
Abstract
Introduction:
Advancement in medical expertise and technology has led to a growing cohort of children with medical complexity (CMC), who make up a rising proportion of childhood deaths. However, end of life in CMC is poorly understood and little is known about illness trajectories, communication, and decision-making experiences.
Objective:
To synthesize existing literature and characterize the end-of-life experience in CMC.
Methods:
A literature search of MEDLINE, CINAHL, PsycINFO, Scopus, Embase, and Google Scholar was conducted up to August 26, 2021. Studies reporting CMC at end of life were included and the extracted data were analyzed descriptively.
Findings:
Of 1535 publications identified, 23 studies were included. Most studies (15/23 [65%]) were published from 2015 to 2021 and were quantitative in nature (20/23 [87%]). The majority of studies that extracted data from a single country (18/20 [90%]) originated from North America. Study outcomes were categorized into four main domains: (1) place of death (2) health care use (3) interventions received or withdrawn (4) communication, and end-of-life experiences. The weighted percentage of in-hospital CMC deaths was 80.6%. Studies reported that CMC had increased health care use and were subjected to more intensive interventions at end of life compared with non-CMC. Qualitative studies highlighted the following themes: Intrinsic prognostic uncertainty, differing perspectives of the child's quality of life, the chronic illness experience, a desire to have parental expertise acknowledged, surprise at the terminal event, the experience of multiple losses, with an overarching theme of the need for compassionate care at end of life.
Conclusions:
This scoping review highlighted important characteristics of end of life in CMC, outlining the emerging evidence and knowledge gaps on this topic. A better understanding of this cohort of seriously and chronically ill children would serve to inform clinical practice, service development, and future research.
Introduction
Children with medical complexity (CMC) are defined as individuals with substantial family-identified service needs, characteristic chronic and severe conditions, functional limitations, and high health care use. 1 Advancements in medical expertise and technology has led to a growing cohort of CMC, many of whom would not have survived previously. 2 CMC have unique health challenges, including that of constant medical fragility, fluctuating decline, and uncertain illness trajectories. 3 They are at high risk of morbidity and mortality and make up a rising proportion of childhood deaths. 4
End of life in CMC is often described as a challenging and even traumatic experience for patients, families, and health care providers. 5 However, end of life in CMC remains poorly understood with little known about illness trajectory, communication, and decision-making experiences. 6 Existing literature about end of life in children focuses mostly on children with cancer. 7 This lack of knowledge may compromise the clinician's provision of care and lead to communication gaps in the family/clinician encounter. 8 An enhanced understanding on this topic would serve to inform clinical practice, facilitate communication, and ultimately optimize care for CMC at the end of life.
The aim of this scoping review was to synthesize current literature and uncover characteristics and experiences at end of life in CMC. The study protocol was registered on the Open Science Framework (https://osf.io/cxnk3/?view_only=9dc05adce0594c26aee81403763b600d).
Methods
A scoping review methodology was chosen for this study to explore the extent of literature for this broad topic and to map and summarize the evidence to inform future research. 9 The Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review (PRISMA-Scr) statement 10 was used for reporting of the scoping review.
Search strategy and eligibility criteria
The search strategy was developed with a librarian and included five databases: MEDLINE (Ovid), CINAHL, PsycINFO (Ovid), Scopus, and Embase (Ovid). The full search strategies from all the databases are outlined in Supplementary Appendix SA1. In addition, gray literature was searched through Google scholar to identify additional documents. The search was not limited by date, language, or study design and the last search was conducted on August 26, 2021. Both empiric and review articles were considered for inclusion.
The review included studies with participants 0–21 years of age. Studies with participants over the age of 21 were considered if they included participants within the target age range. We included studies with participants who fulfilled the definitional framework of CMC by Cohen et al. 1 and who were at end of life, which we broadly defined as beginning when an illness, injury, or condition progresses to a point where the health status is diminished below a level that makes it impossible to live in a way that is meaningful or acceptable, and that might end with the patient's death. 11 Examples of keywords that fulfilled this broad definition of end of life were dying, terminal, hospice, and palliative. In addition, studies that explored experiences of parents and health care workers were included as long as their children or patients met the inclusion criteria. We excluded studies with only participants who were health care providers, patients with cancer, or over the age of 21 years.
