
Abstract
Background:
As a key component of advance care planning, serious illness conversations form a core intervention in palliative care. To achieve effective serious illness conversations, acknowledgment and inclusion of patient sense of self and identity are critical. However, no framework exists to describe how goals, values, and choices relate to patient identity. This conceptual gap hinders the advancement of palliative care education and practice.
Objective:
This philosophical investigation aimed to explicate two items: first, a novel conceptual framework for serious illness conversations; second, a structured approach to optimize these conversations within the palliative care clinical context.
Methods:
A philosophical and theoretical analysis was performed within an interdisciplinary context, by scholars in palliative care, medical humanities, philosophy, and bioethics. Key literature in psychology, qualitative research on the experience of serious illness, medical ethics, and choice architecture in medical decision-making were reviewed, and a structured conceptual and narrative analysis was performed.
Results:
An original and innovative identity-centered conceptual framework for serious illness conversations was developed. The framework consists of a four-step, reproducible approach: (1) attend to patient narrative identity, (2) identify values, (3) cocreate goals, and (4) actively promote choices. In short: attend, identify, create, and promote (AICP).
Discussion:
By using this conceptual framework and four-step approach, clinicians can accomplish goal-concordant serious illness care and build rich clinical relationships that foster trust and goodwill.
Key Message
Starting with narrative identity in serious illness conversations provides an opportunity to honor patients and promote goal concordant care.
Case Example
Dan, a 23-year-old young man with a history of relapsed leukemia, is over it. His posture and expression reinforce what he has already shared during his oncology clinic visit: he wishes he could be out driving his car, cooking, spending time with his girlfriend, anywhere other than tethered to an IV pole waiting for platelets. He is exhausted by bone pain and annoyed with the need for regular transfusions to keep his blood cell counts up. His mother, his oncologist, and his palliative care team look on apprehensively.
“You’ve had a hard road Dan, and we are all so disappointed that your cancer has relapsed,” Dan’s oncologist begins in a gentle tone. “We want to support you in whatever decision is right for you. Based on what we’ve told you about risks and benefits, do you think you’d like to proceed with a second bone marrow transplant?” The physician looks on earnestly, hoping to promote Dan’s autonomy in this difficult decision.
Dan sighs out in exasperation, dropping his head into his hands. “So you’re asking me to pick—do I want to suffer more, in exchange for a possible chance for cure, or do I want to go home and die?”
Introduction
In the face of advancing illness, questions about death and dying take on a new urgency. Time suddenly speeds up, as a narrow window emerges for patients to articulate their thoughts and preferences around end-of-life care. In these emotionally fraught situations, the implications of life and death decisions weigh heavy, impacting clear thinking and communication for both patients and clinicians.1,2
For clinicians, successful serious illness conversations require emotional sensitivity, tact, and a reliable strategy or framework. 3 To address these challenges, efforts have been made to advance education in health care communication.4–8 Yet despite these efforts, many clinicians still feel underprepared in initiating conversations around advance care planning. 9 With these barriers in place, there is risk for delaying and derailing difficult goals of care conversations, and thus missing a critical window. 10
Serious illness conversations frequently arise during periods of crisis—when decisions are pressing and a choice is required.11,12 In such cases, clinicians generally try to maximize patient autonomy by providing an overview of the clinical problem, presenting a limited menu of possible interventions, and asking patients to choose the most tolerable in an array of undesirable options.13,14 However, we contend that this creates an unnecessary and forced dilemma for patients. As an alternative, palliative care clinicians can first seek to understand a patient’s identity, values, and goals as contained within their personal narrative.
