
Abstract
Palliative care improves outcomes, yet rural residents often lack adequate and equitable access. This study provides practical tips to address palliative care (PC)-related challenges in rural communities. Strategies include engaging trusted community partners, addressing cultural factors, improving pediatric care, utilizing telehealth, networking with rural teams including caregivers, and expanding roles for nurses and advanced practice providers. Despite complex barriers to access, providers can tailor PC to be patient-centered, respect local values, and bridge gaps. The “Top 10” format emphasizes the relevant issues to enable clinicians to provide optimal care for people from rural areas.
Introduction
Specialty palliative care (PC) improves symptoms, increases patient and family satisfaction, targets care to patients' goals, and is associated with cost savings.1,2 Robust evidence supports the use of early PC for patients with advanced illnesses, 3 but these recommendations are primarily based on trials conducted in urban areas. Less is known about the applicability to rural communities. 4 Sixty million Americans, or nearly one-fifth of the population, live in rural areas. 5 Ninety percent of hospitals with PC are in urban areas, and only 17% of rural hospitals have PC programs. 6
Providing PC to individuals in rural areas presents a distinct set of challenges and opportunities. Navigating these areas, where access to specialized services can be limited, requires PC providers to adapt and overcome a host of obstacles. By understanding rural areas' strengths and challenges, providers can work toward ensuring that individuals living in these regions have access to quality palliative and end-of-life care that meets their unique needs and goals. These “Ten Tips” attempt to both offer urban PC specialists' the chance to learn about rural care while also providing a model for helping rural providers to understand more about delivering primary PC.
Tip 1: Rural Health Disparities Include Higher Mortality Rates and Diminished Life Expectancy, in Stark Contrast to Urban and Suburban Communities
