
Abstract
Background:
Breathlessness is a common symptom for palliative patients that can cause distress and decrease function and quality of life. Palliative care services in Australia aim to routinely assess patients for breathing-related distress, but timely reassessment is not always achieved.
Objective:
To improve the timeliness of breathlessness reassessment in a home-based community palliative care service in New South Wales for people with moderate-to-severe breathing-related distress. Breathing-related distress was defined as a Symptom Assessment Score for “breathing problems” of four or more.
Methods:
This collaborative quality improvement (QI) project between SPHERE Palliative Care CAG, Stanford University mentors, and a Sydney metropolitan specialist palliative care service included a: (1) retrospective chart audit; (2) cause and effect analyses using a fishbone diagram; (3) development and implementation of key drivers and interventions; and (4) a pre-and-post evaluation of the timeliness of reassessment of breathing-related distress and changes in Symptom Assessment Scale scores for “breathing problems.”
Results:
Key interventions included multidisciplinary education sessions to facilitate buy-in, with nurses as case managers responsible for breathlessness reassessment and documentation of scores, access and training in electronic palliative care data entry software, fortnightly monitoring and reporting of breathing-related distress scores, and development of an educational flowchart. The proportion of patients reassessed within seven days of an initial nursing assessment of moderate-to-severe breathing-related distress increased from 34% at baseline to 92% at six months.
Conclusion:
A local QI project increased the proportion of patients with a timely reassessment of their breathing-related distress in a community palliative care service.
Background
Breathlessness is a common symptom in palliative care patients that interferes with functional capacity and quality of life and can be a source of distress. In patients with advanced cancer, the risk of mortality is increased by 80% when breathlessness is present. Worldwide, in 2017, marked suffering or distress from breathlessness was experienced for ∼6.6% of all days spent in palliative care settings before death. 1
Chronic breathlessness is systematically underrecognized and undertreated in palliative care, and the impact of breathlessness on individual patients is poorly understood. 2 A rigorous assessment of breathlessness should include a thorough patient history, examination, and thoughtful investigations to ensure that reversible underlying causes are treated and symptom management is optimized. 3 Early integration of palliative care with respiratory, rehabilitation, and primary care services, with referral based on distress from breathlessness and complexity of symptom management is recommended, rather than prognosis. 4 Models of care need to shift toward the triggering of services or triaging patients based on symptom distress related to refractory breathlessness, and account for short-term admissions earlier in patients' disease trajectory as well as end-of-life care. 4 Addressing distress from breathlessness is particularly important as pharmacological management, while helpful for physiological aspects of breathlessness, cannot address psychosocial issues related to breathlessness nor the cognitive processes that drive breathlessness. 4
In 2005, the Palliative Care Outcomes Collaborative (PCOC) introduced the Symptom Assessment Scale (SAS) to Australian palliative care settings to capture distress from common palliative care symptoms, including breathlessness. 5 Wide implementation of the SAS, other PCOC measures, and national benchmarks have supported individual health services to evaluate clinical outcomes and initiate quality improvement (QI) where required. 5 A SAS score of >8 leads to a severity score of “unstable” and therefore requiring urgent follow-up (Table 1). 6 PCOC has clearly defined responsiveness to urgent needs (i.e., 90% of patients in the unstable palliative care phase 5 having their needs met within three days). People requiring urgent follow-up are identified according to the clinician-rated Palliative Care Problem Severity Score and phase on admission to the service, and are targeted for follow-up within 24 hours as part of usual care. However, there is no specified timeframe to manage moderate distress identified through the SAS. According to the PCOC framework, a patient could remain classified in the “stable” or “deteriorating” phase for some time yet with unaddressed breathing-related distress.
Palliative Care Outcomes Collaboration Phase Definitions 6
Or, in the instance of an expected deterioration, symptoms might be medically addressed, yet the patient may still experience breathing-related distress. 4
The problem of breathing-related distress locally
Recent evidence of significant assessment and response gaps for breathing-related distress was identified in a specialist community palliative care service in metropolitan New South Wales (NSW), Australia. Based on PCOC data between July and December 2020, 98% of patients admitted to the community service experienced breathing problems, yet only 17% received responsive care, well below the national benchmark of 60%. 7 Responsive care refers to the proportion of patients with moderate-to-severe symptoms at the beginning of the phase who have absent or mild symptoms at the end of the phase.8,9 In addition, only 22% of patients with moderate-to-severe breathing-related distress (defined as a PCOC score ≥4) on admission had a repeat SAS documented within seven days. As such, we determined that the service not providing adequate responsive care for patients with breathing-related distress in part stemmed from the low rate of timely reassessment. Our QI project therefore aimed to improve the timeliness of breathlessness assessment in a home-based community palliative care service in NSW.
Objective
Between February and August 2021, our first objective was to increase the proportion of patients with a moderate or severe PCOC SAS score (≥4) for “breathing problems” on admission to community palliative care services who had a repeated PCOC SAS score for “breathing problems” completed by any member of the multidisciplinary team within seven days from 34% to 90%. Other objectives were to assess changes in breathing-related distress scores among those with moderate-to-severe breathing-related distress on admission. As there was no clearly defined timeframe for repeat assessment of patients with moderate breathing-related distress, a target of seven days for reassessment was decided by consensus within the project team and aligned with weekly multidisciplinary team review of individual patients. 9
Methods
Design
This QI project included a retrospective chart audit, cause and effect analyses, development and implementation of key drivers and interventions, and a pre-and-post outcome assessment of scores for “breathing problems” among those identified with moderate-to-severe breathing-related distress. The project is reported according to the Revised Standards for Quality Improvement Reporting Excellence (SQUIRE) Checklist version 2.0. 10
Setting/context
The project was undertaken in one Australian specialist community palliative care service between February and August 2021. The service provides care to ∼250 patients and is predominately a Clinical Nurse Specialist-led service with a strong multidisciplinary team. The proportion of patients who speak a language other than English at home within the local health district is higher than the national average (21%), 11 yet lower than other Sydney metropolitan local health districts (46%–71%).12,13 The project was part of an international collaborative program involving Stanford University, California and the Australian SPHERE Palliative Care Clinical Academic Group. The QI team included a clinical nurse specialist and researcher, physiotherapist, doctor, occupational therapist, nurse practitioner, and palliative care and QI researchers as mentors.
