
Abstract
Background:
Patients in palliative care are often treated with antithrombotics, even in the late stages of disease. Clear guidelines regarding deprescribing are lacking.
Objective:
The aims of this study were to investigate bleeding as a side effect of antithrombotic treatments the last year in life and map the timing of deprescribing.
Methods:
A retrospective cohort study was performed. All medical records were screened for deceased patients admitted to a palliative care unit in Stockholm, Sweden, over a 3-year period. Patients with antithrombotics were identified; data on bleeding, and on side effects due to deprescribing, were extracted from the medical records. Log-binomial models were used to explore factors associated with bleeding.
Results:
Of 1501 patients, 897 were treated with antithrombotics during the last year of life (mean age 75 years, 41% women). Of these, 56% continued treatment up until the last 3 days of life. Of the 897 patients, 144 (16%) had at least one bleeding during the treatment. The risk for bleeding was significantly higher for men with prostate cancer compared to other cancer forms, adjusted relative risk 1.9 (95% CI 1.1–3.2). No difference in risk for bleeding was found between sex, age groups, type of antithrombotics, or indication. Two patients (0.2%) developed strokes after antithrombotics were deprescribed.
Conclusions:
Treatment with antithrombotics during the last year of life is associated with a high risk of bleeding. In this cohort, men with prostate cancer seemed to have more side effects of bleeding than other groups. Few experienced side effects from deprescribing.
Introduction
Antithrombotic treatments are often prescribed in specialized palliative care units,1–5 since patients with cancer or chronic cardiovascular diseases (e.g., atrial fibrillation and stroke) often benefit from this treatment, regardless of adverse effects.1,6 Antithrombotic treatments include antiplatelet drugs (aspirin, clopidogrel, and glycoprotein IIb/IIIa receptor antagonists) and anticoagulants (unfractionated and low-molecular weight heparin, warfarin, and direct oral anticoagulants [DOACs]). 7 Clinical guidelines suggest that many patients with thrombosis and cancer, with atrial fibrillation, or after a stroke would benefit from lifelong prophylactic treatment with antithrombotics. It is, therefore, common for some patients to have used antithrombotics for an extended duration before being admitted to specialized palliative care.
In Sweden, over one million citizens were treated with antithrombotics in 2022, which is approximately 10% of the population. 8 The international use of antithrombotic therapy among patients in specialized palliative care varies from 7% to 60%, according to previous studies performed in the United States, Austria, and United Kingdom.1,9–11 In a study from 2017, Kowalewska et al. reported that 7% of the patients admitted to a hospice in Oregon, United States, were using antithrombotics. 1 Arevalo et al., from The Netherlands, also reported a significant difference in the use of antithrombotics during the last week of life between patients who died in a hospice-care ward (27.1%), at home (45.9%), and in hospital (72.9%). 12
The adverse effects of antithrombotics are primarily bleeding, with varying degrees of severity such as bruises, nasal bleeding, gastrointestinal bleeding, hemoptysis, hematuria, or intracranial bleeding.13,14 Previous studies have shown that the prevalence of bleeding among patients treated with antithrombotics is about 10%.15,16 In the late palliative stage, i.e., the last weeks and days of life, the care should be focused primarily on quality of life and symptom control 17 ; at this stage, the potential adverse effects of many medications outweigh their benefits. 17 It is essential to weigh the risks related to discontinuation of antithrombotics (e.g., the risk of suffering from lung emboli or stroke), which could significantly impact symptom burden against the risk of severe bleeding. 15 Although the benefits and safety of using antithrombotic therapy at the end of life are unclear, there is no clinical guideline indicating when antithrombotics should be deprescribed in palliative care to avoid potential adverse effects.18,19
The primary aim of this study was to investigate bleeding as an adverse effect of antithrombotic use and the associated risk factors during the last year of life in patients admitted to a palliative care unit. Secondary aims were to study the side effects from deprescribing and map the timing of deprescribing antithrombotic treatment in the study cohort.
Methods
Study design
This is a retrospective single-center cohort study. A retrospective review of medical records was performed for all deceased patients who had been admitted to a specialized palliative care unit in Stockholm, Sweden, “ASIH Stockholm Södra,” 20 from January 1, 2016, until December 31, 2018.
The study was approved by the Swedish Ethical Review Board, Dnr 2018/1798-31. No informed consent was obtained since all patients included were deceased at the time of the retrospective review.