Rural health disparities are not homogeneous, but rather vary depending on the community and region of the country. Despite this heterogeneity, the barriers to health care share common themes such as lack of access to providers and reliable technologies7–9 and lower income and higher poverty rates.10,11 Also importantly, there exists relatively less private insurance coverage due to higher unemployment or working in jobs that do not have employer-provided health insurance, requiring higher use of public program coverage(s) or uninsurance. 12
Rural individuals are more likely to have multimorbidity 13 such as cancer, heart disease, and lung disease. 14 Age-adjusted death rates in rural areas exceed those of populations living in metropolitan areas. 14 A persistent gap in life expectancy has remained between rural and urban populations, with the convergence of rurality and poverty resulting in a significant disparity (Fig. 1). 15
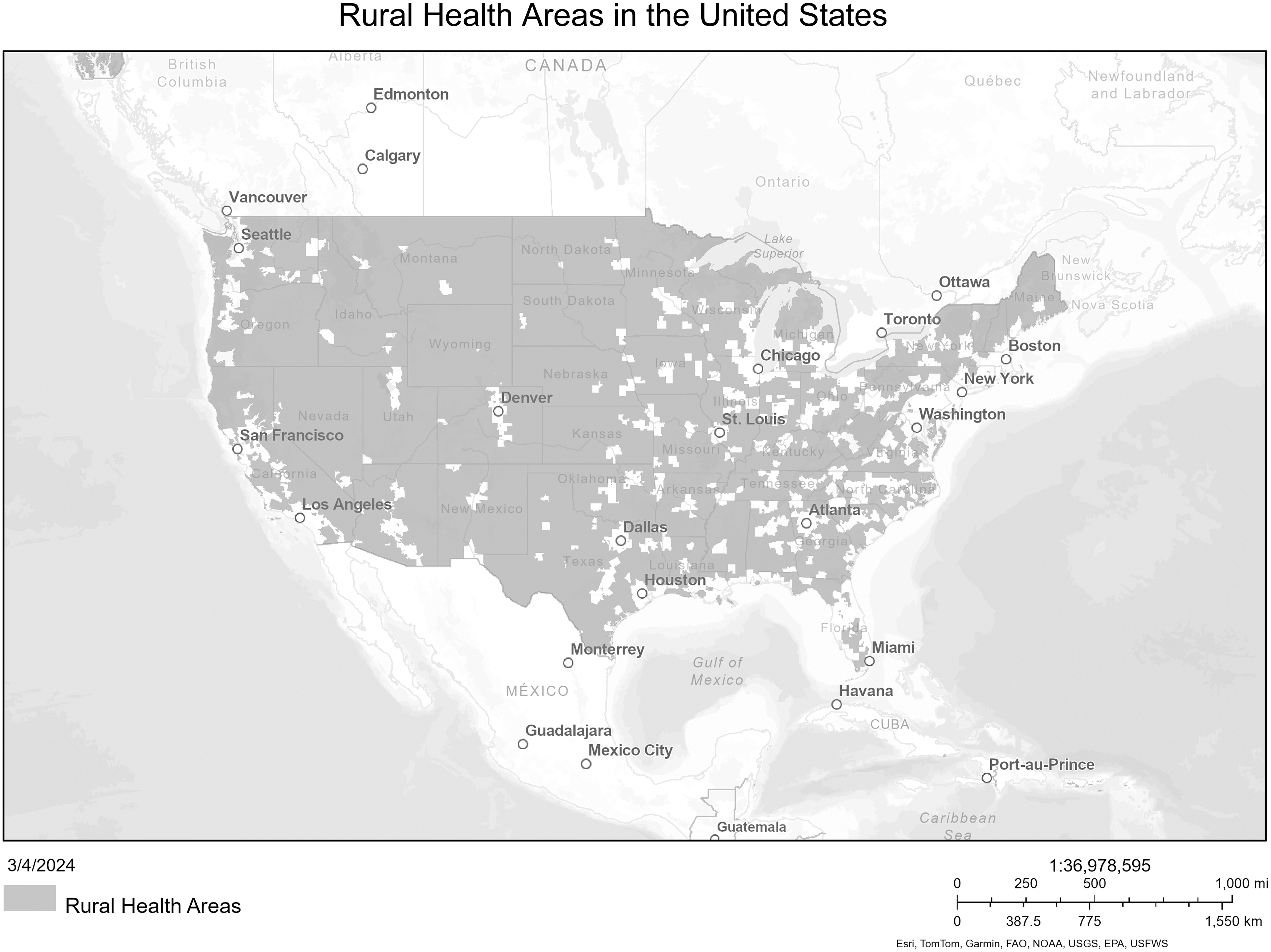
Map of regions designated Rural Health Areas by the Health Resources and Services Administration.
Tip 2: The Scarcity of Clinicians, Pharmacies, and Medications Converges With the Opioid Epidemic to Limit Access to Essential Health Care Resources
In rural regions, there are lower per capita rates of primary care and specialist providers compared to urban areas. 16 Additionally, many retail pharmacies have disappeared due to declining populations, increased usage of mail order firms, rising prices, and lack of personnel, leading to “drug store deserts.”17,18 Consequently, people are sometimes forced to drive long distances to receive their medications 18 while at the same time facing constraints such as lack of public transportation, paucity of wheelchair-accessible vehicles, driver shortages, and poor road conditions. 19 With fewer pharmacies, patients face critical challenges in obtaining medications for pain and symptom management.
The recent scarcity of certain opioids and evolving opioid prescribing limitations present significant barriers for people living in rural areas. 20 These challenges unfold amidst the backdrop of rising rates of opioid misuse and overdose deaths nationally. That said, rural individuals also continue to have a higher likelihood of receiving opioid prescriptions. 21 This dangerous mix is an added challenge to already existing obstacles to accessing safe prescription pain treatments (Fig. 2).