QI process
The project involved a process of monthly one- to two-hour remote mentorship sessions with Stanford University mentors (J.M. and M.D.) through Zoom teleconferencing, didactic instruction, and project-based learning in QI. These mentors guided each online session using an A3 template, based on “Plan-Do-Study-Act” method, which uses a small scale, iterative approach to testing solutions that allows rapid assessment and feedback and the flexibility to adapt to changes that align with the clinical context. 14 An overview of the course structure and process is provided in Table 2.
Stanford University and SPHERE Palliative Care Clinical Academic Group Collaborative Quality Improvement Project Road Map
Cause and effect analysis using a fishbone diagram identified measurement, material, environmental methodological and personnel factors related to the problem (Fig. 1 and Table 3). Weights (%) were assigned to factors considered modifiable within the scope of the project, termed “key drivers.”
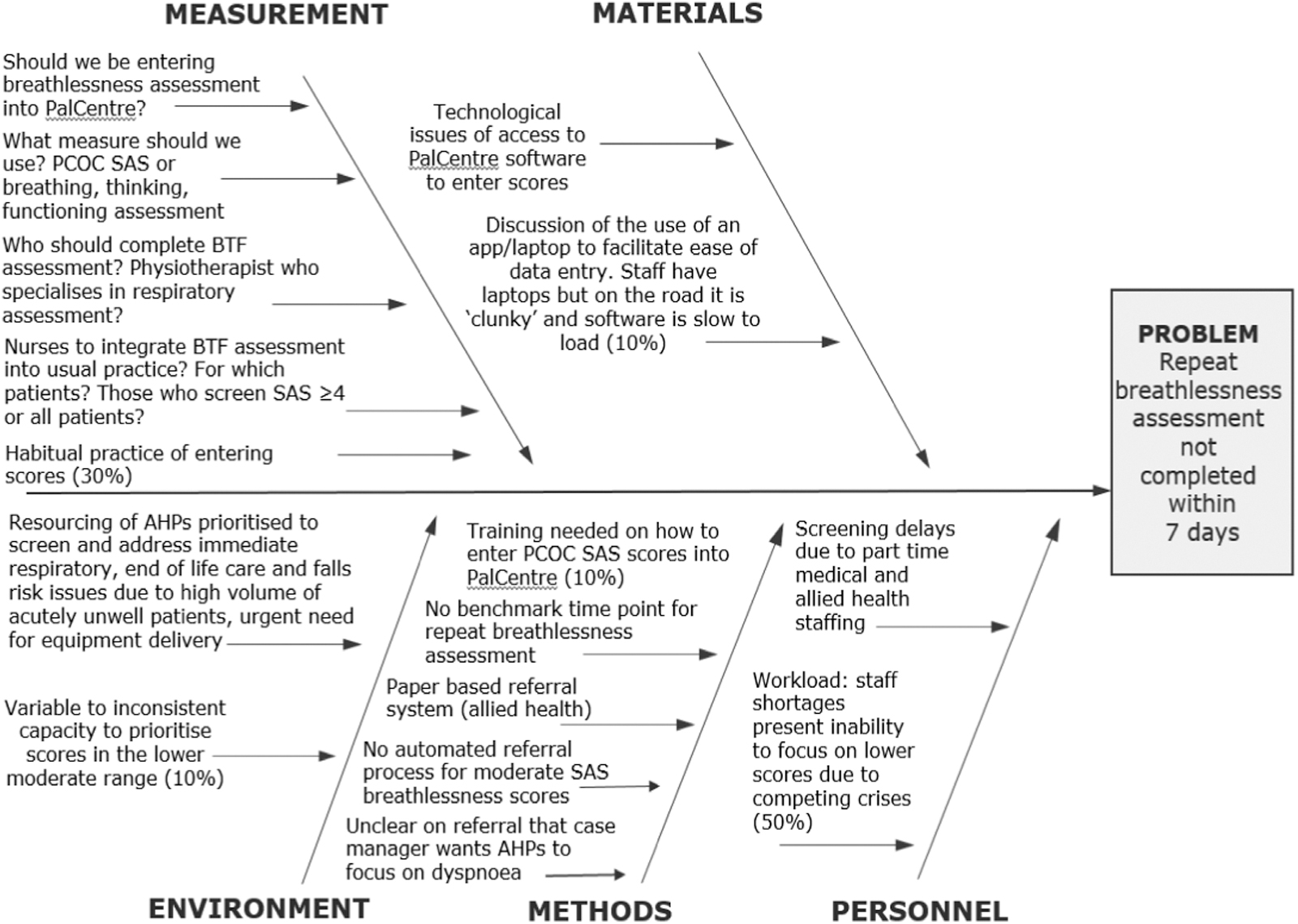
Cause and effect diagram.