The palliative care community has broadly recognized that expertise and training are required to deliver goal-concordant care at the end of life. Over the past decades, many research dollars and policy initiatives have been devoted to advance care planning. Unfortunately, there has been little transformation in how critical medical decisions are made or communicated. 15 A more effective, philosophically robust, and humanistic framework is needed. 16
One recently proposed solution is to reimagine goal setting as an iterative process. In the model set forth by Palladino et al., clinicians are tasked with assessing a patient’s understanding of the illness, sharing information, then “[exploring] the patient’s goals, values, and priorities with open-ended questions,” before offering recommendations on next steps.17,18 This stepwise model can be repeated throughout the illness trajectory. An iterative conversational approach such as this avoids the pitfall of decision-making under pressure, and may even help to stave off decisional regret.19,20
Still, there is a crucial step missing from this paradigm: a recognition of and response to a patient’s identity. “Identity” is a philosophically complex concept that is often misunderstood or taken for granted in medical practice.21,22 This lack of conceptual scrutiny is especially problematic for palliative medicine, where a deep understanding of identity is essential for holistic and effective care. 23 When the primary focus of palliative care is on goals rather than identity, palliative clinicians can fail to understand a patient’s values, which may subsequently lead to a failure to secure and support goal-concordant care. 24 Furthermore, there is a lost opportunity to illuminate the person at the center of the decisions and to thereby honor a patient’s unique lived experience.
Human beings carefully fashion identities across lifetimes. However, illness and disease can disrupt those identities.25–27 An identity disruption may force an individual to confront their own mortality, perhaps for the first time. This disruption may result in a sense of diminished agency and threat to sense of self, which can lead to significant existential distress.21,28,29 By centering identity, palliative care clinicians can discover more about their patients’ values and become better equipped to both promote agency and fortify patients’ sense of self against distress and loss.22,30 A deliberative, identity-centered model—rather than one revolving around goals or choices—is therefore also ethically preferable, insofar as it is the approach that best supports shared decision-making, and thereby helps to avoid the poles of unbridled patient autonomy on one side and clinician paternalism on the other.31–35
To promote mutual narrative reflection before decision-making, we propose an innovative four-step identity-centered framework for serious illness conversations: (1) attend to patient narrative identity, (2) identify values, (3) cocreate goals, and (4) actively promote choices. In short: Attend, Identify, create, promote (AICP).
Importantly, the AICP framework is a conceptual framework. The aim of a conceptual framework is to provide understanding of a process or situation by delivering an “interpretative approach to social reality.” 36 A conceptual framework lays out the key factors, constructs, or variables that comprise a phenomenon and then outlines the relationships among them. 37 For our purposes, the phenomenon is “serious illness communication,” and the constructs are narrative identity, values, goals, and choices. Hence, unlike many excellent resources in palliative care, the AICP framework is not a communication guide, checklist, or training program that offers step-by-step guidance on what to do or say within discrete conversations nor is it a theoretical framework that endeavors to explain, predict, and generate empirical hypotheses.38–40 Rather, the AICP framework provides a conceptual map of human identity and the mode by which a patient’s identity is intrinsically linked, in a stepwise fashion, to their values, goals, and choices. This map will help clinicians orient themselves to where they are and where they ought to be, in the sweep of both particular time-bound conversations, as well as broad and evolving patient–clinician relationships.
Because the AICP framework is a conceptual framework, it is not designed to replace conversational roadmaps such as the Ariadne Lab Serious Illness Conversation Guide, VitalTalk’s PAUSE or REMAP, or David Wu and colleagues’ 3-Act Model.3,41–43 Rather, we designed it as a piece of scaffolding or meta-framework which can support, augment, and even clarify these more practical approaches and tools (Fig. 1).
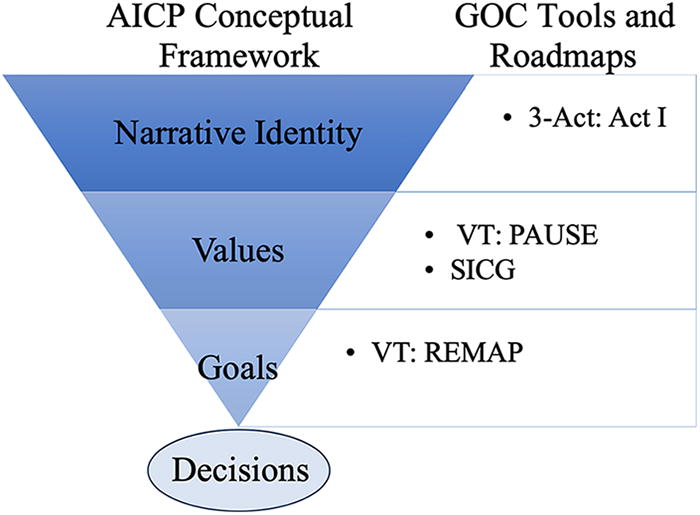
AICP framework stages and complimentary use of established communication tools. GOC, Goals of Care; 3-Act, 3-Act Model; VT, VitalTalk; SICG, Serious Illness Conversation Guide.
