
Abstract
Purpose:
Primary palliative care (PPC) interventions are needed to address unmet symptom needs within standard oncology care. We designed an oncology nurse-led PPC intervention using shared care planning to facilitate patient engagement. This analysis examines the prevalence and severity of symptoms reported by patients and how symptoms were addressed on shared care plans (SCPs).
Methods:
Secondary analysis of a cluster randomized PPC intervention trial. Adult patients with metastatic solid tumors whose oncologist “would not be surprised if the patient died within a year” were included. Twenty-three oncology nurses received PPC training and conducted up to three monthly visits with patients. Symptom prevalence and severity were assessed before each visit using the Edmonton Symptom Assessment Scale (ESAS). Nurses collaboratively developed treatment strategies with patients, targeting the most bothersome symptoms for improvement.
Results:
Among 571 nurse-led PPC visits with 235 patients, the most prevalent and severe symptoms were tiredness (reported at 86% of visits; ESAS ≥4 in 55% of visits), low sense of wellbeing (78%; ESAS ≥4 in 38%), and poor appetite (69%; ESAS ≥4 in 42%). Moderately severe symptoms were addressed on SCPs ranging from 4% (drowsiness) to 35% (tiredness) of the time. Symptom management plans developed by PPC-trained oncology nurses primarily focused on nonpharmaceutical interventions (70%) compared with pharmaceutical interventions (30%).
Conclusion:
The symptoms that patients report most frequently and as most severe on SCPs were addressed less frequently than expected. Further research is needed to understand how PPC interventions can be designed to more effectively target and improve bothersome symptoms for patients with advanced cancer.
Clinical Trial Registration:
ClinicalTrials.gov identifier: NCT02712229
Introduction
The addition of specialty palliative care to standard oncology care improves quality of life and symptom burden for patients with advanced cancer.1–4 Despite these demonstrated benefits, it is not feasible for every patient with serious illness to receive specialty palliative care due to specialist workforce shortages. 5 Primary palliative care (PPC), or the provision of palliative care by nonspecialists, is a potential alternative.6,7 However, PPC interventions must be effectively designed to address key domains of quality palliative care. 8 A recent analysis found that PPC interventions were less likely than specialty palliative care interventions to address physical needs and did not demonstrate an impact on symptom burden. 9 An enhanced understanding as to how PPC approaches address unmet symptom needs is necessary so that future PPC trials can effectively target and improve symptom burden.
The Care Management by Oncology Nurses (CONNECT) intervention trained and supported existing oncology infusion room nurses at community cancer centers to provide PPC along with standard oncology care. Symptom assessment and management was a key component of this PPC approach. 10 To maximize patient involvement, infusion room nurses completed shared care plans (SCPs) with patients to identify and target patients' most bothersome symptoms during intervention visits. In a recently completed cluster randomized trial, the CONNECT intervention did not significantly improve overall symptom burden at three months when compared with standard oncology care, although there was evidence of a dose effect, with patients who received the full intervention experiencing greater symptom improvements. 11
In this analysis, we sought to report the prevalence and severity of symptoms experienced by patients with advanced cancer during PPC visits, describe the frequency with which symptoms were addressed by oncology infusion room nurses using SCPs, and categorize strategies used to manage these symptoms. For this study, we used a dataset of 571 PPC visits conducted with patients with advanced cancer from the CONNECT trial. 11 This analysis provides a detailed description of symptom burden in a large cohort of patients with advanced cancer. In addition, we describe the strategies utilized by PPC nurses to address common cancer symptoms. We hope that this work will inform future development of PPC interventions aimed at expanding access to palliative care and addressing unmet symptom needs in patients with advanced cancer.
Methods
Overview
This study is a secondary analysis of data collected during the CONNECT trial (ClinicalTrials.gov identifier: NCT02712229). This trial enrolled patients with advanced cancer at 17 community oncology clinics in Western Pennsylvania from July 2016 through February 2020. Full details and results of the study have been published previously. 11 This is the first analysis of CONNECT data to focus on symptom assessment and management.
