
Abstract
In this report, we present the case of an older adult with severe obesity and multiple comorbidities, including heart failure with preserved ejection fraction (HFpEF), who experienced a prolonged decline complicated by recurrent hospitalizations and skilled nursing facility stays during the two years preceding death. This case highlights challenges in prognostication attributed to severe obesity complicated by HFpEF, which likely delayed goals of care conversations, and access to palliative care and hospice, despite high symptom burden. We discuss prognostic uncertainty among those with severe obesity and outline potential future directions.
Introduction
Obesity affects almost half of those age 60 and older in the United States, with severe obesity (body mass index [BMI] ≥35 kg/m2) predicted to become the most common type of obesity by 2030. 1 Recent studies have shown that severe obesity is increasingly prevalent during the last two years of life among older adults. 2 In addition, obesity affects populations where there are long-standing health care equity concerns associated with race/ethnicity, gender, sexual identity, and socioeconomic status. 3
Older adults with severe obesity have high rates of multimorbidity, including diabetes, heart failure with preserved ejection fraction (HFpEF), chronic obstructive pulmonary disease (COPD), and renal failure, along with an increased risk for hospitalization. 4 Studies have shown that adults with severe obesity experienced high in-hospital mortality during the COVID-19 pandemic.5,6 Currently, hospice utilization is low among individuals with severe obesity, with one study indicating adults with severe obesity were 40% less likely to enroll in hospice than nonobese adults and had shorter average durations of hospice enrollment. 7
Especially challenging is the common coexistence of severe obesity and HFpEF in older adults, often associated with a high burden of multimorbidity, functional impairment, recurrent hospitalization, and mortality. 8 HFpEF is distinct physiologically, and more strongly associated with obesity, than heart failure with reduced EF (HFrEF), which is better studied regarding evidence-based treatment, prognosis, and palliative needs at the end of life (EOL). Symptom burden and palliative needs in HFpEF are often attributed to multiple comorbidities and may be underrecognized. 9 With the rising prevalence of comorbid HFpEF and severe obesity, there is a critical need for timely palliative care (PC) initiation to address symptom burden, caregiver needs, and EOL transitions.
Case Description
A 72-year-old female patient (RL) with past medical history of severe obesity (BMI 47 kg/m2), HFpEF, atrial fibrillation, COPD, asthma, polymyalgia rheumatica, recurrent urinary tract infections, chronic kidney disease (CKD) stage III, and vertical banded gastroplasty complicated by stenosis and gastric outlet obstruction presented to the emergency department (ED) with dyspnea at rest, severe fatigue, and bilateral lower extremity edema. This admission was six months before her death at home (Fig. 1).
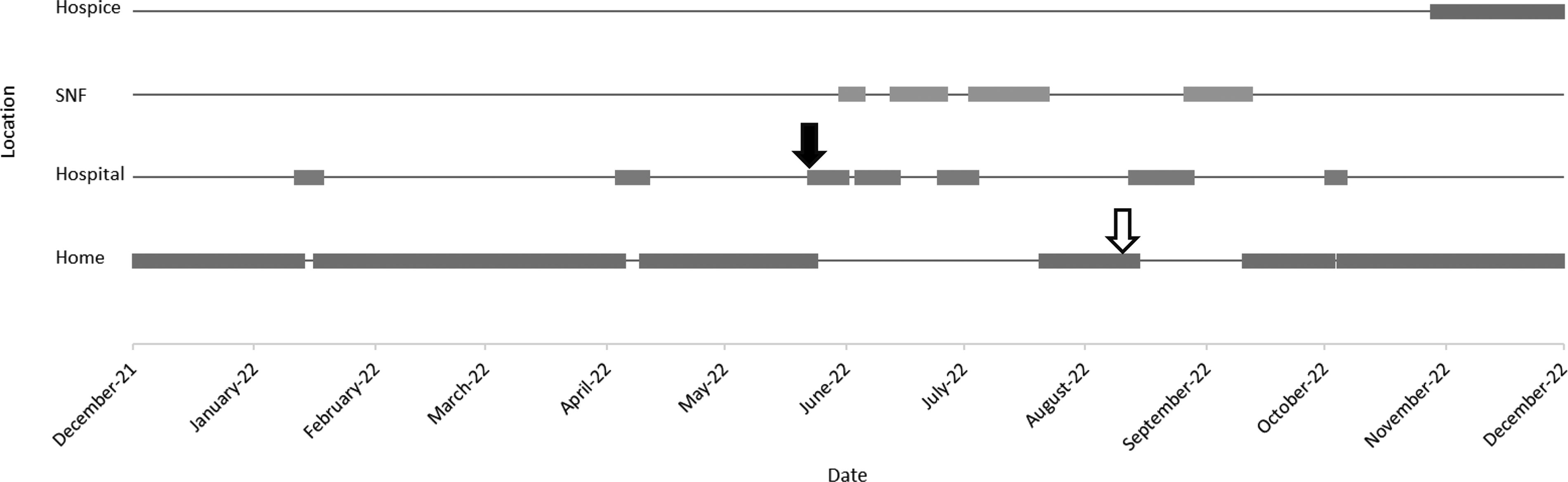
Care setting during last 12 months of life. The solid arrow indicates the index hospital admission, and the hollow arrow indicates initiation of home-based palliative care.