The AICP Four-Step Identity-Centered Framework
Step 1: Attend to narrative identity
Humans are storytelling beings. This means that unlike other animals, humans use stories or narratives to construct identity and to make sense of their own lives and the lives of others. The human mind is primed for narrative: it displays a built-in predisposition to “organize experience into a narrative form, into plot structures and the rest.” 44 This insight is the basis for the influential “narrative self” theory of identity wherein human consciousness provides an internalized, evolving story of the self, which supplies a sense of continuity and purpose to life. 45
In clinical medicine, it follows that at the center of every patient’s story sits a protagonist “Self” in process of construction. Importantly, a patient’s sense of self gets fashioned in sequence and in adherence to a plot. This means that when patients tell their stories, things rarely “just happen.” Instead, events (such as cancer recurrence) and decisions (such as hospice enrollment) are explained and justified in reference to larger-scale plots. These overarching narratives are often told in recognizable genres: tales of divine calling, victimhood, black comedy, spiritual testing, pointless tragedy, “coming of age,” or self-actualization. 46 Clinicians will benefit from learning both to recognize and navigate these narratives and to understand their relationship to a patient’s identity. Together, these skills encompass what has been termed “narrative competence.”
“Narrative competence” is the ability to absorb a story, decipher its meaning, and allow oneself to be moved by the narrative’s message to act on a patient’s behalf. 47 This is a process that can be taught and honed. 48 Conceptually, there are two facets inherent to this process, both of which bear on the pedagogy of narrative competence. These include (1) the creation of an environment conducive to receiving another person’s story and (2), the development of the necessary skills and virtues to effectively—and tactfully—receive, digest, and interpret the story.
Time constraints at the end of life and the vulnerability inherent in serious illness conversations present distinct challenges to creating a conducive environment for sharing in stories. Yet, providing a space of trust for honest sharing is a critical component of truly understanding a patient’s identity. This “space” contains both physical and emotional dimensions. First, it requires a true physical structure, a location containing necessary support people, arranged with care in order to promote clinical attention.49–51 Second, narrative conversations about identity require a safe emotional space for patients to inhabit. The structure of an emotional safe space is variegated. One important aspect of a safe emotional space is the presence of a trauma-informed care philosophy, since in the process of storytelling, past traumas are frequently revealed. Providing interdisciplinary trauma-informed care is an optimal means of facilitating serious illness conversations, as well as the palliative standard of care. 52
Next, the narrative must be actively absorbed and metabolized. This too requires attention (i.e., attending to) as well as generous listening. To listen generously entails taking in what is told verbally, as well as attending to nonverbal cues. 53 Gestures and expressions hold meaning, as do silences, including the gaps and absences in storytelling. 54 Absorbing a narrative also demands curiosity and humility, both considered virtues of clinical practice.55,56 Regarding curiosity, where ambiguity or confusion exists, palliative clinicians should use exploratory statements to gain clarity and concreteness, rather than filling in gaps with canned assumptions or by imposing psychoanalytic jargon (e.g., she is probably just “practicing avoidance” or he is just “projecting” onto the team). Importantly, palliative clinicians can acquire training in the practice of cultural humility, in order to reduce the impact of cognitive bias and to improve their ability to clarify and coconstruct the content of a patient’s narrative.57–59 . From the broader didactic perspective, it is notable and exciting that many of the narrative processes and competencies mentioned above are expanding across palliative care education in the form of the 3-Act model.60–62
When patient voices are not accessible, owing to developmental stage, differences in ability, illness severity, or other reasons, caregiver perspective becomes even more critical. In palliative care, we are accustomed to asking, “what would your loved one say, were they to be able to speak now?” As an alternative, we would consider rephrasing to emphasize narrative, by first asking, “tell us about your loved one’s life?” or even, “can you tell us the story of your loved one’s life?” This method of life review by caregivers is not banal and provides a critical window into a patient’s values (and may serve as an important therapeutic endeavor for the caregiver as well). 63 It also allows an additional opportunity for the clinician and the caregiver to honor the patient whose voice is not actively present.