Participants
Eligible patients were adults (>21 years old) with a diagnosis of metastatic solid tumor and an Eastern Cooperative Oncology Group (ECOG) performance score ≤2 (ambulatory, capable of self-care, and active for ≥50% of the day), 12 who were planning on receiving ongoing care from the cancer clinic participating in CONNECT and for whom their oncologist “would not be surprised” if they died within the next year.11,13 Patients were ineligible if they were unable to read and write, unable to provide consent for treatment, or had a hematologic malignancy. 10 All participating patients provided written informed consent. Patients enrolled in the intervention arm who completed at least one CONNECT visit with a SCP were included in this analysis.
Intervention
CONNECT recruited and trained existing oncology infusion room nurses. Training consisted of an immersive (intensive) three-day instruction on evidence-based palliative care strategies to improve quality of life and symptom burden, with role-playing scenarios to practice newly learned skills. Nurses were taught to develop treatment plans informed by a palliative care symptom management resource guide, as well as discussions with the patient about what had or had not worked for them in the past, their expectations and goals, and their preferences. After training and throughout the intervention, nurses received ongoing support from an experienced nurse project manager. Trained study staff analyzed audiorecordings of intervention visits to ensure intervention fidelity. 11
CONNECT nurses focused on providing four key components of PPC: symptom assessment and management, emotional support, advance care planning, and care coordination. CONNECT nurses met monthly with patients for three months, before, after, or proximal to regularly scheduled oncology visits. When an in-person visit was not possible, nurses conducted the visit through a scheduled phone call. Nurses communicated with participating patients' oncologists after each CONNECT visit to discuss details of the encounter, including patients' view of their illness, symptom severity, and SCPs. This collaboration was particularly important when nurses felt pharmaceutical interventions were most appropriate to address patients' symptom needs.
At the beginning of each visit, patients completed an Edmonton Symptom Assessment Scale (ESAS), a well-validated, easily administered patient-reported symptom scale developed in patients with advanced cancer receiving palliative care.14,15 The ESAS assesses the severity of nine common cancer symptoms (anxiety, appetite, depression, drowsiness, nausea, pain, shortness of breath, tiredness, and wellbeing) on a scale of 0–10, with 10 being the most severe. ESAS scores are categorized as not present (0), mild (1–3), moderate (4–6), and severe (7–10).15,16 A symptom score of ≥4 is generally considered clinically significant.17–19 Patient-reported symptoms not encompassed by established ESAS categories were recorded as “other,” using the same severity scale.
During their visit, nurses reviewed the ESAS, elicited the patient's symptom needs, and came to an agreement on which symptom(s) to target and address on the SCP. Although ESAS data informed this process, patients were encouraged to identify their most bothersome symptom regardless of reported severity. SCPs were based on collaborative care models for managing chronic illness across various primary care settings (Supplementary Appendix SA1).20,21 Nurses completed SCPs with patients during each intervention visit. SCPs facilitated patient engagement in discussions regarding symptom burden and promoted effective self-management strategies. Nurses recorded ESAS symptom severity for the most bothersome symptom(s) and corresponding treatment plans on the SCP. At the end of the visits, nurses provided a copy of the SCP to the patient and kept the original to be discussed with the patient's oncologist and referenced at subsequent CONNECT visits. SCPs guided longitudinal discussions of symptom burden and management across CONNECT visits. Additionally, nurses conducted follow-up telephone calls with patients to identify treatment adjustments.
All enrolled patients completed demographic questionnaires at study enrollment, including age, sex, race, time since diagnosis, and cancer type.10,11
Analysis
ESAS scores are presented as a continuous variable (mean ± standard deviation) for each intervention visit and overall, across all three intervention visits. Symptom prevalence was determined by considering a symptom “present” when its ESAS score was score ≥1 and “moderately severe or greater” when the ESAS score was ≥4.
