
Abstract
Background:
The determination of what makes a medical treatment inappropriate is unclear with a small likelihood of consensus.
Objectives:
This study aimed to explore how clinicians in cardiology perceive “inappropriate treatment” and to collate the common profiles of cardiology patients receiving likely “inappropriate treatment” as perceived by clinicians in a multiethnic Asian context.
Methods:
A qualitative study was conducted using semistructured in-depth interviews with 32 clinicians involved in the care for cardiology patients at a large national cardiology center in Singapore.
Results:
Clinicians' accounts indicated that elements of potentially inappropriate treatment encompass patient-related treatment elements as well as quantitative and probability-based elements such as resource use and probability of treatment benefit. Patient prognostic profiles, characterized as likely to have received inappropriate treatment by clinicians, were organized into six categories according to demographic, clinical, and functional factors.
Conclusions:
The perception of inappropriateness of treatments among clinicians in cardiology was primarily focused on patient-related outcomes. Collated patient profiles may serve as meaningful indicators of patient cases receiving potentially inappropriate treatment for further research and intervention.
Introduction
With rising health care costs at the end of life, concerns of inappropriate or futile treatment have grown in the past decade.1,2 A policy statement from the Society of Critical Care Medicine emphasizes that “futile interventions” pertain to interventions that are unable to accomplish the intended physiologic goal for the patient. 3 On the contrary, potentially inappropriate treatment tends to be nebulous and challenging to define,1,4 as it generally varies from a case-to-case basis. 3 In this study, potentially inappropriate treatment is conceptualized as an intervention that does not provide a reasonable expectation for survival outside the acute care setting with sufficient cognitive ability to perceive the benefits of treatment. 3
In the cardiology setting, previous studies have found that clinicians have a more curative or proactive mindset in treating patients at the end-of-life, which may lead to potentially inappropriate treatment.5,6 However, the fundamental question as to how cardiology clinicians perceive what makes a treatment potentially inappropriate, as well as elucidation of which cardiology patients tend to receive inappropriate treatment, has not been explored. Furthermore, there has not been a study examining the perceptions of inappropriate treatment among clinicians in cardiology in an Asian setting. This question is particularly pertinent in an Asian clinical setting where more inappropriate treatment is often expected due to strong family involvement in decision-making process.7,8 Therefore, this study aimed to explore the perceptions of clinicians in cardiology on what makes treatment inappropriate and aimed to identify common patient prognostic profiles of those who may have received potentially inappropriate treatment in the cardiology setting.
Materials and Methods
Study design
Clinicians from a large national cardiology center in Singapore were recruited with purposive sampling by gender, subspecialties, and designation. An interview guide was developed based on existing literature9,10 and consultation with a senior cardiologist and a palliative medicine clinician working in a cardiology clinic (Supplementary Appendix SA1). Interviews were conducted in-person in a meeting room at the cardiology center or remotely via phone between December 2019 to June 2020 in English by two research team members (S.Y. and J.L.). Interviews ranged from about 30 to 60 minutes and field notes were taken to note any important features. There were no repeat interviews. Details of the study design were previously published. 8
Data analysis
Interviews were audio recorded and transcribed verbatim for analysis and subsequently imported into NVivo 12 to facilitate qualitative analysis. Data were thematically analyzed through familiarization with the data line by line and repeated sorting, coding, and comparison. 11 Data were coded independently by two research team members (J.L. and S.Y.) trained in qualitative research, and discrepancies were resolved with discussion. Code categories were developed and compared to ensure that they were mutually exclusive. Core categories were elaborated around definitions of “inappropriate treatment” and patient profiles likely to have received “inappropriate treatment,” primarily from the question “Can you please describe a situation in your experience when a person got treatment at the end of life you didn't think they should have had?.” Coded data were subsequently compared with findings from existing literature12,13 to assess commonalities and differences and to conceptually relate one another. Therefore, both inductive and deductive approaches were adopted to refine and develop the themes and subthemes on inappropriateness and patient profiles.
Ethics
This study was approved by the Central Institutional Review Board of SingHealth (CIRB-2019-2887).
Results
A total of 32 clinicians were interviewed, including cardiologists (n = 19), cardiac surgeons (n = 10), and palliative care doctors (n = 3) involved in the care of cardiology patients. Out of the 32 participants, 20 participants (62.5%) were male. In terms of ethnicity, 27 participants were Chinese, 3 were Malay, and 2 were Indian. Most participants were consultants (53.2%), followed by senior consultants (21.9%), associate consultants (18.8%), and registrar or residents (6.4%). Data saturation was achieved at 30 interviews, and 2 interviews were additionally conducted to confirm saturation in emergent themes.