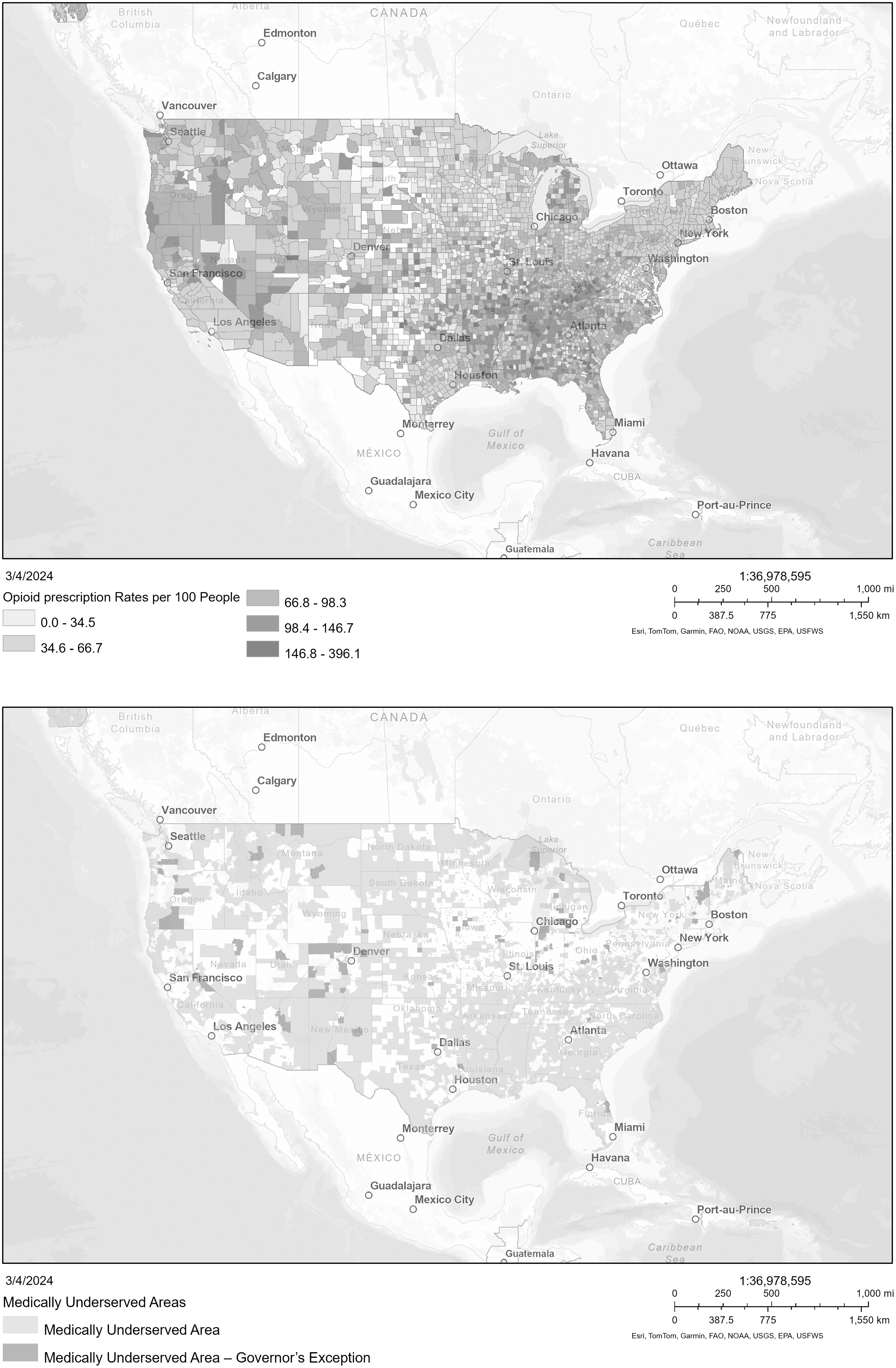
Top map: Opioid prescription rates per 100 people. Bottom map: Medically Underserved areas. Source: Health Resources and Services Administration.