Assessment of the titles, abstracts, and full texts were conducted independently by two investigators (G.M.C.N. and M.-H.B.). Any disagreement regarding study selection was resolved through discussion and moderated by a third party (H.P.) when necessary. Methodological quality was not assessed, as the authors had determined this was not necessary given the purpose of the study. 12
Data extraction and analysis
Data were extracted using a standardized data charting form by G.M.C.N. and then verified by M.-H.B. 13 Data on authors, settings, study aims, methods, patient characteristics, and results were extracted. The weighted percentages of study outcomes were calculated based on the sample size of each study using Excel. Qualitative data was analyzed using holistic content analysis. 14 In this interpretative process, data were read multiple times until common subthemes emerged. These subthemes were then clustered into themes and domains. Underpinned by individual empirical experience, reflexive analysis 15 was applied by G.M.C.N. and H.P. (content expert in CMC) across findings from all data streams.
Results
Identification of studies
Of the 2125 records retrieved, 26 publications from 23 studies were included in the scoping review. These included four reports from the same study, which were not considered duplicates.5,6,16,17 Figure 1 outlines the selection process in a PRISMA flow diagram.
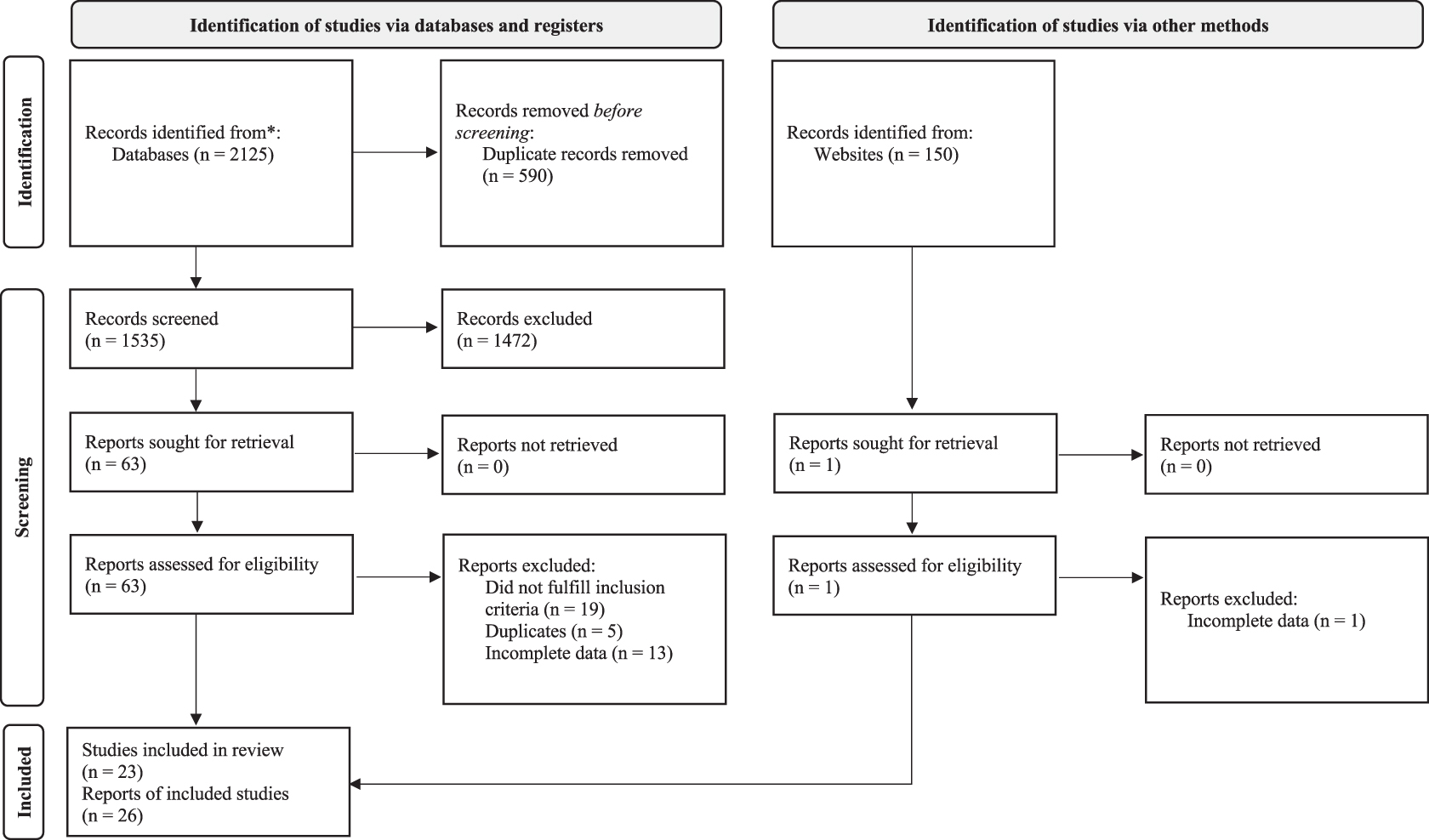
PRISMA flow diagram of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta Analyses.