Analysis of Root Causes of Delays in Breathlessness ReAssessment Within Seven Days
BTF, Breathing, Thinking, Functioning; PCOC, Palliative Care Outcomes Collaborative.
Interventions were developed by the project team to address these key drivers. The sustainability of each intervention was considered and promoted by designating the method, frequency, and personnel for sustainability activities. Reliability of interventions was categorized as Level 1: Individuals (feedback, checklists, training and basic standards); Level 2: Procedures (embedded standard work, reminders, constraints); or Level 3: Systems (process design, fail safes, physical layout, built in feedback, automated systems, concentration of responsibility). “Maturity bars” denoted progress of each intervention as (0) an untested idea, (1) early tests/Plan, Do, Check, Act; (2) multiple levels; (3) early implementation; and (4) working well in operation. Interventions were also classified as involving a “barrier” or as “abandoned” where relevant.
Measures
Data were collected between September 2020 and August 2021. Data collected at baseline included:
Demographics: diagnoses, date ready for care, episode start date, and hospital admissions and readmissions during the study period (yes/no).
Australian Karnofsky Performance Scale (AKPS) Score. 15
Palliative Care Outcomes Collaboration (PCOC) Phase. 5
Resource Utilization Group Activities of Daily Living (RUG-ADL). 16
PCOC SAS breathing problems subscale8,9 (Fig. 2). The first and second breathing-related distress scores, including the score taken at episode start date, were collected. Use of the PCOC SAS has been widely implemented in Australian palliative care settings due to its ability to identify the distress related to patients' breathlessness rather than the presence of the symptom.
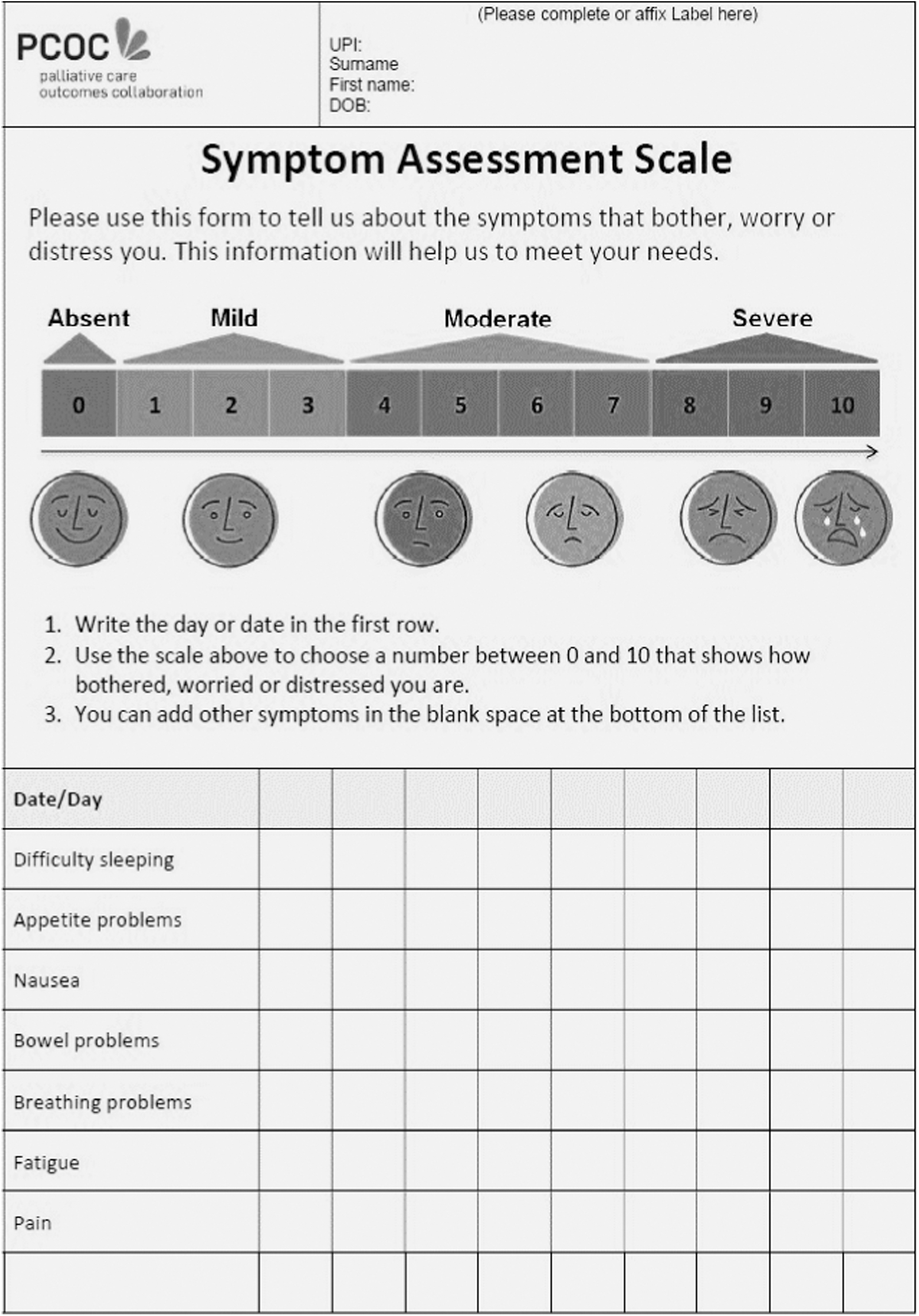
Palliative Care Outcomes Collaboration Symptom Assessment Scale (including ‘Breathing Problems’ subscale). 8
Timeliness of breathlessness assessment: The date of assessment and number of days between the first and second breathing-related distress assessment were collected.