Step 2: Identify values
Once a patient’s narrative begins to flow, their values can be discovered like rocks shaping the current of a stream. Values sit at the joints of narratives, helping to direct stories one way or the other. In relaying narratives, individuals put their values on display—for example, when sharing how they have made “judgment calls” about what is moral or immoral, praiseworthy or vile. Values may be stated directly or they can be revealed by listening carefully to how patients choose to actually live their lives, similar to the concept of “revealed preferences”' in economics. 64
Values can be conceptualized as “priorities, internal compasses or springboards for action”—as kinds of “moral imperatives.” 65 Values are arranged hierarchically and differ from person to person and within cultures. 66 Values are intimately connected to community norms (e.g., around what defines “the truth” or “appropriate behavior”), and values often condition beliefs, such as “this is just what good parents do.”67,68 Practically speaking, values orient and direct activities in accordance with personal or communal desires. In so doing, values serve as a compass, telling people how to structure their goals and ultimately how to act.
Values typically share a congruence with narrative, goals, and decisions. For example, if a patient with ALS says they want to “die naturally” whenever “God calls me home,” but then requests a gastrostomy tube and tracheostomy, this warrants a dialogue to better understand what at first blush appears to be a decision at odds with stated values. Does the patient value control and self-determination more than they are willing to admit? Do they live with the guilt of leaving a loved one behind? Has their identity changed significantly with the stressors of illness? Because values emerge directly from a person’s story, they generally ought to align with it, unless there is a clear reason for departure. It is the palliative clinician’s responsibility to, when appropriate, gingerly guide patients back to their own narrative core, in order to facilitate a retelling of that same narrative when and if a retelling is necessary.
Step 3: Cocreate goals
A goal is more specific than a value. 69 Whereas values concern abstract concepts, like freedom, progress, or safety, a goal represents a desirable and targeted outcome. Goals can be clearly and rationally pursued; people “set goals” but do not “set values.” 70
Within serious illness conversations, goals do not flow as freely as narrative or reveal themselves as clearly as values. It is up to the clinician to help cocreate goals within the framework of what is realistically possible, given ethical standards and the medical facts.71–73 It is likely, and should be anticipated, that a patient may conceive of goals outside of what is medically available. These goals should not be dismissed. A clinician can acknowledge the hopes, reframe them as beyond the expected borders of what is medically feasible at this moment, and encourage exploration of additional goals.
For example, consider a 91-year-old patient and a 38-year-old patient both faced with a progressive and life-limiting diagnosis. Both value family. For the 91-year-old, valuing family may manifest in the goal of witnessing the upcoming birth of a great grandchild. Conversely, for the 38-year-old, valuing family may lead to the goal of cultivating a spousal partnership and bodily integrity to share physical intimacy. For the two individuals with similar stated values, decision-making regarding medical interventions may diverge significantly based on individualized goals in the context of those values.
Step 4: Promote choices
Once value-informed goals are clarified, goal-directed decisions can emerge. When clinicians understand who the patient is, what they value, and why, it becomes easier to promote an informed, patient-centered plan.