Study setting
The “ASIH Stockholm Södra” unit provides specialized home care and in-patient specialized palliative care. All the teams in the unit are staffed by trained specialists in palliative medicine and physicians in training. In the specialized home care, 80% of patients have malignancies and 20% nonmalignant diseases. The patients are at different stages of their diseases and in need of supportive or palliative care. The in-patient ward has 16 beds for patients in late palliative stages and end-of-life care, where the focus of the care is on comfort and symptom control. The unit enrolls patients from the south-eastern part of Stockholm, mostly covering low- and middle-income areas, with approximately 800 000 inhabitants. The average duration of care is 4 months for the specialized home care and 1–2 weeks for the specialized palliative ward. When patients are admitted for specialized palliative care, the unit has the overall responsibility for the patients, so they do not have contact with their general practitioner during this time. If the patients have other medical contacts, these are with specialist care departments at the hospital. The medical regimens are reviewed with the patients and, apart from antitumoral treatments, all prescriptions are made by the specialized palliative care doctors. Antitumoral treatments, given for both palliation or with curative intention, are always prescribed and deprescribed by oncologists at the oncology clinics in the hospital. In specialized home care, a visit is made to the patient at least every week for the assessment and control of symptoms. At this visit, the patients’ medical regimens are reviewed, and they receive their medication for the coming week. In the specialized palliative ward, a review and assessment is held with the patient every day. Blood tests or INR are taken as necessary and not on a regular basis. The unit is described in detail elsewhere. 21
Participants
All patients deceased between January 1, 2016, and December 31, 2018, at the palliative care unit (specialized home care and specialized palliative ward) were included in the study and screened for the use of antithrombotics (ATC code B01) during the last year of life. Patients with short-term (4 weeks) prophylactic antithrombotic treatment after surgery were excluded to maintain a homogenous study population.
Variables
All variables were extracted from the medical records. For all patients who had been prescribed antithrombotics, the following data were extracted: Type of medication (Supplementary Table S1), indication for and dose of antithrombotics, date and reason for deprescribing, complications after deprescribing (e.g., thrombosis, strokes), bleeding during antithrombotic use, and date and type of bleeding. Demographic and clinical data, including date of birth and death, sex, form of care (specialized home care or specialized palliative ward), primary diagnosis, and cause of death were also collected.
All medical records were reviewed by a senior consultant at the unit, who is specialized in oncology and palliative medicine.
Statistical methods
Descriptive statistics are presented as n (number) and percentage (%). Chi-square test was used for the comparison between patients with cancer and the noncancer group. The log-binomial generalized linear models were used to explore mutually adjusted factors associated with bleeding compared to no bleeding. The estimates from the unadjusted and adjusted models are presented. The adjusted model included the following factors potentially related to bleeding: Sex, age, primary diagnosis, indication, and type of antithrombotic treatment. All these factors were identified a priori based on subject matter knowledge.
All analyses were performed with R version 4.3.1.
Results
Participants
All 1501 patients admitted to the unit and deceased from 2016 to 2018 were screened for antithrombotics (ATCcode B01). Patients who had never used antithrombotics or used them for less than 4 weeks after surgery were excluded (n = 551). This resulted in a total of 950 patients, who had been treated with antithrombotics for more than 4 weeks. Since we wanted to study treatment and deprescription during the last year of life, another 53 patients who received treatment with antithrombotics before the last year of life were also excluded (n = 53). The remaining 897 patients treated with antithrombotics during the last year of life comprised the study population (Fig. 1).