Analysis
Reassessment data for breathing-related distress were reported as a percentage on a line chart in four-week increments over a six-month period. Weekly periods were defined as midnight Sunday evening to 23:59 the following Sunday night. Data were analyzed and reported using descriptive statistics. An additional analysis included a paired sample t-test to detect mean differences in breathing-related distress scores at the second assessment.
Ethical considerations
This project did not meet criteria for an Institutional Review Board review and was approved as a QI initiative from the relevant Local Health District ETH11249.
Results
Retrospective chart audit
At baseline (September 14, 2020–January 11, 2021), the proportion of new patients admitted to home-based community palliative care with a breathing-related distress score ≥4 reassessed within seven days was 34%.
Cause and effect analysis
Root causes included a lack of understanding as to who should be entering SAS scores for breathing problems on PalCentre software, variable to inconsistent capacity to prioritize scores in the lower to moderate range due to competing crises, the need for training on how to enter SAS scores in to PalCentre, and the need to support clinicians' access to PalCentre (Fig. 1 and Table 3).
Development of key drivers
Four key drivers were identified, including:
Nursing and allied health staff to create a habitual practice of entering symptom assessment scores at each assessment. Timely allied health referral for breathing-related distress where applicable to eliminate referral lag. Embodying a preventative mindset that is proactive rather than reactive (for example, by promoting assessment of breathing-related distress before a crisis arises). Consistency of practice in scoring breathing-related distress for “breathing problems” using the PCOC SAS (Fig. 3).
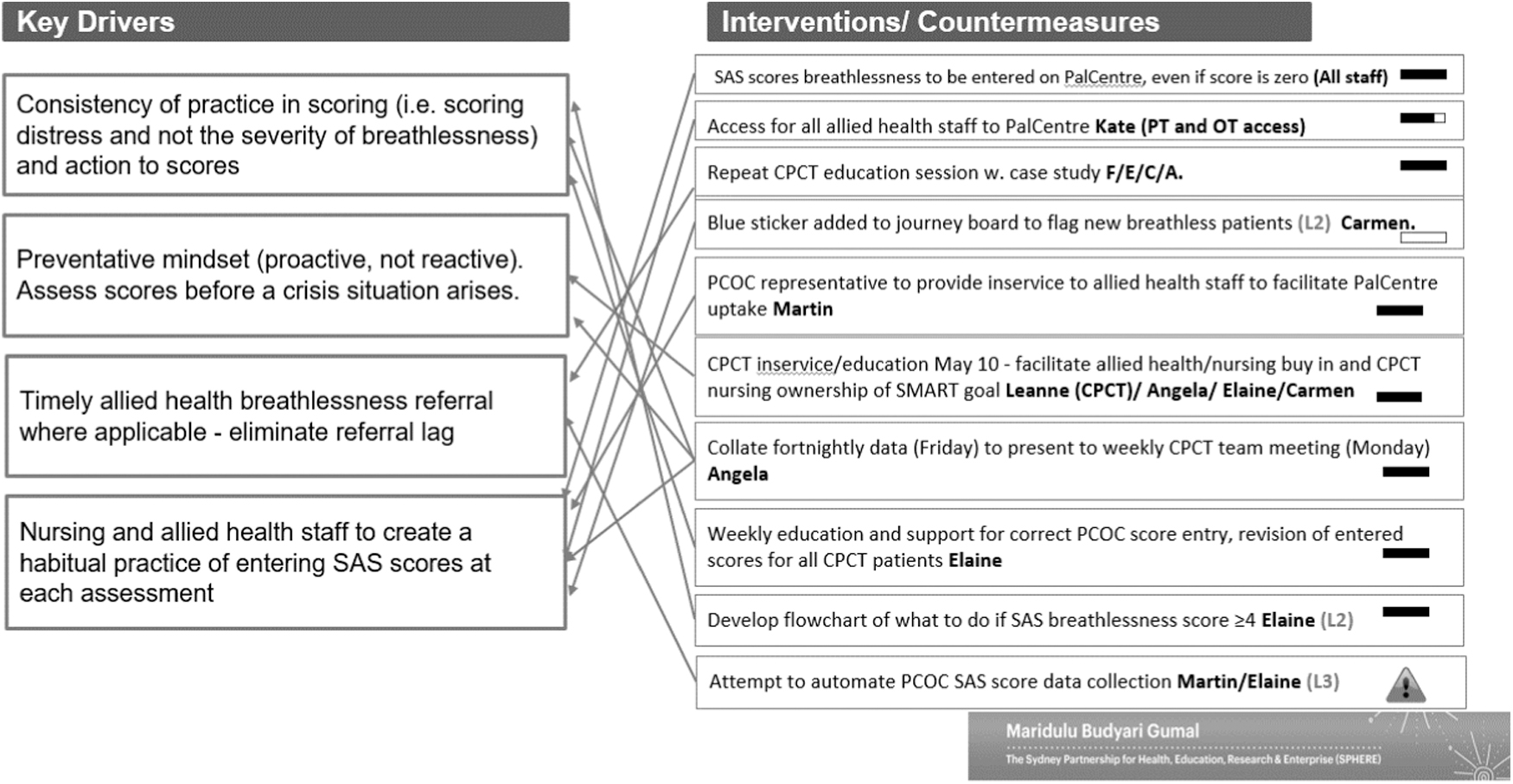
Key drivers and interventions. CPCT, Community Palliative Care Team; OT, occupational therapy; PT, physiotherapy.