Symptoms were considered “addressed” if they appeared on the patient's SCP for that visit. To establish uniform data abstraction parameters, two study staff members independently reviewed each SCP to determine what symptoms were addressed and categorize written treatment plans. If more than one symptom was included on an SCP, all were considered addressed during that visit.
We categorized treatment plans as pharmaceutical or nonpharmaceutical and reported frequencies (percentages) for these categories. Pharmaceutical treatment plans included new prescription or over-the-counter medications and medication dosage or frequency changes. Nonpharmaceutical treatment plans included suggested behavior modification, psychosocial change, dietary change, referral to additional health care provider, and homeopathic remedies. If a treatment plan did not fit clearly into one of the decided categories, it was categorized as both (e.g., referral to a specialist provider for a medication adjustment). If addressed symptoms had multiple treatment plans, each plan was categorized individually. When adjustments were made to treatment plans from a previous visit that symptom was considered addressed again during the subsequent visit.
Results
Among 336 intervention arm patients enrolled across 17 oncology practices, 80 patients died during the intervention and 40 were lost to follow-up. Two hundred thirty-five completed at least one CONNECT visit with a SCP and were included in this analysis. The patients included in this analysis had a mean age of 68.4 (standard deviation 9.9) years, were near evenly split by gender (53% female), and were mostly Caucasian (>94%) and non-Hispanic (99%). The most common cancers that were treated included lung (40%), gastrointestinal (28%), genitourinary (16%), and breast (12%) (Table 1).
Characteristics of 235 Patients with Advanced Cancer Enrolled in a Primary Palliative Care Intervention
ECOG, Eastern Cooperative Oncology Group; GI, gastrointestinal; GI cancers, esophageal, colon, rectal, gallbladder, gastric, liver, pancreatic; GU, genitourinary; GU cancers, bladder, endometrial, ovarian, prostate, urethral; SD, standard deviation.
Twenty-three CONNECT nurses conducted a total of 571 PPC visits for these 235 patients. Telephone visits comprised 12.5% of total intervention visits. ESAS symptom scores were mostly mild (≤4) and remained relatively stable across the three CONNECT visit time points (Table 2). The five ESAS symptoms with the overall highest mean severity included tiredness (4.2 ± 2.9), poor appetite (3.1 ± 2.9), low sense of wellbeing (2.9 ± 2.4), drowsiness (2.6 ± 2.8), and pain (2.1 ± 2.6) (Table 2). Nausea was associated with the overall lowest mean severity (0.8 ± 1.8).
Edmonton Symptom Assessment Score Severity Reported by Patients with Advanced Cancer at Consecutive Primary Palliative Care Visits
All values are presented as mean ± SD.
ESAS, Edmonton Symptom Assessment Scale; SOB, shortness of breath.
The most commonly reported symptoms were tiredness (reported at 86% of all visits), low sense of wellbeing (78%), and poor appetite (69%) (Fig. 1). The least commonly reported symptoms included anxiety (reported at 47% of all visits), depression (45%), and nausea (24%). The symptoms most commonly reported as moderate to severe (ESAS ≥4) were tiredness (55% of visits), poor appetite (42%), and low sense of wellbeing (38%) (Fig. 1). The symptoms addressed most frequently on SCPs were tiredness (addressed at 35% of visits), poor appetite (20%), and pain (16%). Low sense of wellbeing, drowsiness, and nausea were all addressed infrequently (≤6% of the time). Depression and anxiety were addressed in a similar trend, reported as moderately severe at 20% yet addressed at 6% of visits. When reported as moderately severe, the symptoms addressed most frequently were tiredness (63.3% of the time), followed by pain (63%) and nausea (54.7%). When moderately severe, low sense of wellbeing was only addressed 13.8% of the time, and drowsiness 11.7% (Supplementary Appendix SA1).