Tip 3: Local PC Champions and Community Engagement Can Serve as a Fundamental Strength for Rural PC Teams
Individuals living in rural areas know their community best and often create bonds similar to those shared among family members. 22 These relationships can provide insight into decision-making that is unmatched in outsider relationships, highlighting the need to identify and engage local PC champions in the effort. Strong social infrastructure leads to community attachment and engagement. 23 Supports can be leveraged to strengthen PC services through PC champions (Fig. 3). 24
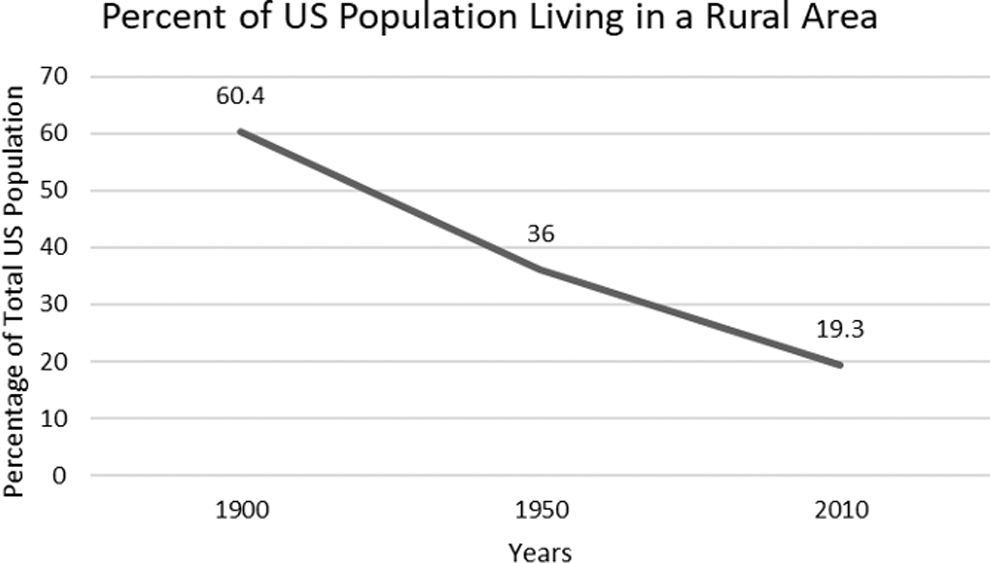
Percentage of the US population living in rural areas. Source: US Census Data.
Rural regions provide an opportunity to broaden our thinking about who may comprise an interprofessional team. Advocates not only can consist of health care professionals, such as nurses, advanced practice providers (APPs), physicians, social workers, first responders, and community health workers, but also laypersons such as clergy, fitness instructors, and hair stylists. Places such as churches, senior citizen centers, and rotary clubs are critical vehicles to strengthen community resiliency. 23 Engaging family caregivers is also essential as they are more knowledgeable about the supportive care needs of the patients and the local resources unique to their rural community. Collaboration is key to improving the quality of life of patients and families.25,26
Identifying and training local PC champions enhances care provision 24 by integrating PC into primary care practice as a standard of care 27 and focusing on providing primary PC education and services to local community members. These PC supporters improve awareness of PC and its benefits and encourage others to learn about PC. 26
Tip 4: Sensitivity to Cultural Practices and Beliefs Is Essential for Effective Rural PC and Advanced Care Planning
Circumstances that have impacted care in rural areas include a lack of family caregivers, decreased health literacy, the need to travel long distances, and sometimes even the rural terrain itself, which can limit palliative and end-of-life care for this vulnerable population of people.28–30 Different cultural care practices can create barriers to care including the feeling of surrendering to an illness or giving up hope for a cure.28,31 Resistance to PC can also result from the belief that palliative or hospice care will hasten death. Interdisciplinary, culturally congruent education for all providers and community caregivers could be a way to dispel myths and increase understanding of PC options. 28
There is a need to support a workforce that can care for diverse populations, including children, preserve folk practices when making decisions for care, and communicate with family in a way that is easily understood.28,29 Providers should practice cultural humility in their care practices and communication. Family values and resources should be assessed and advance care planning should accommodate these values and resources.