Characteristics of included studies
Table 1 provides a summary and Figure 2 an evidence map of the studies included. These studies were published from June 2001 to July 2021, with majority of studies (15/23 [65%]) published from 2015 to 20212–7,16–27 (Table 2). Most studies that extracted data from a single country (18/20 [90%]) originated from North America.2–6,16–20,22,23,25,27–34 A range of study designs were used, most of which were quantitative in nature (20/23 [87%]).4,7,18–35 All quantitative studies were observational. Most studies collected data on subjects who were patients (20/23 [87%])4,7,18–35 and these were predominantly decedents (21/23 [91%]).3–7,16–18,20–35 Approximately half [11/23 (48%)] of studies included both CMC and non-CMC17,21,23,24,27–32,35 and most studies (18/23 [78%]) used the definition of complex chronic condition (CCCs) defined by Feudtner et al.4–6,16–25,27–32,34,35 We categorized heterogeneous study outcomes into four main domains: (1) place of death (2) interventions received or withdrawn (3) health care use (4) communication and end-of-life experiences.
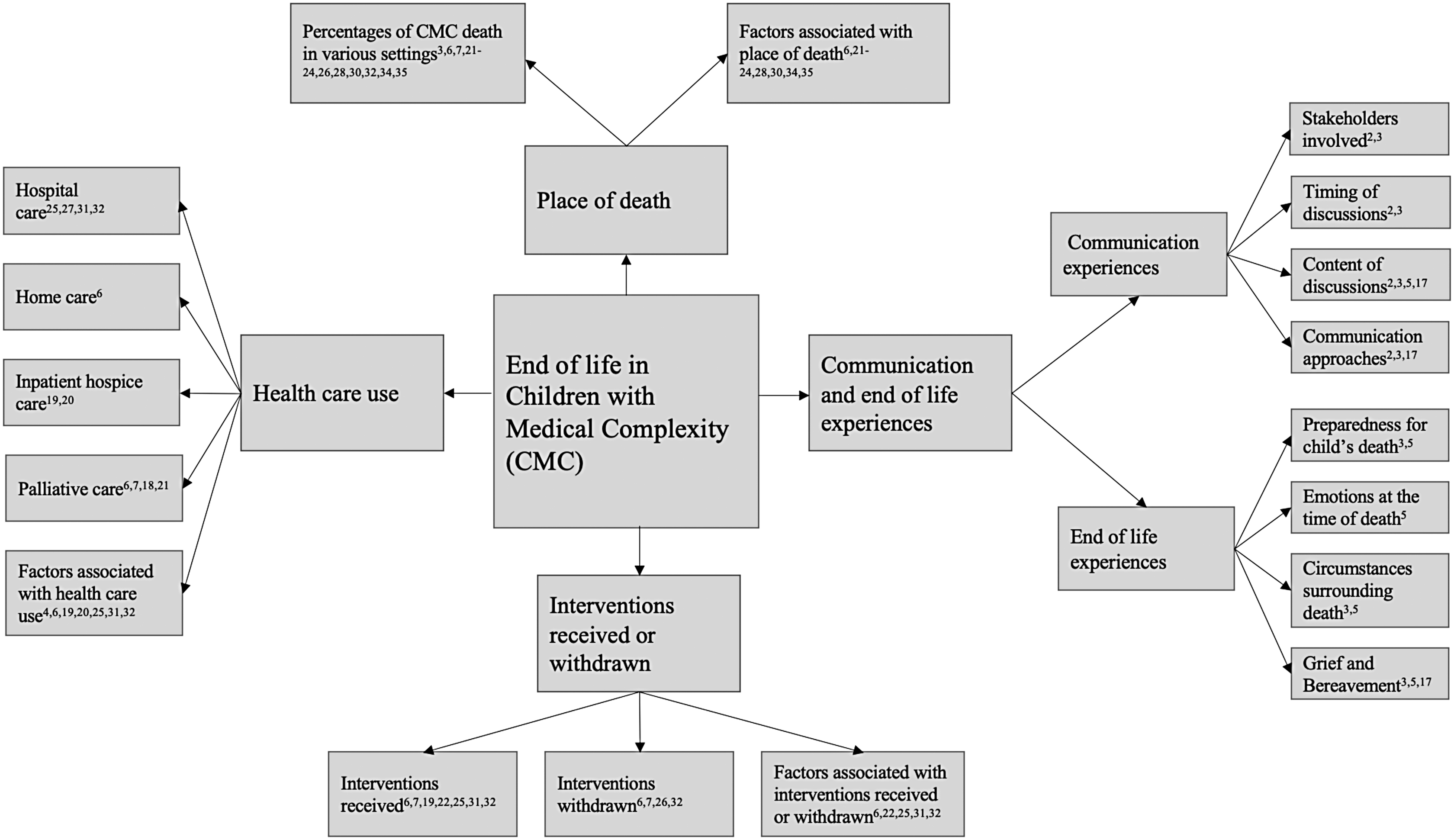
Evidence map of studies that investigated end of life in children with medical complexity.