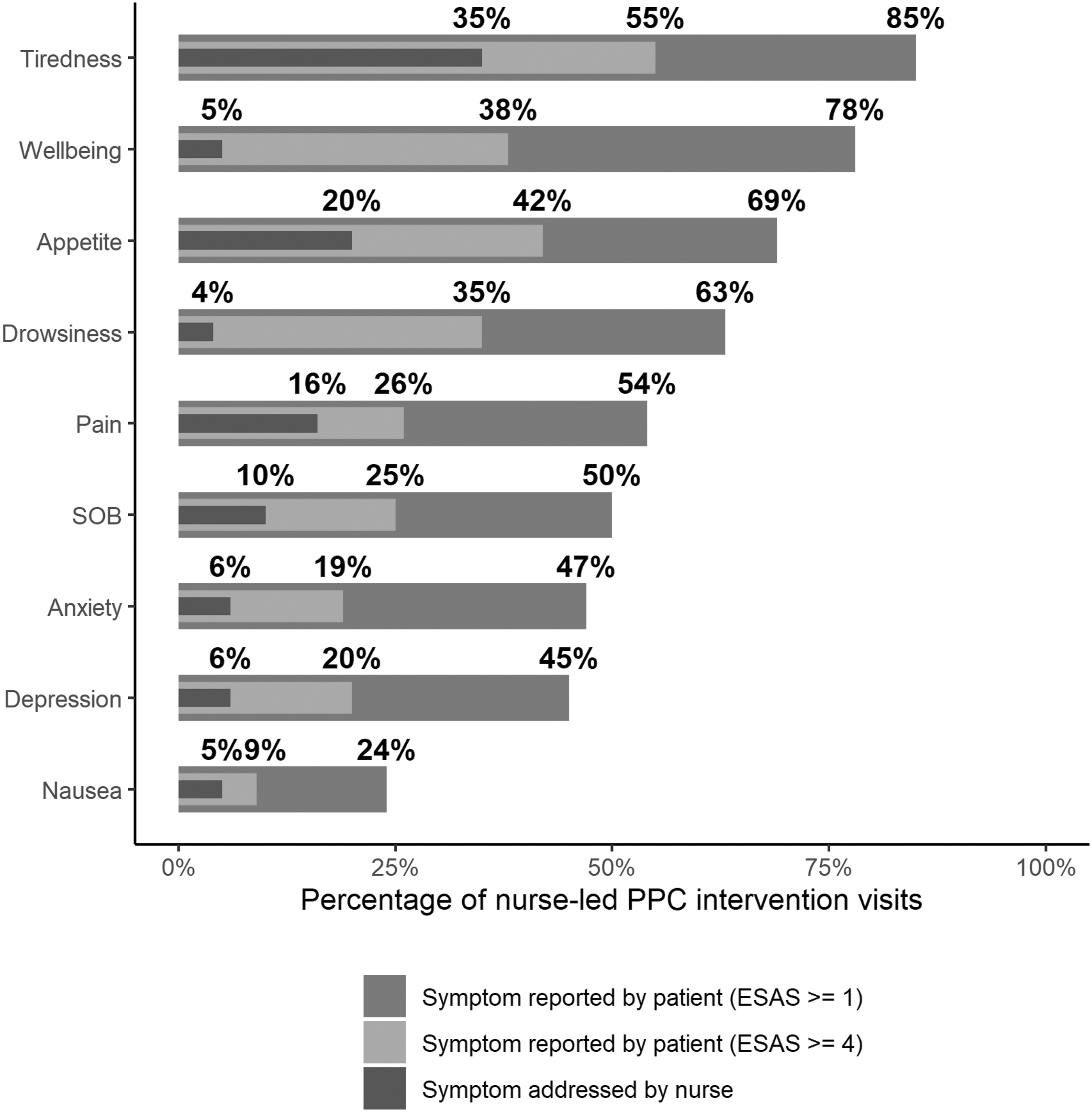
Percentage of PPC visits (n = 571), in which ESAS symptoms reported by patients with advance cancer and addressed by nurses. ESAS, Edmonton Symptom Assessment Scale; PPC, primary palliative care; SOB, shortness of breath.