Although it is crucial that patients understand their illness and their options, we recommend waiting until Step 4 to delve into the particulars of each intervention. Once goals are cocreated within the boundaries of what is possible given the medical facts of the case, then clinicians may inject expertise including pros and cons of each intervention to allow for fully informed decision-making. Importantly, there are published tools that can be used at this point in the decision-making process. For example, the use of “Best Case/Worst Case” approach to weighing treatment options can be incorporated here, in order to maximize shared decision-making.74–76
Starting with choices places the onus completely on the patient. However, by allowing the patient to first share their story, then reflect, and finally hear provider input, there is greater emphasis on a shared decision—which can only occur in the context of an actual back and forth conversation. The patient and clinician can then become true deliberative partners, and thereby prevent the patient from shouldering the burden of illness and decision-making alone. 77
A metaphor is illustrative. The relationship among narrative identity, values, goals, and decisions can be pictured as a set of Matryoshka dolls (Figure 2). Matryoshka is a wooden doll that separates at the middle to reveal a smaller figure inside. The smaller figure also pulls apart to disclose an even smaller doll within. The pattern repeats until the tiniest doll is found at the center. Analogously, a patient’s narrative can be understood as “containing” values, with values containing goals, and goals containing discrete choices. Crucially, like a set of Matryoshka dolls, a clinician cannot get to a patient’s authentic choices and then support them in making a decision from among those choices, if they do not first travel through the patient’s narrative, values, and goals. To attempt to do so risks trauma and coercion and, in our experience, increases the likelihood that a patient will have decisional regret or change their mind in the future.

Matryoshka dolls.
Discussion
Whether intending it or not, clinicians act as choice architects, exerting significant power and influence over decision-making processes. 78 However, by using the stepwise narrative approach outlined above, clinicians will be better equipped to practice a transparent and patient-centric version of shared decision-making. We have found that this approach enhances ethical medical care, insofar as it can limit clinical paternalism, promote patients’ authentic choices, and curb the infusion of bias into serious illness conversations.
At the heart of this procedure is the identity of the patient, an identity that gets fostered and fortified through relationship and care. By cultivating a relational approach, palliative clinicians work to establish trust and build connection, processes that can lead to stronger patient–clinician relationships and a higher quality of care.79–81 This becomes clear when considering our patient Dan again, this time hypothetically through the four-step identity-centered framework.
Attend: Approaching Dan to make a decision without starting with his narrative resulted in overburdening and frustration. Instead, let us say we return to Dan and encourage him to tell his story. As the platelets are finishing, we ask “tell us about yourself?” With a little prompting, we learn about Dan’s trajectory from a childhood athlete to an adult who loves his “team” of friends and family and the freedom afforded in running and driving fast.
Identify: We hear about his passion for cooking, and give him space to share excitement around a new romantic relationship. Values such as independence, interpersonal connection, and enjoying life’s pleasures emerge.
Create: From there, we cocreate goals with Dan, including sharing more time with his family and partner, preserving autonomy in self-care, retaining the sense of taste to enjoy food, and maintaining his clarity to drive, arranged hierarchically in that order.
Promote: In promoting choice, we discuss medical interventions available, including bone marrow transplant, palliative chemotherapy, and hospice care. We reflect back what we heard from Dan in the conversation, and ask for permission to make a recommendation. Dan ultimately choses to pursue a second transplant, after coming to realize that this fits with his goal for more time with loved ones.
In summary, within this proposed conceptual framework, clinicians meet patients right where they are in their serious illness trajectory. There is no sacrifice of autonomy or self-determination; rather, this proposed narrative-based four-step identify-centered framework promotes digging deeper to uncover the unique needs of each individual in order to provide personalized planning. When applied with generous listening and humble curiosity, the patient and clinician can become a dynamic team. In starting with narrative, we honor the humanity of the person suffering from an illness and allow a patient’s story to authentically guide decisions. We believe that this humanistic mode of interpersonal communication lies at the heart of practicing goal-concordant and ethical palliative care.
Footnotes
Authors’ Contributions
All authors approved the final version as submitted and agreed to be accountable for all aspects of the work. Of note, “Dan” represents an amalgamation of two young adult patients cared for by authors N.L., S.T., and T.T. Name and other identifying factors have been removed or significantly changed for confidentiality.
Authors Disclosure Statement
N.L., S.T., J.W., M.W., and T.T. conceptualized the article, drafted the initial article, and reviewed and revised the article.
Conflict of Interest: Dr. Webb receives research funding from the Patient-Centered Outcomes Research Institute (PCORI), and honoraria from the American Academy of Hospice and Palliative Medicine. Dr. Tate receives research funding from the Greenwall Foundation Faculty Scholars Program.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.