Development and implementation of interventions linked to key drivers
First, to address key driver 1, we ensured that all members within the project team and community nursing and allied health staff within the organization had access to the PalCentre software and received internal training on how to enter PalCentre scores onto the software platform in real time (Fig. 3). PalCentre is a purpose-built program for health services participating in the PCOC data collection initiative, which captures information about patients, the interventions they receive, and their outcomes. An external education session by a PCOC representative was prearranged to facilitate PalCentre uptake. Staff were also encouraged to enter scores for “breathing problems” even where the score was 0. Common practice before the project was to only enter scores where PCOC SAS scores for breathing problems were ≥5, which may have limited the identification of some moderately distressed patients.
To address key driver 2, a flowchart created by our doctor (E.G.) was introduced to facilitate the timely assessment and management of breathing-related distress as an additional training tool (Fig. 4) and was delivered in an introductory session with community nursing and allied health staff in April 2021. The use of the Breathing, Thinking, Functioning (BTF) Assessment 17 as the gold standard of breathlessness assessment was reiterated and education on how to conduct a BTF assessment was provided by the community palliative care Nurse Practitioner (C.S.). The BTF Assessment outlines three cognitive and behavioral components of breathlessness that contribute to heightened reactivity and a cyclical worsening of symptoms. As part of the BTF Assessment, it is recommended that nurses address aspects of (1) breathing (respiratory rate, use of accessory muscles, dynamic hyperinflation, inefficient and/or increased work of breathing); (2) thinking (anxiety, distress, thoughts about dying, panic, misconceptions, attention to sensations, memories and past experiences); and (3) functioning (deconditioning of limb, chest wall and accessory muscles, reduced activity, tendency to self-isolate, needing more help from others) 17
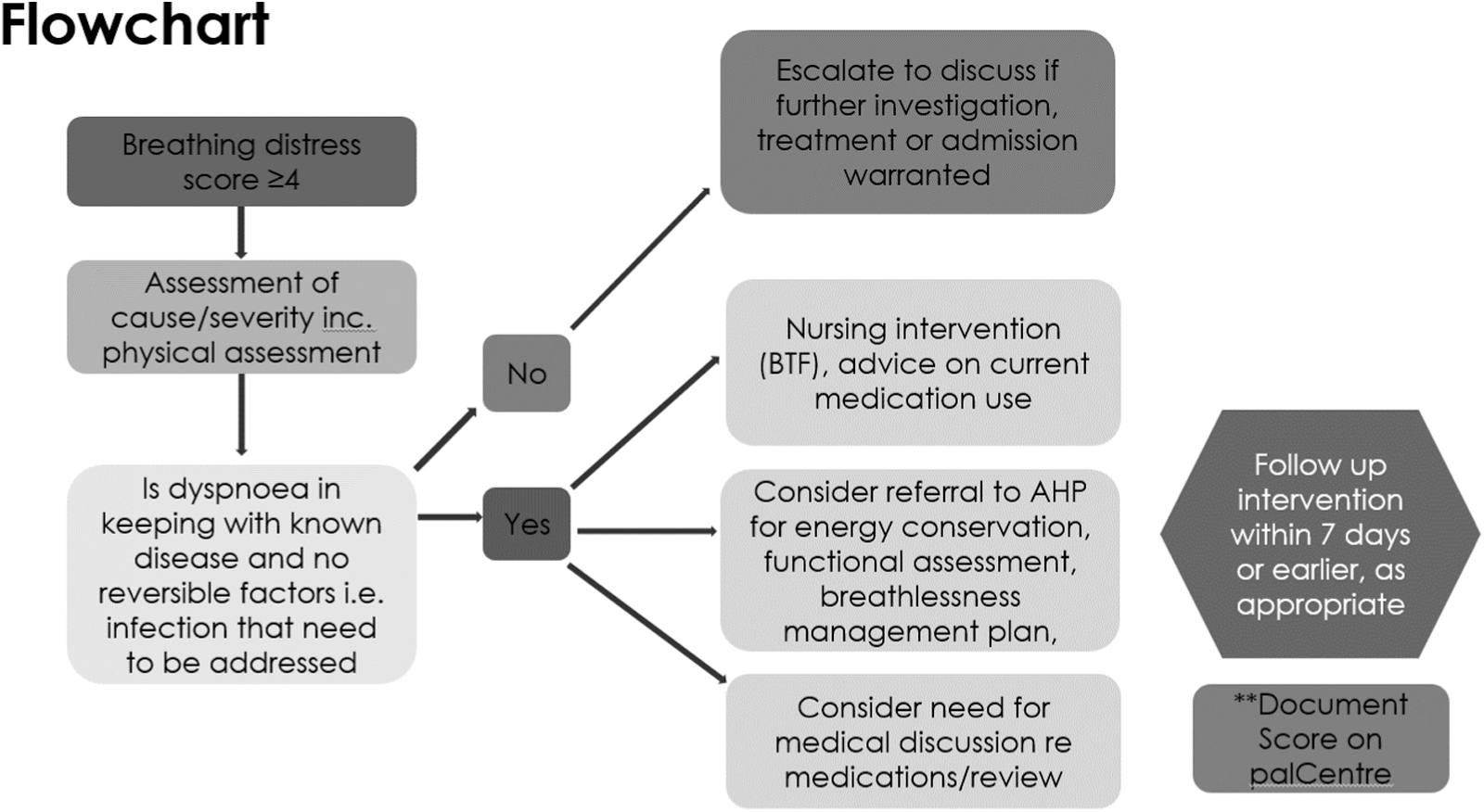
Flowchart for the assessment and management of moderate-to-severe breathing-related distress. AHP, allied health professional; BTF, breathing, thinking, functioning.