Treatment strategies used to address individual symptoms are shown in Table 3. Poor sense of wellbeing, poor appetite, drowsiness, and tiredness were addressed with nonpharmaceutical interventions in >80% of PPC visits. Nausea and pain were predominantly managed with pharmaceutical treatment plans. Inclusion of a pharmaceutical intervention on a treatment plan was less common overall compared with inclusion of nonpharmaceutical interventions (Table 3).
Treatment Strategies Employed by Oncology Nurses to Address Symptoms during N = 571 Primary Palliative Care Visits
Total >571 because >1 symptom addressed at some visits.
Discussion
In this secondary analysis of an oncology nurse-led PPC intervention, we identified the frequency and severity of symptoms reported by patients with advanced cancer and assessed the frequency and manner with which these symptoms were addressed on SCPs. While palliative care is often thought of as primarily addressing pain in advanced cancer, we observed that the most commonly reported ESAS symptoms were tiredness, low sense of wellbeing, and poor appetite. These symptoms were also ranked as the most severe. The most common and severe symptoms were addressed infrequently on SCPs, however, at just over half of visits in which they were present. Particularly, low sense of wellbeing was commonly reported as moderately severe, yet infrequently addressed. Nurses predominantly facilitated nonpharmaceutical interventions to address patients' reported symptoms.
Our reported prevalence and average severity of ESAS symptoms is similar to previous investigations of patients with advanced cancer in palliative care settings.18,22,23 Tiredness (fatigue) is consistently reported to be highly prevalent in patients with advanced cancer.23–25 In addition, our finding of average ESAS symptom severity as low to moderate is consistent with previous work. 26 A knowledge of which symptoms are reported most frequently by patients with advanced cancer is key in designing interventions to improve symptom burden. Our findings add to the growing body of literature demonstrating that certain symptoms with low-to-moderate severity remain highly prevalent in patients with advanced cancer and are associated with poorer quality of life.27–30
Symptoms that patients ranked as moderately severe on the ESAS were frequently not addressed on SCPs. This was particularly true for low sense of wellbeing, drowsiness, and depression. There are several potential explanations for this finding. The ESAS symptoms, patients rank as most severe, may not be the symptom they brought up to their oncology nurses when completing SCPs. For instance, if patients perceive their oncology team is not positioned to handle their depression or low sense of wellbeing, they may not have identified it when prompted. Conversely, patients may have existing social or community resources they feel are sufficient in managing their psychological symptoms. Some patients may also fear that discussing specific symptoms with their oncology team will impact their ongoing cancer treatment. Previous work has demonstrated that although patients with cancer may perceive issues as important (e.g., advance care planning), they may be unwilling to raise those issues to their providers. 31 Furthermore, sociocultural norms and the stigma surrounding mental health and its treatment may account for the reluctance of some patients to choose psychological symptoms to be addressed.
Additionally, this finding may suggest that participating oncology nurses felt better equipped to address physical symptoms than psychological symptoms. In surveys conducted during CONNECT trainings, nurses identified “addressing emotional needs” and “overcoming fear of discussing end-of-life issues” as specific goals to improve upon during the intervention. 32 A separate focus group study found that oncology nurses report “patients' lack of emotional disclosure” and “maintaining emotional boundaries” among factors impacting the provision of psychosocial care. 33 A qualitative interview study with CONNECT nurses found that although nurses reported fulfillment and satisfaction associated with developing deeper emotional relationships with patients, they endorsed guilt associated with doing less treatment-oriented tasks than their colleagues. 34 Although CONNECT trainings provided nurses with evidence-based skills for symptom management, participating nurses may have felt they had inadequate time, support, or tools to address and manage specific psychological symptoms.
Moreover, while relatively rigorous for a PPC intervention, nurses received far less communication training than palliative care specialty clinicians. Lastly, physical symptoms may have been more straightforward for nurses to discuss with oncologists, leading to prioritization.