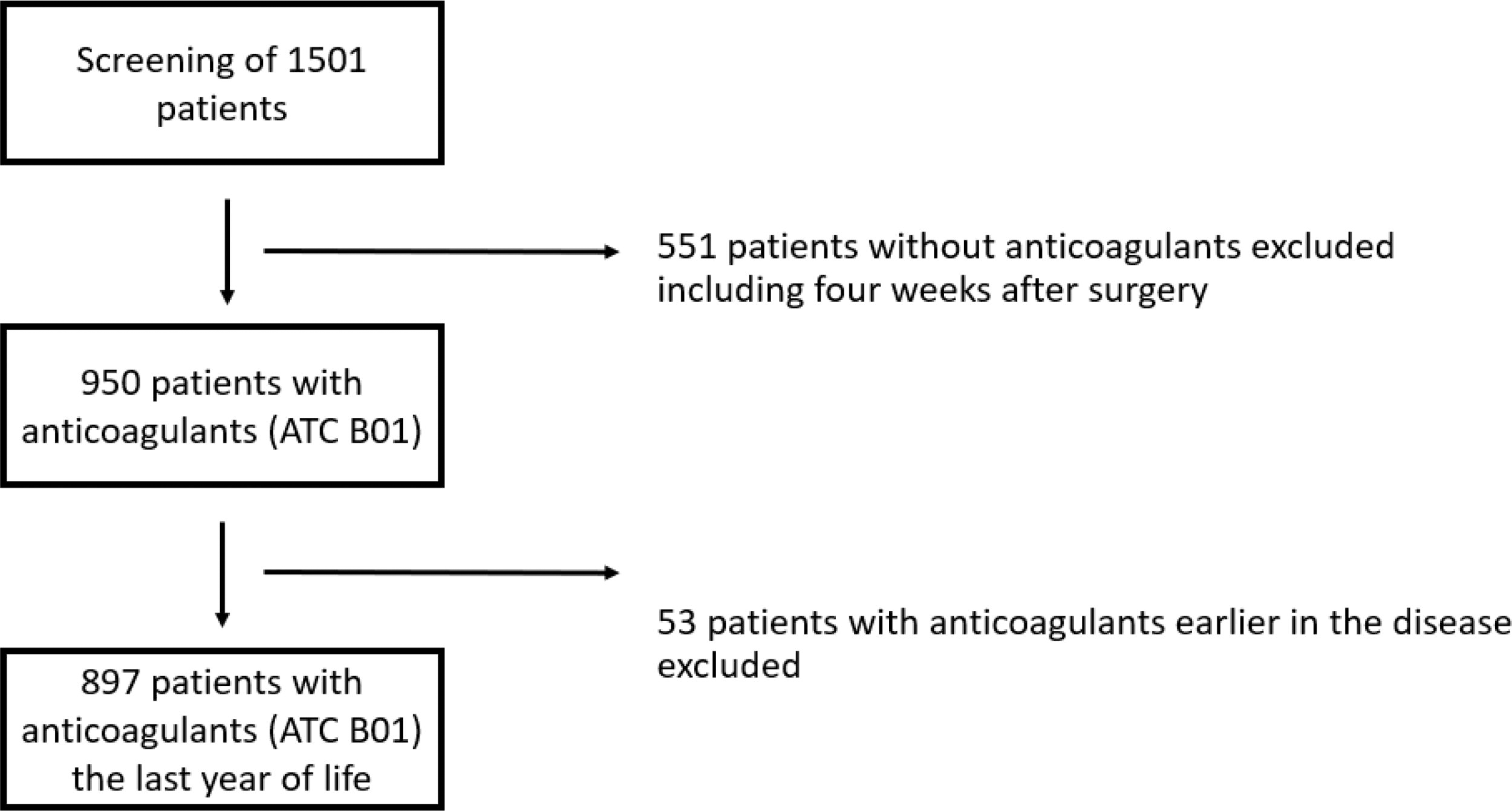
Flow chart of inclusion of patients from a specialized palliative care unit in Stockholm, Sweden, who died between 2016 and 2018.
The majority was men (58.4%), the mean age at death was 75 years, and cancer was the most common primary diagnosis (76%) (Table 1). When admitted to the clinic, most patients received specialized home care (73%) and the remaining 27% received care in the specialized palliative ward.
Characteristics of 897 Palliative Patients Using Antithrombotics in the Last Year of Life
Statistical analysis was performed using Chi-square test and p < 0.05 was considered statistically significance of bold.
Other per oral (warfarin, dabigatran etexilate, and direct oral anticoagulants [DOAKs]).
CNS, Central Nervous System; LMWH, Low-molecular weight heparin.
The majority of the study cohort was patients with cancer (76%). Patients with cancer were treated with low-molecular weight heparin (LMWH) to a higher extent compared to those with no cancer, 36% compared to 11% (p < 0.001). Thrombosis and myocardial infarction were the most common indications in the cancer group, compared to atrial fibrillation in the noncancer group.
Bleeding
Among the 897 patients using antithrombotics in the last year of life, 144 (16.1%) experienced bleeding of some kind. The occurrence of bleeding was similar between patients with cancer and the noncancer group, 15.6% compared to 17.5% (p = 0.45). The most common sources of bleeding were from the gastrointestinal tract, hematuria, nasal bleeding, tumor bleeding, or bleeding from the skin. Fourteen patients (9.7%) had bleeding from the central nervous system (CNS). The occurrence of CNS bleeding in patients with cancer was significantly lower than in those with a noncancer diagnosis, 6.6% compared to 18.4% (p = 0.02), see Table 1.