As momentum for the project grew within the team, a second education session was delivered in May 2021 to promote “buy-in” to the project and to facilitate nursing ownership of the SMART goal. At the end of this session, nursing staff agreed they were primary responsibility for ensuring that a follow-up assessment of moderate breathing-related distress was completed within seven days of their initial nursing assessment. This intervention addressed key drivers 3 and 2. The flowchart was refined to include clinician assessment of Resource Utilization Group-Activities of Daily Living, Palliative Care Problem Severity Scale, PCOC Phase, subsequent symptom management and follow-up, and was presented as a training tool for new and current community staff. Staff education was repeated in June 2021.
To address key driver 4, our doctor provided ad hoc advice and troubleshooting regarding inconsistent PCOC Phase and SAS scoring. A new process was commenced within the community palliative care team whereby newly admitted patients with moderate-to-severe breathing-related distress scores (and other symptoms) were reviewed and discussed weekly within the multidisciplinary team meeting to ensure that a timely plan for reassessment and management was in place (Fig. 5). It was also important to ensure that both new and existing staff understood and communicated clearly with their patients about the need to score distress related to breathlessness rather than the severity of the symptom. The distinction is made where a person could be coping or have adjusted to a chronic symptom and is not distressed by the symptom versus the need to provide nonpharmacological support and/or medical treatment for the onset of a new symptom that may be, for example, mild in severity but is distressing for the patient to experience.
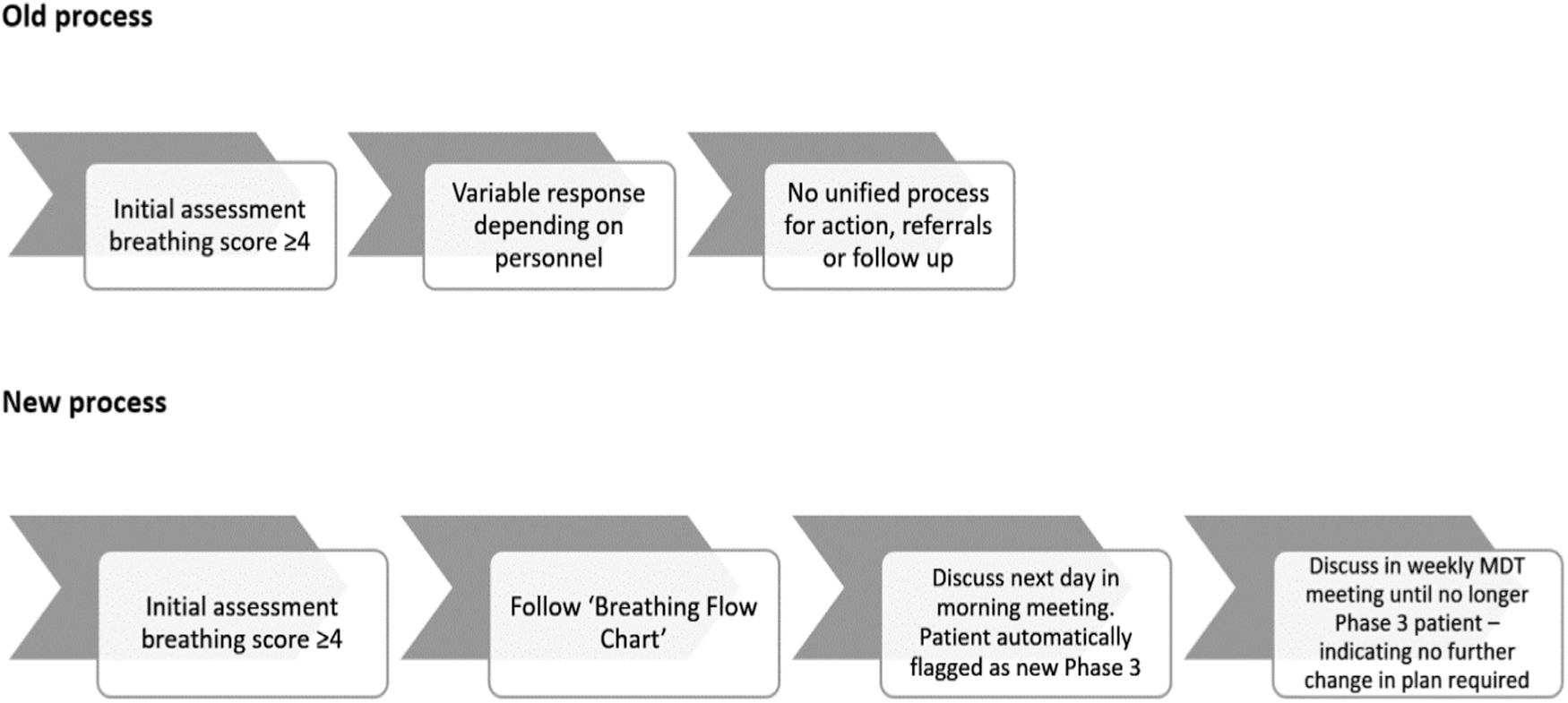
Process map for the timely assessment of breathing-related distress. MDT, multidisciplinary team.
A line graph template developed by Stanford University was used to present data to community palliative care staff to identify their current breathlessness assessment practices and identify opportunities for improvement. This addressed key driver 3. This line graph was presented at the education session with the community nursing and allied health team in May 2021. The line graph was updated monthly and presented again at the second education session in June 2021 to mark progress.