Rural teams may be skeptical of advice from urban or academic teams, as significant qualitative differences between urban and rural health care systems give rural-to-rural interactions the greatest credibility and value. When local skills grow and are augmented by telehealth consults from PC specialists, patients can stay in their communities and receive excellent, trusted care. As one individual in a frontier area testified, “This is the first time the people in the healthcare system listened to me so fully and cared about what I wanted. I am so relieved I can stay home.” 32
Tip 5: Disparities in PC Services Among Racial and Ethnic Minorities in Rural Areas Require Special Attention
PC programs and services have expanded in the United States in recent years. However, disparities to access persist among individuals representing racial and ethnic minority groups. 33 There is an urgent need for targeted interventions. 34 Racial and ethnic groups face inequitable access to timely and appropriate services resulting in incomplete advance care planning and lower likelihood of receiving PC services at all.34,35 PC is often perceived as giving up or end of life, and these cultural meanings create misconceptions and act as major barriers. 36
There is a need to increase awareness and education about PC and advance care planning that is intentionally inclusive of minority populations, for example, by partnering with trusted faith leaders and parish nurses. 37 Providers should value and demonstrate compassion toward the culturally specific PC needs and concerns of the patients and their families. 38 This will help in building mutual trust and minimizing caregiving strain and compassion fatigue. 39 Recruitment and training of diverse staff must also be a priority. By implementing these measures, we can move closer to equitable access for racial and ethnic minorities in rural areas, ultimately fostering a system that provides support to all individuals.
Tip 6: Children Face Some of the Greatest Barriers to PC and End-of-Life Care in Rural Areas
With all major free-standing children's hospitals located in urban areas, 6 rural pediatric PC services are severely limited. Lack of pediatric-trained personnel is often cited by providers as the greatest challenge to caring for children. 40 Building and nurturing relationships between specialist pediatric PC providers and rural health care workers is key. Tele-health maybe helpful in bringing specialty PC access to individuals who are isolated from PC.
Adult hospice, which is more prevalent, and PC teams can apply their expertise to caring for pediatric patients and their families. Coalitions can help further educational opportunities, especially learning more about parent/caregiver psychosocial support, goals of care, and symptom management. 41 Provisions in the Affordable Care Act broaden the eligibility of hospice care for children since those patients can now continue receiving curative or life prolonging therapies while benefitting from hospice care. 42 In spite of this payment mandate, children often lack access to end-of-life care in rural areas given lack of care teams discussed above. 30
Tip 7: Medicare's Traditional Payment System Adds Complexity to the Challenges of Ensuring Proper Reimbursement
Many rural providers are more dependent on Medicare and Medicaid than their urban counterparts and often struggle to keep afloat. Financial reimbursement for PC services generally happens through Medicare's physician fee schedule using fee-for-service visits and/or care management services. 43 In addition, since there is not a separate Medicare PC benefit, many rural PC services are provided through the home health or nursing home Medicare benefits by incorporating the PC philosophy into care.
In the outpatient setting, Rural Health Clinics (RHC) and Federally Qualified Health Centers (FQHC) are important safety net providers, with enhanced reimbursement rates for Medicare and Medicaid services.44,45 However, the billing is complex. RHCs must comply with unique billing requirements, along with meeting traditional Medicare regulations.46–48
Before 2022, RHCs and FQHCs could not bill for chronic care and transitional care management or another program that provides additional payment for care management services for the same beneficiary during the same time period. 49
Since this policy changed starting in 2022, where Centers for Medicare and Medicaid Services (CMS) will allow RHCs and FQHCs to bill concurrently for care management services, the issues are primarily understanding and awareness of what can now be billed, capacity and systems for documentation to support billing, and concerns over patient cost sharing if the patient does not have supplemental insurance (Table 1).
Six State-Based Approaches to Advance Palliative Care (PC)
Source: Donlon et al. 70
Tip 8: Telehealth Is Crucial for Care in Rural Regions But Comes With Its Own Challenges, Including Broadband Infrastructure Accessibility and Reimbursement
The rural/urban divide in broadband access has narrowed in recent years, but ∼17% of Americans in rural areas lack coverage compared to only 1% of urban dwellers. 50 Telehealth, a diverse set of services comprising synchronous audio/video, audio-only, and remote monitoring, is essential to ensure that all patients, regardless of mobility status or geographic location, receive necessary PC services.