Summary of the Included Studies
These four articles came from a single study and were not considered duplicates.
ACP, advanced care planning; CCCs, complex chronic conditions; CMC, children with medical complexity; CNS, central nervous system; ED, emergency department; ICU, intensive care unit; LT-CCCs; life-threatening complex chronic conditions; MCCCs, multiple complex chronic conditions; PC, palliative care.
Characteristics of the Included Studies
Denominator used for percentage calculation for this variable is 20.
Studies evaluated more than one outcome.
Place of death
Place of death was the most frequently studied outcome, which was investigated by 52% (12/23) of studies. The weighted percentage of CMC deaths occurring in the hospital was 80.6% (33.5%–91.9%) and that occurring at home was 14.9% (0.0%–50.0%) (Table 3). Of children who died in the hospital, the weighted percentages of those dying in the intensive care unit (ICU), general ward, and emergency department were 44.1%, 58.3%, and 4.5% respectively. CMC deaths were increasingly occurring at home, as reported by two studies that had evaluated trends of place of death over time.28,30
Summary of Study Outcomes
BiPAP, bilevel positive airway pressure; CPR, cardiopulmonary resuscitation.
Multiple factors associated with place of death were investigated, including that of age,21–23,30,35 CMC diagnostic category,24,28,30,34,35 and sociodemographic variables21,28,35 (Table 3). While individual studies demonstrated associations between these factors and place of death, the findings were not consistent across studies and statistical analyses to pool the results together were beyond the scope of this review.
Interventions received or withdrawn
Multiple interventions that CMC received at end of life were studied, with a focus on life-sustaining interventions (Table 3). The most frequently studied intervention was mechanical ventilation, and the percentage that received mechanical ventilation ranged from 13.7% to 76.0% across different study periods.7,21,22,25,35 Where both groups were reported alongside, CMC were more likely to be mechanically ventilated and to be ventilated for a longer duration as compared with non-CMC.31,32 Specific diagnoses within CMC were found to be associated with medically intense interventions at end of life,6,22,25,32 but again, the reported associations were not consistent across studies.
Interventions that were withdrawn included that of mechanical ventilation, enteric feeding, and inotropic medication.6,7,26,33 Withdrawal of interventions was not the focus of most studies, except for one study that evaluated the experience of palliative extubation in a pediatric hospital. The main findings were that most palliative extubations occurred in the ICU and the time between mechanical ventilation withdrawal and death ranged from 15 minutes to 2 years. 26
Health care use
The four types of health care use by CMC at end of life reported by studies were that of hospital care, home care, inpatient hospice care, and palliative care (PC).4,6,7,18–21,25,27,31,32 Measures of hospital care use included that of hospitalization rates, duration of hospitalization, ICU admission rates, and hospital costs. CMC were hospitalized more frequently and for longer periods than non-CMC, with the rate of hospital admission rising nearing death.31,32 Common factors found to be associated with health care use were that of CMC diagnostic category,4,6,20,25,31,32 number of CCCs, 19 and age4,31 (Table 3).