Elements of inappropriateness
Participant accounts indicated two salient categories in terms of elements of inappropriateness: (1) elements inappropriately affecting the patient and (2) elements based on quantitative definition (Supplementary Table S1).
For the former, these included how the treatment burden will affect the patient, and the nature of “hope” influencing treatment decisions. Most participants described inappropriate treatment based on these patient-related treatment outcomes. Treatment burden to patient was commonly discussed along the lines of prolonging the patient's suffering. For example, a participant mentioned:
For me, I define it as prolonging a very aggressive support such as ECMO and you think that there is no chance of recovery, or meaningful recovery after a certain period, or […]meaningful outcome to the patient—#2, cardiologist
This also aligns with giving a sense of false hope as well as not improving or worsening the clinical, symptomatic outcomes of the patients. The patient's potential for or lack of quality of life was also frequently discussed, indicating the importance of this outcome for determining the inappropriateness of a treatment.
For elements based on quantitative definitions, a minority of participants discussed the consideration of resources to characterize treatment to be inappropriate. More participants referred to a probability-based approach, where there is either low or no chance of benefit conferred to the patient. The probability of patient benefit also encompassed probability of positive treatment prospect, with participants often referring to high likelihood of patient suffering as an element of inappropriateness.
Common patient profiles
When asked to provide example situations, in which patients likely received treatment that they should not have, participants primarily referred to six patient profiles (Fig. 1). These included: (1) patients with neurological deficiencies; (2) patients with severe sepsis or infection as well as multiorgan failure; (3) young adult patients with severe cardiomyopathy and succumb to complications; (4) middle-aged or young adult patients with acute myocardial infarction and succumb to complications; (5) incapacitated elderly patients with multiple comorbidities and end-stage heart failure; and (6) very elderly and frail patients. In Figure 1, these profiles are mapped across demographic, clinical, and functional factors, with solid lines indicating commonly reported characteristics for each profile and dashed lines indicating some of the less commonly reported characteristics associated with the profile.
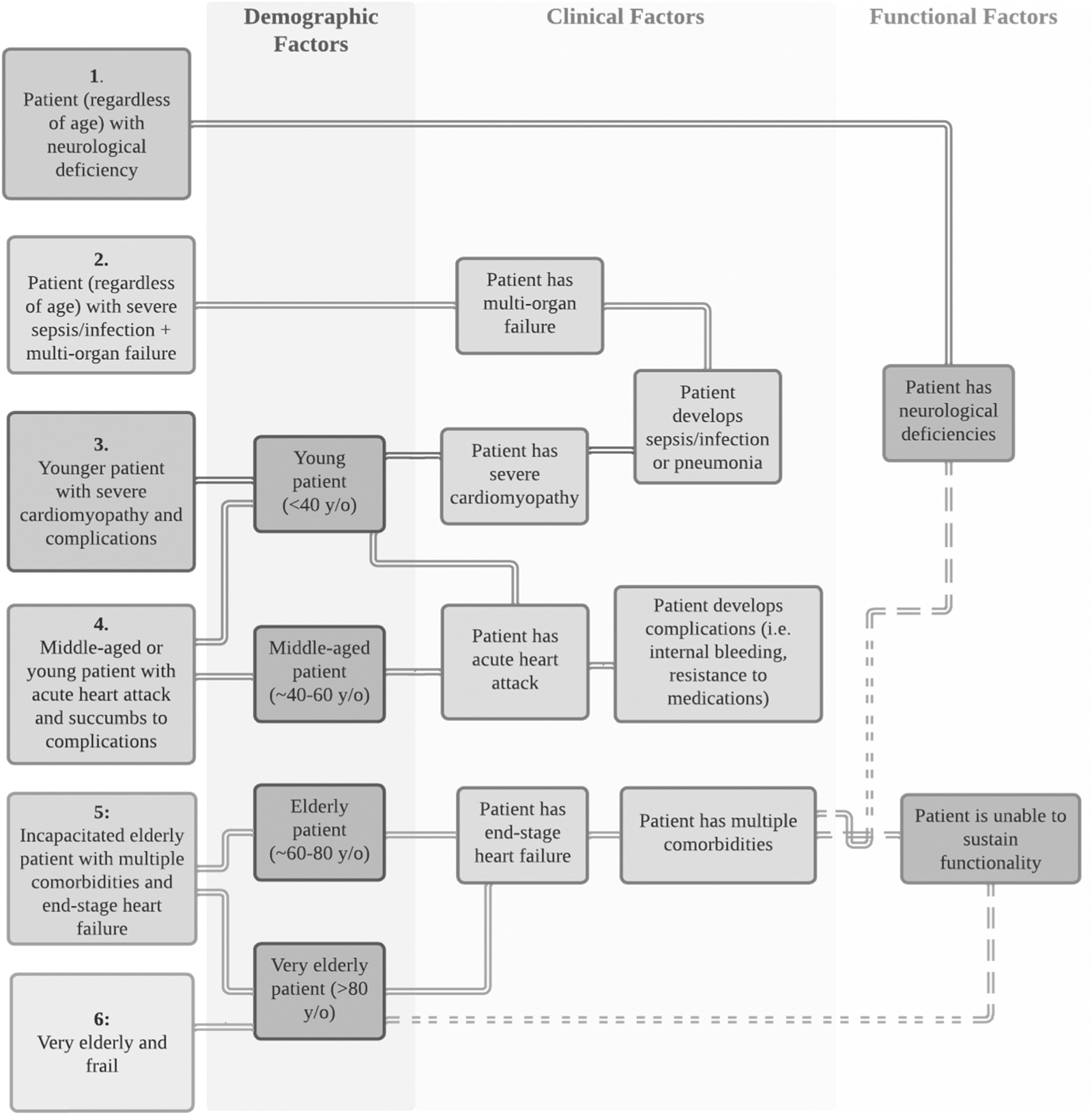
Commonly reported prognostic patient profiles to have likely received futile treatment (n = 32).