A routine of fortnightly updates of the proportion of patients with moderate-to-severe breathing-related distress who received a repeated SAS score for “breathing problems” within seven days were collated from PalCentre software into an Excel spreadsheet by the researcher (A.R-N.) and added to the line graph prospectively on a fortnightly basis until the end of the project in August 2021. These updates were disseminated through email to the team doctor before discussion at the next multidisciplinary team meeting.
Evaluation of the timeliness of breathing-related distress
Moderate-to-severe breathing-related distress was experienced by ∼21% (n = 181) of patients who were admitted to the service between September 2020 and August 2021. These patients were predominantly admitted due to a malignancy (81%, n = 151), with a median AKPS score of 50 (range 30–90) and a mean RUG score of 8 (standard deviation [SD] 5) (Table 4). At baseline, the mean number of days to reassessment of breathing-related distress was 8.3 (SD 11.3) days. During the intervention period, the mean number of days to reassessment of breathing-related distress decreased to 6.2 (SD 8.5) days.
Characteristics of Patients with Moderate-to-Severe Breathing-Related Distress (September 2020—August 2021)
AKPS, Australian Karnofsky Performance Scale; RUG-ADL, Resource Utilisation Group Activities of Daily Living; SD, standard deviation.
At the commencement of the intervention period in April 2021, the proportion of reassessments “breathing problems” that were completed within seven days increased to 50%, which was likely due to some clinical staff obtaining access to PalCentre software, and education about the necessity of the organization to comply with SAS score data entry to facilitate local PCOC benchmarking against national averages. By the end of May 2021, after initial staff education and introduction of the flow diagram, the proportion of patients with a reassessment of their SAS score for “breathing problems” increased to 60%. After the second education session in late June, the proportion of patients with a timely reassessment of breathing problems (i.e., within seven days) increased to 83%. By late July, after the introduction of fortnightly updates of patients who required a reassessment of their breathing-related distress, the proportion of patients with a timely reassessment of their breathing-related distress increased to 86% and then exceeded the project target by late August, reaching 92%. Overall, the mean increase in SAS breathing-related distress was 58% at the conclusion of the project (Fig. 6).
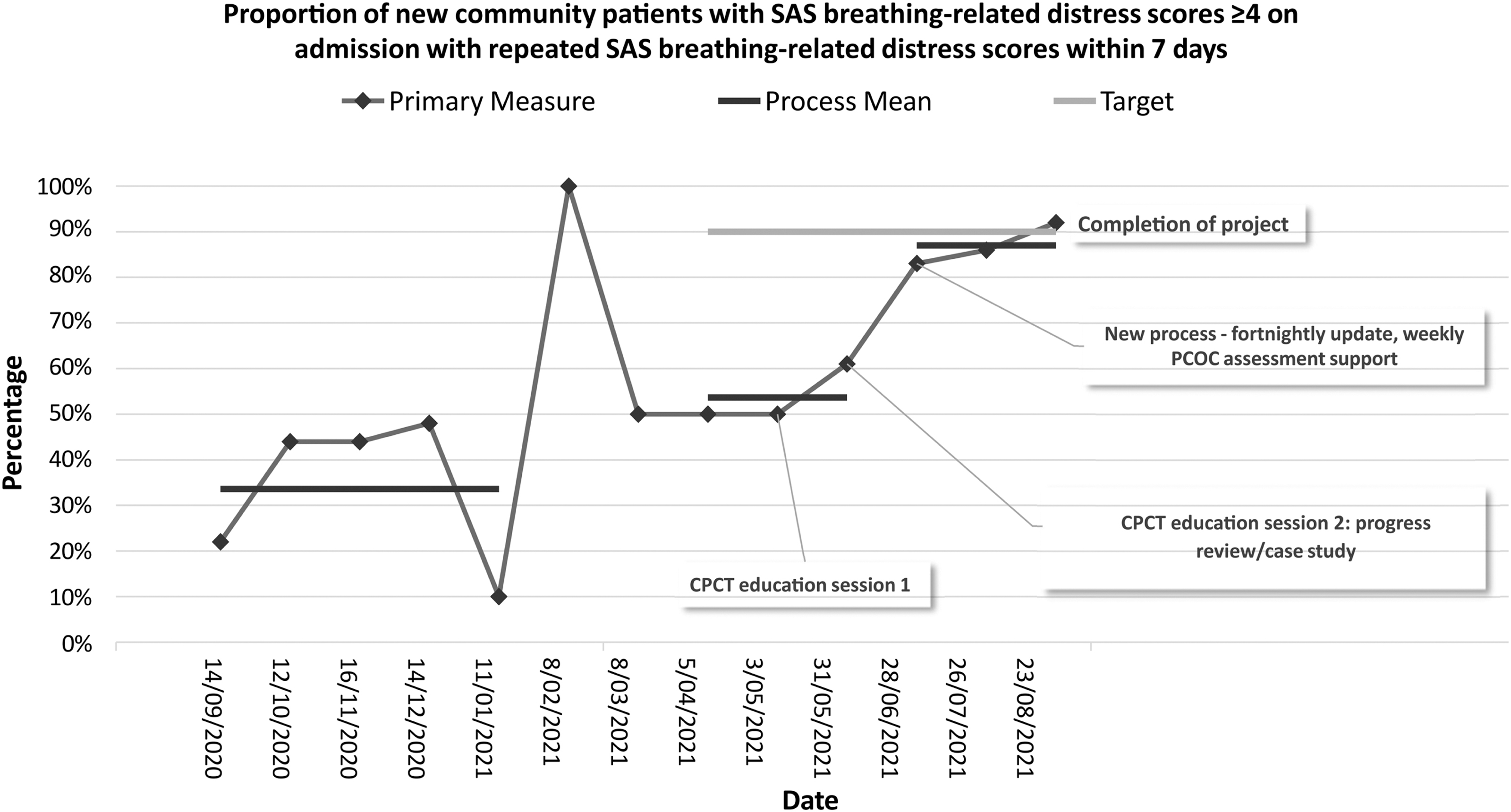
Proportion of new community patients with SAS breathing-related distress scores on admission with repeated SAS breathing-related distress scores within seven days. CPCT, community palliative care team.