Risk factors for bleeding
Relative estimates of risk factors associated with bleeding were calculated. No increased risk was found in relation to age, sex, or indication for antithrombotics. Regarding primary diagnosis, there was an increased risk of bleeding in men with prostate cancer, RR 1.9 (95% CI 1.11-3.2), in the model adjusted for sex, age, primary diagnosis, and indication for and type of antithrombotic treatment compared to those with a noncancer diagnosis (Table 2, Fig. 2). No patient with gynecological cancer (n = 30) suffered from bleeding. There was also an increased risk of bleeding in the group receiving other oral (warfarin, dabigatran etexilate, and direct oral anticoagulants [DOACs]) types of antithrombotics compared to antiplatelets (aspirin) in crude data, but not in the adjusted model (Table 2, Fig. 2).
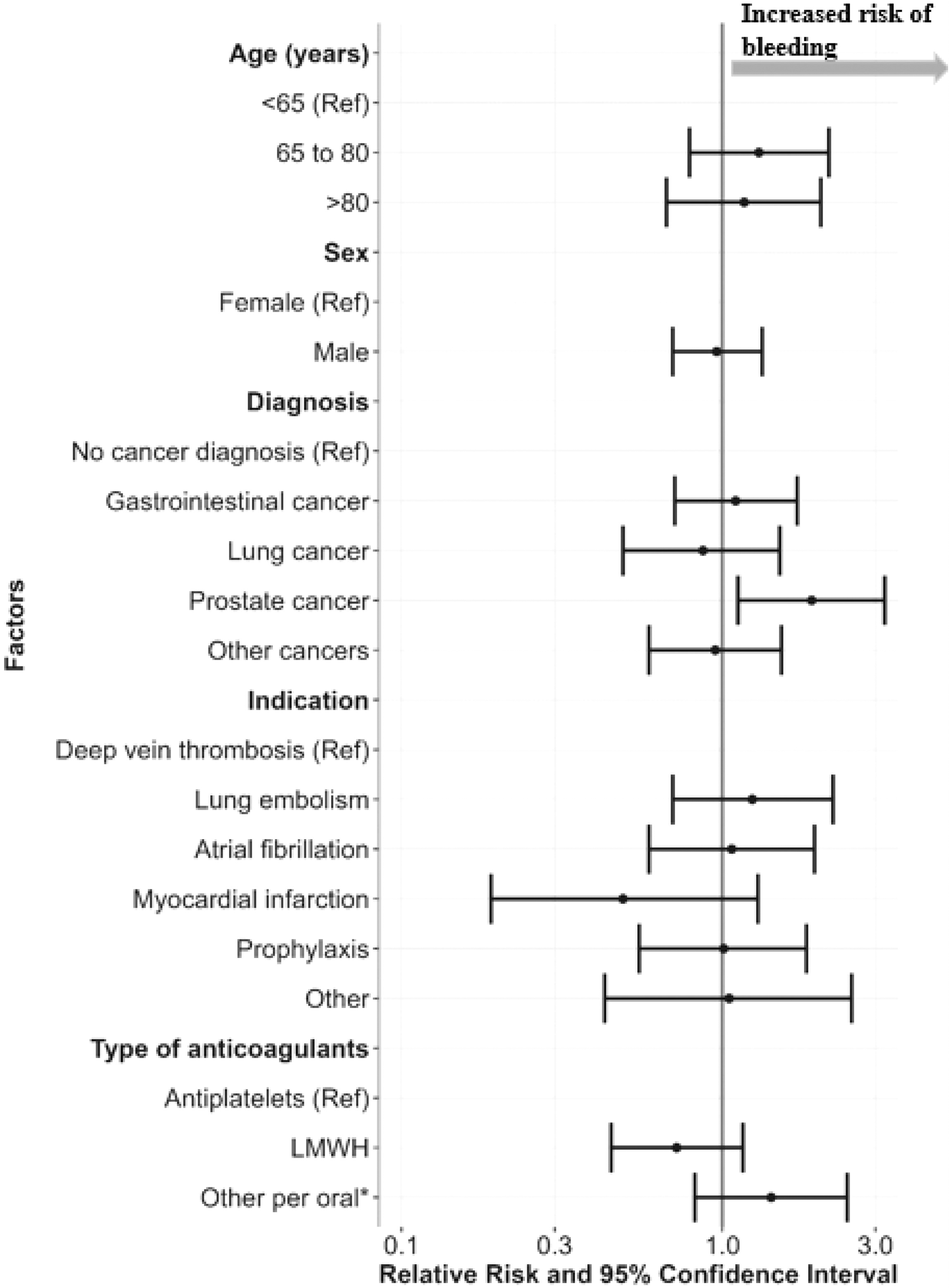
Adjusted relative risk estimates of factors associated with bleeding for patients in palliative care, who used antithrombotics during the last year of life Adjustments were made for sex, age, primary diagnosis, and indication for and type of antithrombotic treatment. *Other per oral (warfarin, dabigatran etexilate, and direct oral anticoagulants [DOAKs]). LMWH, Low-molecular weight heparin.