The most common profile reported was patients with severe sepsis or infection as well as multiorgan failure, regardless of the age of the patient, followed by very elderly and frail patients. Most participants mentioned that the elderly tend to have difficulty for end-of-life issues, and this may, in part, be due to potential neurological deficiencies or severity of illnesses. A participant stated:
In terms of cardiac patients, those who are nearing end of life are usually pretty identifiable., They are very sick patients and critically ill. And a lot of them, whatever we do, don't really respond to it or some of them are already brain dead at times.—#28, cardiac surgeon
We have also collated the interventions mentioned by participants to have been potentially inappropriate treatments to these patients in these circumstances in Supplementary Table S2.
Discussion
From one of the first studies in Asia to examine the perceptions of clinicians in cardiology of potentially inappropriate treatment, we found that clinicians primarily view inappropriate treatment as a pitfall in patient clinical outcomes, with a minority of clinicians alluding to resource usage and probability-related outcomes to assess inappropriateness. Furthermore, we identified patient prognostic profiles that may have higher likelihood of receiving inappropriate treatment. We emphasize that identifying these profiles is not to promote the undertreatment of these patient groups, but to propose interventions to foster better treatment decision making for these patient groups and their families.
What this study adds
Our findings regarding the elements of inappropriateness align with findings from prior studies in other settings.13–15 Although our findings from cardiology are similar to categories pertaining to medical futility from a previously published systematic review, the elements of inappropriateness in our study did not encompass professional aspects such as societal norms, as we had categorized them as factors that influenced medical futility rather than elements of inappropriateness. 8 Furthermore, unlike prior studies, the present study did not find definition for challenges such as unfamiliarity with or inability to define inappropriate treatment. This may explain the familiarity of the term within the cardiology setting compared to other clinical specialties.
In terms of the common patient profiles, previous studies have retrospectively operationalized inappropriate and futile treatment through medical chart reviews and assessments by health care workers.2,12,16 As opposed to determining discrete clinical markers or outcomes of inappropriate treatments after treatments already occurred, we sought to explore the common prognostic profiles of patients that may have received futile treatment as perceived by practicing cardiology clinicians. The implications of this method would be to prospectively identify a larger, holistic group of patients that match “high-risk” prognostic profiles for the consideration of interventions before the potential provision of inappropriate treatment, such as engaging in earlier end-of-life discussions and planning. These profiles presented in this study serve as a preliminary reference tool and should be refined, operationalized, and empirically tested in future studies.
Strengths and limitations
The current study has several limitations. We recruited participants from a single cardiology center, so generalizability of findings may be limited. However, the center accounts for more than 40% of cardiology patient treatments nationally. Another limitation would be the retrospective nature of the identified patient profiles, as clinicians were not asked to identify potential inappropriate treatment cases. Future studies should examine the possibility and validity of identifying common patient profiles before the administration of inappropriate treatment.
Footnotes
Acknowledgments
The authors thank all the clinicians at National Heart Centre Singapore (NHCS) who took part in this study.
Authors' Contributions
N.G. and S.Y. contributed to the study inception and design. J.L. and S.Y. conducted data collection and analysis. J.L. drafted the article with advice and supervision from S.Y. N.G. provided editorial input. D.S. and S.H.S.N. provided clinical and editorial input. All authors read and approved the final version of the article.
Funding Information
This study was supported by the Lien Centre for Palliative Care Extramural Research Award LCPC-IN19-0001.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.