Changes in breathing-related distress scores
The mean SAS Score for “breathing problems” among those with moderate distress decreased from 5.5 (SD 1.5) at initial assessment to 4.1 (SD 2.18) at second assessment, which reached statistical significance (p < 0.001). The proportion of patients with mild breathing-related distress (SAS ≤3) at the second assessment was ∼27% (n = 34).
Sustainability outcomes
Interventions were predominantly classified as Level 2 Procedures (embedded standard work, reminders), except for an attempt to automate PCOC SAS data collection, which was classified as Level 3 (automated systems) (Fig. 3). This attempt was abandoned, as it was considered outside the scope of the project. One other Level 2 planned procedure to introduce a blue sticker system to identify patients with moderate breathing-related distress was abandoned due to COVID19 lockdowns and the dispersion of the community palliative care team, which prevented the use of a shared physical space. Most interventions implemented reached maturity and worked well in operation.
Discussion
This QI project (1) identified patients experiencing breathing-related distress who required follow-up; (2) identified staff support needs for the scoring of breathing-related distress; and (3) embedded processes for the timely review of patients with moderate-to-severe breathing-related distress.
Different systems of reporting breathlessness between a Respiratory Chronic Care Program, and palliative care physiotherapy and nursing were found. Not all specialties routinely report PCOC breathing-related distress scores on a widely accepted and validated SAS, which is consistent with the literature.18,19 Nursing assessment usually included a brief summation of patient-reported symptom distress paired with clinical assessment, including listed medications and/or equipment in place to manage these symptoms. Nursing assessment could, but did not consistently include breathlessness education and management.
Limitations in providing optimal nursing care for breathlessness symptom management were largely due to time pressures and staff limitations, 20 where some staff perceived that they were only able to provide crisis management, rather than preventive care. Service provision, in particular, assessment capabilities such as chest auscultation was limited by COVID19 restrictions, which limited community home visits.
Nursing referrals to allied health staff often prioritized urgent equipment issues and fall prevention, while referrals specifically for breathlessness education and management were less prevalent. Management of severe breathlessness in people with symptoms or signs of underlying respiratory diseases triggered immediate comprehensive breathlessness-specific referral, education, and management. A physiotherapy referral often triggered comprehensive breathlessness assessment and education as part of their initial assessment, regardless of the reason for referral.
Implications
Innovative approaches to service provision to comprehensively address refractory breathlessness in a timely manner are needed. 21 This is essential in Australia where services to manage breathing-related distress are not available for palliative care patients with breathlessness who do not meet criteria for pulmonary rehabilitation clinics. 18 Consistent, timely, breathlessness-specific allied health referral of patients with moderate-to-severe breathlessness symptoms will likely improve the consistency of breathlessness assessment and management practices in the palliative care setting.
Improved nursing assessment of breathlessness symptoms and management practices, which includes a BTF assessment, may also improve patients' ability to manage their symptoms, and reduce distress. 17 Future research is required to understand if a comprehensive multidisciplinary breathlessness assessment and management program in the palliative care setting can improve the severity of symptoms in the context of functional decline and expected disease progression.
A palliative care breathlessness clinic also has the potential to shift nurse-led multidisciplinary patient care for breathlessness from a crisis management to a preventive mindset, which may reduce the frequency of specialist palliative care admissions and associated costs. 22 For example, in the United Kingdom, a complex multidisciplinary breathlessness intervention service with a maximum wait time of one week, which included medical review and pharmacological management, and selective use and application of a range of nonpharmacological strategies (e.g., hand-held fan, breathing control, activity pacing, relaxation, mindfulness and visualization, brief cognitive therapy, positioning, airway clearance techniques, and an individualized exercise plan), generated significant reductions in distress due to breathlessness. 22 Implementation of another breathlessness clinic that included activity repacing, breathing retraining, simple relaxation techniques, and psychosocial support over three weeks found significant reductions in functional capacity (walking distance without dyspnea and ability to climb hills or stairs) and breathing-related distress. 23
Reconfiguration of a day service to a closed self-management clinic to create capacity and enhance the experience of patients with fatigue, breathlessness, and anxiety also resulted in a 176% increase in annual contact hours, a 125% increase in contact time per patient, upskilling of staff to address breathlessness within multiple chronic conditions, and increased multidisciplinary support. 24
Limitations
This QI project was conducted at a single site, which reduces the generalizability of the findings to other community palliative care settings and contexts. The baseline reassessment rate reported may vary given the delayed uptake of PCOC electronic data capture at the site.
Conclusion
Implementation of a local QI project over a five-month period increased the proportion of community palliative care patients who were reassessed for breathing-related distress by a member of the multidisciplinary team within seven days.
Funding Information
No funding was received to complete this project.
Footnotes
Author Disclosure Statement
No competing financial interests exist.