Studies reported that PC involvement ranged from 28.0% to 88.2%.6,7,18 A study reported that CMC who received PC had longer hospitalizations, fewer prescribed medications, greater referrals for art therapy, and were more likely to have limits of resuscitation established compared with those who did not. 18 Another study found that although over 1000 children die from chronic complex conditions each year in Korea, there were no hospitals or institutions in the country that met minimum standards for specialized pediatric PC at the time. 21
Communication and end-of-life experiences
Communication and end-of-life experiences were examined by both quantitative and qualitative studies. Quantitative studies reported that the percentage of patients who had documented end-of-life discussions ranged from 51.0% to 72.0%.6,7,16,33 Edwards et al. reported that the most common context for initial advanced care planning (ACP) discussion was that of progression of underlying condition, followed by acute deterioration and new comorbidity. 33 Another study found that most parents desired ACP discussions, felt discussions should be initiated by ICU or subspecialty clinicians, and felt more prepared for their child's death if they had ACP discussions with their child's health care providers. 16
Qualitative studies examined the experiences of parents and health care providers. These experiences were grouped into two main domains: (1) communication experiences and (2) end-of-life experiences.
Domain 1: communication experiences
Communication experiences of CMC and families at end of life comprised the following four themes: (1) stakeholders involved, (2) timing of discussions, (3) content of discussions, and (4) communication approaches, with subthemes and example quotations listed in Table 3.
Subthemes that were particularly relevant in this domain included prognostic uncertainty, perception of child's quality of life, chronic illness experience, and recognition of parental expertise.
Parents described a high degree of prognostic uncertainty, as an aspect of their child's unique situation that needed to be considered during ACP discussions.
“It was really hard to gauge … whether [son] was going to give us two weeks or the extra year and a half that he did.” 3
The chronic illness experience also played a role in decision making. Although parents described previous resuscitation events, multiple medical problems, and frequent hospitalizations indicating medical fragility, many parents remained hopeful that their child would pull through.
“We thought she was improving and the final stroke that killed her was totally unexpected. She had survived the lung and liver failure, survived the lung and liver transplant, survived the first stroke…” 5
Parents shared that their child's quality of life was often underestimated by health care providers, thus highlighting the importance of asking parents what they were like at baseline.
“Their automatic assumptions… this is all the things she has wrong with her, oh, her life at home is horrible, she has a painful life, she probably lays in bed, all day, she does nothing. And we're like, what, they doesn't describe her at all.” 2
Lastly, parents implored health care teams to listen to them and showed appreciation when their own expertise in their child's care was valued in the decision-making process.
“They have to listen to parents, I didn't want her poked a million times. I knew where the best place was… I think things could have been done very differently if they would have listened to me…” 3
Domain 2: end-of-life experiences
Themes that emerged relating to end-of-life experiences were: (1) preparedness for child's death, (2) emotions at the time of death, (3) circumstances surrounding death, and (4) grief and bereavement (Table 3). In this domain, important subthemes to highlight were that of parents feeling surprised by their child's death and the experience of multiple losses.
Even though parents were aware of their child's life-limiting condition, the common experience reported was that the death of their child came as a shock.
“It came as, a shock, even though knowing that every day was a gift with [son], because I didn't realize how quickly things could happen.” 3
Parents also described multiple losses with not only the loss of their child but also the loss of relationships with the child's health care team when their child died.
“We were so involved in the medical world throughout my son's life… When he died, that all suddenly stopped since there is now no reason to go to the hospital. It's like falling off a cliff.” 17
An overarching theme of having a compassionate approach was prominently featured in both domains of communication and end-of-life experiences,2,3,17 highlighting the profound impact that kindness, sensitivity, and respect had on families during their child's end-of-life journey.
“We were overwhelmed by the kindness and respect from the staff. There was one very special nurse who had cared for my son at the end who came in to be with us after he died even though she was not on duty… For this kindness we will forever be grateful.” 17
Discussion
To our knowledge, this scoping review is the first to synthesize current literature on the end-of-life experience in CMC. Twenty-three studies in the final review described important characteristics during that period; a few studies contrasted the phenomenon between CMC and non-CMC,23,27,31,32 suggesting that the CMC experience may be unique to their cohort.