We found that the majority of treatments facilitated by oncology nurses to address ESAS symptoms were nonpharmaceutical. This finding may in part be due to the intervention being led by nonprescribing clinicians. While the oncology nurses were asked to follow up with oncologists to discuss treatment plans and needed prescription, they may have prioritized nonpharmaceutical approaches that could be offered without oncologist involvement, for example, behavior, psychosocial, dietary, or homeopathic recommendations. However, it is also the case that we have effective pharmaceutical interventions for certain symptoms (e.g., nausea and pain), but limited pharmaceutical options that are effective in managing the symptoms most frequently endorsed by patients with advanced cancer (e.g., tiredness, low sense of wellbeing, and poor appetite).
Implications and next steps
Our findings suggest that nurse-led PPC interventions may benefit from additional resources and support for oncology nurses to target and manage symptom burden in patients with advanced cancer. Future nurse-led PPC interventions should be designed with input and continual feedback from nurses, to ensure they have the training, skills and resources they need to target and manage patients' most burdensome symptoms. Interventions led by nonprescribing clinicians should be designed to ensure and streamline treatment collaboration with prescribers. Additional consideration should be made for assessing and improving patients' overall wellbeing. Normalizing discussion of psychological symptoms across members of the oncology team may allow patients to feel comfortable broaching these concerns.
Limitations
This secondary analysis has several limitations. Our results are exploratory in nature and intended to be hypothesis generating. Although the ESAS was administered at each visit, we were unable to identify symptoms that may have been discussed and addressed during visits but not included on SCPs. Similarly, variation in the level of detail recorded on SCPs may have impacted our analysis. We also do not know the extent to which SCPs truly addressed symptoms that were most bothersome to patients. Lastly, our sample population is mostly Caucasian, non-Hispanic, and from Western Pennsylvania, which limits overall generalizability.
Conclusion
In conclusion, we found the symptoms that a population of patients with advanced cancer rank as most severe on an ESAS are not always the symptoms addressed by primary palliative care-trained nurses in SCPs. Further research is needed to understand how PPC interventions can be designed to effectively target and improve symptom burden in patients with advanced cancer.
Footnotes
Acknowledgments
The authors would like to thank all CONNECT nurses who worked diligently and selflessly to make the CONNECT trial possible and the patients who agreed to be part of this study.
Authors' Contributions
C.J.M.: conceptualization, investigation, qualitative data—coding and analysis, figure design—review and editing, formal analysis, methodology, project administration, writing—original draft, and writing—review and editing. A.A.: data curation, methodology, formal analysis, figure design—review and editing, and supervision. R.F.: data curation, methodology, formal analysis, and original figure design—review and editing. R.M.A.: conceptualization, resources, investigation, and writing—review and editing. M.R.: conceptualization, investigation, and writing—review and editing. K.S.: conceptualization, investigation, and writing—review and editing. E.C.: conceptualization, investigation, and writing—review and editing. D.W.: conceptualization, investigation, and writing—review and editing. T.S.: conceptualization, investigation, and writing—review and editing. Y.S.: conceptualization, methodology, project administration, investigation, resources, supervision, writing—original draft, and writing—review and editing.
Ethics Approval
The CONNECT study was approved by the University of Pittsburgh Research Subjects Review Board (STUDY19090204).
Consent to Participate
Informed consent was obtained from all individual participants in the study.
Consent for Publication
Y.S. authorized and oversaw use of data from the CONNECT trial for this secondary analysis.
Funding Information
The CONNECT trial was supported by R01CA197103 from the National Cancer Institute (principal investigator: Y.S.) and in part by K24AG070285 from the National Institute on Aging (recipient: Y.S.). This project used UPMC Hillman Cancer Center clinical facilities that are supported in part by NCI P30CA047904.
Author Disclosure Statement
R.M.A., Y.S., and D.W. are contributors to UpToDate. The authors report no other conflicts of interest in this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.