Background
Despite following with the heart failure clinic for the past two years, RL’s outpatient heart failure management was challenged by a combination of social and medical factors. Transportation barriers necessitated that she was predominantly seen virtually. Heart failure telemonitoring was limited, initially because of a lack of a functional scale at home and later because of physical limitations impairing her ability to stand on the scale. Diuresis was limited by acute kidney injury and hyperkalemia. Her steroid dependence (for asthma and polymyalgia rheumatica) with inability to taper steroids because of worsening pain and secondary adrenal insufficiency further exacerbated fluid retention. She experienced respiratory symptoms requiring nocturnal oxygen, which complicated her clinical picture, in the context of known asthma and likely undiagnosed obstructive sleep apnea. Our patient had 13 hospital admissions in the preceding two years, during which time she had experienced significant functional decline; she could ambulate only a few steps to the commode and was now dependent on her grandson for activities of daily living. She had minimal improvement in functional status despite four skilled nursing facility (SNF) stays for post-acute rehabilitation (PAR) in the previous two years. The inpatient PC team was consulted during an admission one year prior when her palliative performance scale (PPS) was 30%. At that time, RL’s goals of care (GOC) were to improve function and independence. Further goals of care discussions were strongly recommended by the PC consultant if there was concern that she would not meet her functional goals. Outpatient PC referral was not pursued by her cardiology team, and PC was documented to be discussed during only one subsequent hospitalization, during which RL declined inpatient consultation owing to the belief that PC is for “patients who are dying.”
Hospital/Post-acute course
RL was admitted to the cardiology team during this admission and received IV diuresis. Owing to her poor functional status, PAR was recommended, but the patient declined as she had not noticed benefit from prior SNF admissions. PC was not discussed; she was then discharged home. She returned to the ED one day after discharge following a fall, suffering an ankle avulsion fracture that was treated nonoperatively, and discharged to SNF. RL was rehospitalized twice in the following month from SNF with Clostridium difficile colitis and aspiration pneumonitis. She was discharged from SNF two months after her initial admission to move in with her granddaughter. Despite over four weeks of PAR therapies, she could only ambulate minimally to the commode with her walker.
Subsequent care transitions
Approximately two weeks after her return home, she established care with home-based PC for management of uncontrolled pain.
During her initial visit with home-based PC, GOC were discussed with RL and her granddaughter, who reported noticing decreased benefit from hospital admissions and PAR therapies. She noticed increased fatigue and had lost ∼5–10 pounds in the previous six months. She had New York Heart Association (NYHA) Class III symptoms and severe back pain, limiting her ability to participate in therapy. RL reported feeling that doctors had been ignoring her pain, having prescribed only acetaminophen. She was prescribed hydrocodone/acetaminophen 5–325 mg for breakthrough pain. She elected a DNAR code status and completed an MI-POST form reflecting her treatment preferences. She was deemed not eligible for hospice at this point, but end-stage heart failure symptoms were discussed; the PC team anticipated hospice transition within the year.
Over the next month, she had two more hospital admissions with multifactorial respiratory failure attributed to COPD, congestive heart failure, obesity hypoventilation, and aspiration pneumonia. She was discharged to SNF for two weeks of PAR and returned home on continuous oxygen. She could pivot to commode but could not walk more than a few steps and had developed a sacral pressure ulcer. She then had an aspiration event while swallowing pills and returned to the ED with shortness of breath and inability to tolerate solid foods. She was recommended to follow a lifelong strict puree diet. She was discharged home to resume home care and home PC and was referred to a house calls program.
The patient elected to transition to hospice two weeks later during an encounter with the home PC nurse practitioner. She reported whole-body pain not relieved by hydrocodone/acetaminophen. Bedbound since hospital discharge because of fear of falling and deconditioning, she reported poor oral intake with inability to follow a puree diet. The certificate of terminal illness by her PCP noted that her multiple chronic medical issues and recurrent admissions portend a poor prognosis of less than six months.
She was enrolled in hospice for 32 days before her death at home.
Discussion
We present the case of an older adult with severe obesity, who experienced challenges with outpatient heart failure management, recurrent hospital readmissions, and multiple rounds of PAR therapies with progressively less benefit. She suffered uncontrolled symptoms because of heart failure and other comorbidities in the last two years of life. She was referred for PC services three months before her death at home, which led to improved symptom management and communication regarding GOC, and later hospice enrollment 32 days before her death.
