beyond the first month of life; depending on needs and updated goals of care, they received ongoing community palliative care support and/or general and subspecialty pediatric follow-up as appropriate.
Discussion
During the 2-year clinical phase of the pilot program, there was a 10-fold increase in referrals for palliative care support compared with the estimated annual referrals before 2018. We hypothesize that the increase was related to three main factors: (1) greater visibility and education about the program, (2) inclusion of all diagnoses where comfort care at birth was considered one ethically reasonable option by the referring experts, and (3) inclusion of families whose goals of care included life-prolonging interventions and intensive care.
We feel that our inclusive approach acknowledges the uncertain and dynamic nature of fetal development and evolving medical and surgical care options and ensures that all families in those circumstances can benefit from concurrent palliative care. In line with that philosophy, the name “IMPACT” evolved over the early months of the pilot program, as clinicians found that the terminology “perinatal palliative care/hospice” was a barrier to referral, particularly when goals of care were intervention focused.
Although there was an overall increase in referrals during the pilot program, relatively few referrals were received for patients opting for early termination. One potential reason for this is that these families likely had fewer clinic or hospital encounters. There may also be a perception of a lack of need for palliative care supports given the existing available social work support acutely at the time of pregnancy termination. We have since advocated more strongly for the potential benefits of IMPACT involvement for longitudinal grief support in these cases given existing evidence that termination in the context of a fetal anomaly may lead to a complicated grief process. 5
Anecdotally, families appreciated the opportunity to engage in legacy creation and storytelling throughout the pregnancy. Owing to visitor restrictions related to the COVID-19 pandemic, we developed small take-home kits containing items to facilitate legacy creation. Through provision of materials and instructions as well as psychoeducation around the benefits of legacy creation, patients were able to work on activities at home so that they could include their partners, other children, and extended family members as desired.
Due to the cross-institutional nature of our program as well as the COVID-19 pandemic, a gradual shift toward more virtual care occurred during the pilot program. Initial consultation and follow-up visits by the IMPACT CNS were almost exclusively done in person during the patient's obstetrical clinic appointments. Partners or other support people, who were not allowed to accompany patients to clinic due to pandemic restrictions, could be included virtually as desired. Grief support and pediatric palliative care consultation were provided virtually a majority of the time.
Although virtual care has its drawbacks, including effects on the clinician–patient relationship and privacy, 6 it also had notable benefits for this program, including efficiency of scheduling for providers from different institutions and the ability for patients to include partners/support people in discussions.
The majority of babies receiving comfort-focused end-of-life care died in hospital in the first 24 hours before mothers were routinely discharged after a birth. For the babies who survived longer than 24 hours and discharged home, community palliative care supports were arranged to ensure a smooth transition in symptom management support. Residential hospice care was offered both for end of life or for transition home depending on prognosis and family wishes.
Going forward, program evaluation will be important from the perspective of both providers and patients. We hope to study the impact of perinatal palliative care supports for families whose goals of care are aimed toward life-prolonging interventions, as this population has not traditionally been served by many perinatal palliative care/hospice programs.
Conclusions
Standardizing perinatal palliative care offerings for families facing a life-threatening fetal diagnosis has allowed significantly more families in our region to access palliative care supports. The high fetal and neonatal mortality rate for this population—irrespective of primarily comfort or intervention-focused care goals—highlights the importance of an inclusive approach.
Footnotes
Acknowledgments
We thank Carolyn Wilson, RN, for her previous role as Grief Support Coordinator during the early development of this pilot program. We also thank the many families and health care providers from Sinai Health System, Emily's House, and the Hospital for Sick Children who have partnered with us to provide this care.
Authors' Contributions
All authors contributed to the content development, writing, and revision of this article.
Funding Information
The Government of Ontario, Ministry of Health and Long-Term Care, provides funding support for the IMPACT program.
Author Disclosure Statement
No competing financial interests exist.