Video can allow providers to see patients and families and vice versa at home or in nearby locations and reduce travel. 51 Patients have reported positive experiences in both telehealth and in-person visits. 52 Furthermore, video technologies can allow for rural providers to access training, as in the example of Project ECHO (Extension for Community Healthcare Outcomes)—an educational “hub-and-spoke” model that pairs palliative specialists with community providers for education and mentoring.53,54
However, challenges remain including the need for access to reliable broadband infrastructure and the technology to conduct telehealth visits. 55 Policies that support infrastructure development and provide access to technology in rural areas can support rural telehealth PC access. Differences in Medicaid reimbursement for audio-only, audio/video, and in-person delivery may also affect accessibility depending on parity laws across states. 56 Several Medicare flexibilities around telehealth reimbursement instituted during the COVID-19 pandemic will end in 2024, and providers must confirm which services are reimbursable via telehealth.57,58 Providing virtual access to PC can bring quality of life-enhancing services to rural individuals with serious illness. 59
Tip 9: Rural PC Teams Flourish by Learning from and Networking with Other Rural Teams Given Similar Challenges and Barriers
To begin PC development, a local champion must be identified to help facilitate a community “needs and gaps assessment” and recruit team members. Foundational components include training to increase professional knowledge and awareness, development of clinical skills, and communitywide processes for advance care planning and community education. The PC champion building a PC service may never have planned a new program. While expert resources are important, the exchange between rural PC champions offers key benefits that can only come from interactions with peers who share common goals within similar environments (Fig. 4).
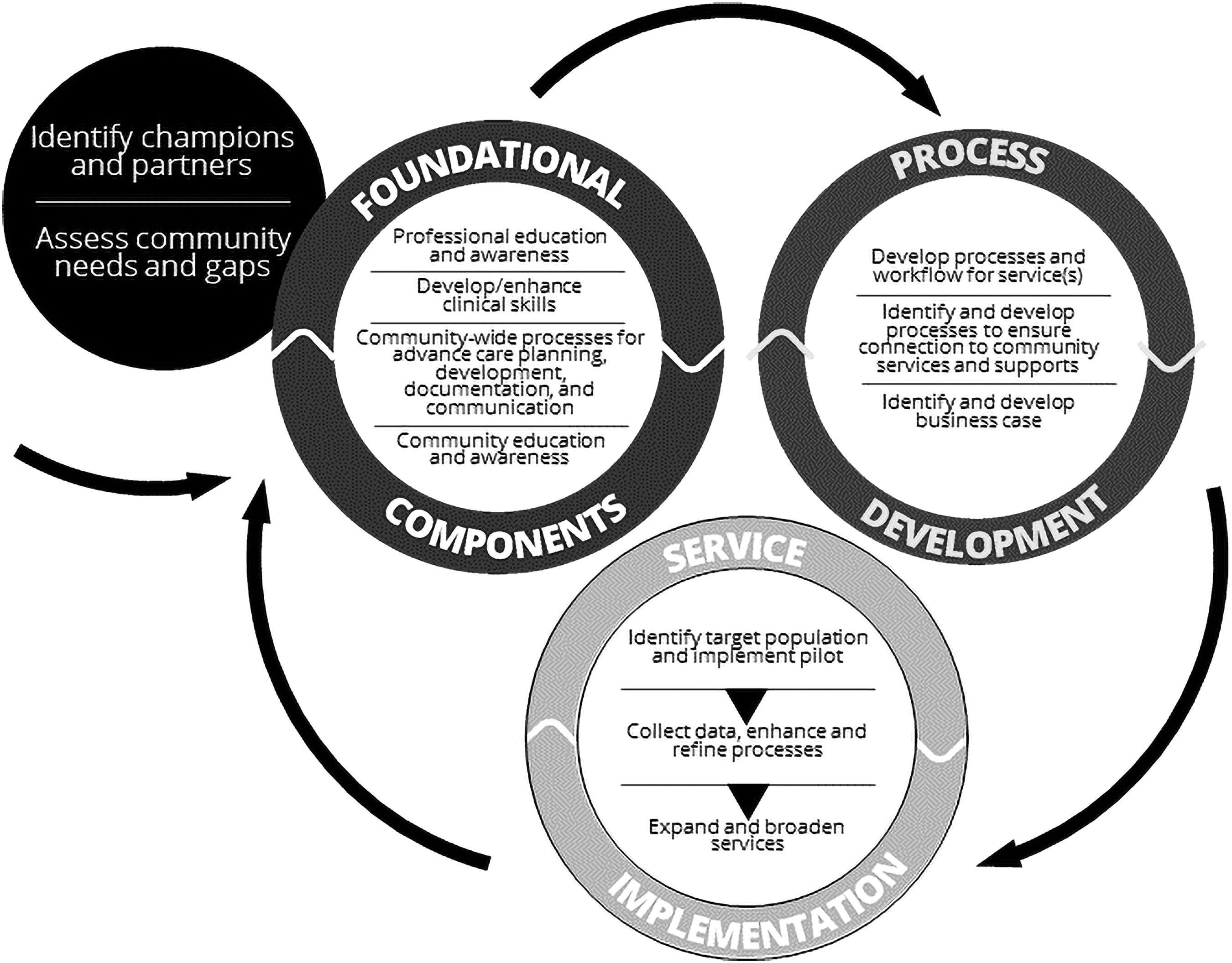
Conceptual framework for rural community-based palliative care service development. With permission from Weng et al. 62
The Learning Action Network (LAN) is one model that offers a peer culture to provide support as well as practical help.60,61 Members engage in round robin forums and exchange tools such as draft policies. The teams train together and participate in case consultations. A common measure set allows the teams to aggregate data to create more statistically significant measures of performance. An up-to-date roster is circulated so that members can reach out to other members. The LAN also uses a web portal to store common resources, upload measures, and engage in dialogue. An advisory team includes experts and all team leads.