We suspect that owing to her obesity-related comorbidities and functional impairment, prognostication was challenging, which likely delayed referral to PC. From a cardiac perspective, it was challenging to classify her heart failure as end stage as she had NYHA Class II–III symptoms when optimized, with physical activity limited more by mobility than by dyspnea, and did not require oxygen during the day until the last three months of her life. In addition, although she was hospitalized frequently, only a fraction (four of seven admissions in the last year of life) were due to heart failure. However, from a broader perspective, RL had multiple poor prognostic indicators during her last six months of life, the most significant of which was recurrent hospitalization. A secondary analysis of the treatment of preserved cardiac function heart failure with an aldosterone antagonist (TOPCAT) trial of HFpEF patients demonstrated increased mortality with recurrent hospitalizations, regardless of whether hospitalizations were for cardiac or noncardiac causes. 10 She additionally had recurrent PAR without significant functional improvement. There has been increasing recognition recently regarding the phenomenon of being “rehabbed to death”—the increasing number of patients who spend the last months of life cycling between rehabilitation facilities and hospital.11,12 Older and frail adults are less likely to benefit from rehabilitation and have fewer days at home following discharge. 13 She additionally had weight loss in the last six months of life, another poor prognostic indicator. Health care providers are trained to recognize underweight status, cachexia, and weight loss, but recognition of weight loss among older adults with severe obesity remains a challenge despite weight loss in older adults being similarly correlated with mortality across all baseline weights. 14
Earlier referral could have enabled better management of dyspnea and chronic pain, with concurrent care focused on disease management. Patients with obesity have a high prevalence of undertreated chronic pain leading to pain-related functional impairment, limiting therapy participation, and impacting quality of life. 15 Although PC referral helped the patient clarify her GOC and ultimately led to hospice admission, the patient was referred to hospice late in her disease trajectory (32 days before death), shorter than the average number of hospice days (104) for patients with cardiac/circulatory conditions. 16 Earlier hospice referral may have provided the patient and family with more support, enabling her to spend more days at home in the last six months of her life. She spent only 100 days at home in the last 180 days of life (32 of which were after hospice referral), limiting her healthy days at home, a recently established quality measure for care at EOL. 17
Prognosis in advanced heart failure is well known to be challenging; patients with heart failure often experience intermittent exacerbations, each possibly fatal, with interval improvement close to their premorbid baseline. 18 In patients with HFpEF and severe obesity, there is higher risk of readmission and death from noncardiac causes, which may further obscure terminal decline. 19 The relationship between obesity and survival in heart failure is complex. In HFrEF, there is evidence that obesity may actually be a protective factor; however, the largest randomized controlled trial of patients with HFpEF, the Irbesartan in Heart Failure with Preserved Ejection Fraction trial, demonstrated adverse cardiovascular outcomes in both lower BMI <23.5 kg/m2 and higher BMI >35.20,21
Commonly used heart failure and palliative prognostic tools fall short in assessing prognosis in patients with severe obesity. In addition to being less well-studied in HFpEF, few heart failure prognostic models incorporate BMI and none account for functional or social factors (e.g., physical and social limitation scores, quality of life), which correlate highly with mortality in HFpEF/severe obesity in newly developed machine learning models.22–24
Two commonly used prognostic calculators by PC providers are ePrognosis using Walter one-year mortality and the PPS-Hospitalized.25,26 These were developed before 2010 when severe obesity prevalence was significantly below current levels, although ePrognosis is updated regularly. Although functional status, albumin, and creatinine are factored in the calculation of the Walter one-year mortality, older patients with severe obesity in the latter years of life have extended periods (many years) of poor functional status because of obesity-related sarcopenia and musculoskeletal impairments, elevated creatinine because of high prevalence of CKD, and lower albumin because of chronic malnutrition. This potentially reduces the prognostic sensitivity of this calculator. Similarly, three domains (ambulation, daily level of physical activity, and self-care assistance) in the PPS focusing on functional status are chronically affected in the severely obese population, leading to early-onset disability before approaching EOL. This reduces the sensitivity of PPS scales to predict decline and referral to hospice. Absolute score may have limited practical utility in prognosis for this population, demonstrated by a patient’s PPS at 30% over a year before her death, a score that in one systematic review was estimated to correlate with survival of 5–36 days in the broader palliative population. 26 Monitoring for decline in PPS is much more helpful as functional decline is correlated with all-cause mortality. 27
Prognostication is key to ensuring timely referral to hospice care. Patients with severe obesity often face death 14–15 years earlier than the normal-weight individuals, yet mortality prediction by health care providers among this obesity class is a challenge. This is exemplified in our patient RL, who did not meet hospice criteria based on heart failure alone, yet her comorbidities, repeated hospitalizations, and poor functional status portended a poor prognosis.
This case illustrates that to provide equitable EOL care to this vulnerable population, more work is needed to develop new prognostic tools and frameworks applicable to older adults with obesity and HFpEF, whereas ongoing research is needed to validate current prognostic tools in this population. In the meantime, an inclusive approach to assessing prognosis and hospice eligibility in patients with obesity and HFpEF is needed, which accounts for medical comorbidities, changes in functional status, and impaired quality of life.
Footnotes
Author Disclosure Statement
C.V. is a board member of the American Geriatrics Society Board of Directors. Otherwise, the authors declare that there is no conflict of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.