Quantitative studies demonstrated that the majority of CMC deaths occurred in the hospital, with increased health care use and intensive interventions. We postulate that this is a reflection of the lived experience of many CMC; with their history of multiple previous life-threatening deteriorations and ultimately, a level of recovery sufficient to return home with their families. Families learn that CMC are both fragile, with sudden and severe deteriorations in their health, and resilient, with recovery after recovery, although not necessarily returning to a previous level of health over time. Thus, an end-of-life discussion with a health care provider who is not informed about a specific child's trajectory over time may seem presumptuous to a parent who has seen their child recover from a similar episode previously. This push-back from parents is often perceived by the health care team as parental denial and as a lack of understanding by the family. 17 Unlike children who are clearly dying, for example, because of progression of a cancer that is not responding to curative treatment, there is not necessarily a clear signal for parents to indicate which crisis will be their child's last; this is reflected in the theme of surprise at the actual death of their child.3,5
The lack of a clear signal along with an overall goal to return home with their child for as long as possible explains parental choices for life-sustaining interventions when these may seem futile to a health care professional who is not informed on the child's history of recovery, resilience, or what quality of life means to the patient and family. It is thus not surprising that conflicts arise between families of CMC and health care teams when goals of care for the child are not aligned. In light of these findings, we propose that we should not be perplexed when families choose these life-prolonging options, but to take a compassionate, patient, and nonjudgmental approach in acknowledging their lived experiences and understanding why and how these families arrived at these decisions. Creating a safe space to listen to these personal narratives would greatly support families as they go through the traumatic experience of their child's life-threatening episode and may ease the moral distress that health care professionals encounter in such situations. 36
Our scoping review also found that CMC diagnostic category was associated with end-of-life outcomes. CMC is well known to be a clinically heterogeneous population with a myriad of different diagnoses, 37 and our findings suggest that this diversity also impacts the end-of-life phase of their illness. Studies reported that the different CMC subtypes had different illness trajectories, end-of-life symptoms, available health care resources, which contributed to the observed differences in patterns of end-of-life care and outcomes.6,25 Kim et al. reported that the diversity of diagnoses made it difficult to create a comprehensive plan for supporting PPC services nationwide. 21 These findings support the ongoing efforts toward a tailored and multidisciplinary approach for end-of-life care in each CMC subtype 23 and guides future research and educational opportunities. For example, Johnston et al. proposed follow-up studies that target the subspecialties with the greatest number of patients receiving high-intensity end-of-life care. 22
Lastly, our scoping review highlights interesting characteristics of the 23 studies synthesized. Majority of the studies were quantitative, perhaps reflecting the importance of large-scale epidemiological studies to identify health care system level opportunities and challenges. 31 Using quantitative methods alone were acknowledged as a limitation in understanding the lived experiences of patients and families at the end of life4,31 and we recommend that more qualitative approaches in future research should be considered to bridge this gap. Even though the search was not restricted by language, majority of publications were North American. This could reflect more established programs and research interests in CMC in this region and highlights a need to better understand the experience in other parts of the world. Lastly, the increasing number of publications on this topic over the past six years are consistent with the trends in the increasing prevalence of CMC 1 and greater interest to study this cohort.
Limitations and recommendations
Our scoping review design has limitations related to our search strategy and analytical procedures. Our decision to focus on patients and families in this study reflects our valuing of their perspectives as the main stakeholders in this first scoping review. We acknowledge that, in choosing this area of focus, we have excluded articles that could give additional insights from the health care professionals' perspective. Exploring the views of health care professionals on this topic would be an ideal follow-up study, especially in understanding the communication gaps and distress in the clinician/family encounter. We also recognize that using pooled averages may reflect findings from studies with a larger number of participants and that in-depth statistical analysis methods such as a meta-analysis may provide more meaningful summaries of the quantitative results. Only Google Scholar was searched for gray literature due to resource and time constraints and we recognize that there could have been potential gray literature sources that were not found.
In terms of identifying gaps in the literature, we noted that there were few to no studies on ethical issues, studies on perspectives from patients themselves, and end-of-life care for CMC in the home and community, and these could serve as possible topics for future research.
Conclusion
This scoping review highlighted important characteristics of end of life in CMC and outlined the emerging body of literature as well as knowledge gaps on this topic. A better understanding of this cohort would serve to inform clinical practice, service development, and future research opportunities.
Footnotes
Acknowledgments
The authors would like to thank Ms. Taline Ekmekjian and Ms. Amy Bergeron for their assistance in developing the search strategy. The authors would also like to thank Mr. Yeo Zhi Zheng and Dr. Chong Poh Heng for their advice during the article writing process.
Authors' Contributions
G.M.C.N.: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing (original draft), visualization, and project administration. M.-H.B.: methodology, validation, investigation, and writing (original draft). H.P.: conceptualization, methodology, validation, formal analysis, investigation, writing (original draft), and supervision.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.