A resource for rural PC services designed by Stratis Health uses a conceptual framework (see Fig. 4) that aligns with national standards and has a structured planning process for development. The planning process includes a strong emphasis on peer-to-peer exchange, such as a LAN. 62 Process development attends to design of workflows, processes to connect to community services and supports, and development of the business case. The last dimension focuses on service implementation. The above graphic (see Fig. 4) outlines this process in more detail.
Tip 10: Strengthening the Role of Nurses and APPs in Rural Areas Enhances Early Initiation and Access to PC
APPs (nurse practitioners, clinical specialists, and physician assistants) and nurses play an integral role in the delivery of PC and are increasingly filling the health care gaps due to physician shortages in rural areas. Integrating advanced nurse practice roles in PC has been successful in bringing better PC outcomes and improved satisfaction, particularly in rural areas.63,64
The advanced practice nurse roles are gradually becoming evident within PC, especially in rural communities where PC services are less accessible and more limited due to personnel shortages.36,65 Nurse-led PC services have helped patients to die at home peacefully, reduced frequent hospitalizations, and lowered hospital costs.66–68 There is less data on physician assistants, but their role has been growing in the field. 69 Whether as local PC champions or PC providers, APPs and nurses play a key role in expanding access to PC in rural areas.
Conclusion
Rural PC demands tailored strategies from providers to help bridge the gaps that exist in rural health care. PC providers can cultivate patient/family-centered care that respects cultural values, acknowledges socioeconomic factors, and addresses the barriers to accessing specialized services. As rural health care landscapes continue to evolve, it is crucial to remain proactive and open to innovation through collaborative efforts between health care organizations, policymakers, and local communities.
Respecting local culture, developing strong partnerships with the local community, utilizing and creating local resources, innovating in telehealth, expanding the role of APPs, and widening learning networks are some of the keys. Ultimately, the success of rural PC lies in the hands of dedicated providers who are committed to overcoming challenges and making a positive impact on the lives of patients and their families.