Relative Risk Estimates of Factors Associated with Bleeding at the End of Life in Deceased Patients Who Used Antithrombotic Treatments in the Last 12 Months of Life, 2016–2018
Statistically significant values in bold data: Percentages are calculated as a fraction of the patients with bleeding across the levels of factors. Relative risks (RR) and 95% confidence intervals (CI) from log-binomial generalized linear models.
Other per oral (warfarin, dabigatran etexilate, and direct oral anticoagulants [DOAKs]).
LMWH, Low-molecular weight heparin.
Effects of deprescribing
Two patients (0.2%) developed strokes after antithrombotics were deprescribed. One had gastric cancer, as well as atrial fibrillation and a previous stroke. After deprescribing apixaban due to gastric bleeding/tumor bleeding and anemia, the patient developed a lethal stroke after 2 months. The other patient had several noncancer diagnoses and atrial fibrillation. Apixaban was deprescribed due to nasal and gastric bleeding and the patient had a stroke after 1 week. The patient died 2.5 months after the stroke due to other causes.
Timing of deprescribing
For 600 patients (66.9%), antithrombotic treatment continued until the last week of life. Anticoagulants were not deprescribed, either at all or until the day of death, for 316 patients (35.2%) in the cohort. For those who continued treatment until the very last days, approximately 44% received this orally. It is not known whether they could actually swallow the medication; most patients cannot take oral medications during the very last days/day of life. Deprescribing more than 180 days before death was more common among patients with cancer compared to the noncancer group (p < 0.05). In addition, deprescribing 8–14 days before death was more common in the group of patients with cancer than in the noncancer group (p < 0.001).
Discussion
Our results show that treatment with antithrombotics in the last year of life for patients in palliative care is associated with the risk of bleeding. In this study, antithrombotic treatment during the last year of life was continued until the last week for 67%, and was not deprescribed at all for 29%. The risk of bleeding was similar between patients with cancer and the noncancer group, and was independent of indication for antithrombotic treatment. Men with prostate cancer seemed to experience more side effects with bleeding than other groups. In contrast, no patient with gynecological cancer had any bleeding during antithrombotic treatment in this cohort. Importantly, only 0.2% of patients developed strokes when antithrombotics were deprescribed.
In this study, the incidence of bleeding was 16.1% for all patients treated with antithrombotics. There is a lack of studies on the frequency of bleeding in patients treated with antithrombotics in palliative care settings. However, in a French study, including 1199 patients on antithrombotic treatment as a primary prophylactic, bleeding incidence was 9.8% in the three months after admission to one of the 22 French palliative care units. 15 In that study, the follow-up time was shorter; three months compared to the last year of life in this study. In addition, only patients with cancer and receiving antithrombotic treatment as primary prophylaxis were included; this is in contrast to our study where patients were included, regardless of diagnosis and indication for antithrombotic treatment. In a Canadian study from 2023, an incidence of bleeding of 10.8% was reported in patients who continued with antithrombotics after being admitted to a palliative care residence versus 7.6% in patients where antithrombotics were deprescribed. 16 However, 78% of the patients discontinued antithrombotics during their stay, which is far more than in our study.
In this study, the risk of bleeding was similar between patients with cancer and the noncancer group treated with antithrombotics during the last year of life. The use of more LMWH in the cancer group is expected and in line with current recommendations.22–25 In general, the risk of bleeding when using antithrombotics is well-known and varies with the type of medication used; direct thrombin inhibitors and factor Xa inhibitors have been associated with lower risk of major bleeding and fatal bleeding than Vitamin K antagonists. However, there are individual risk factors for bleeding, which also affect the overall risk during antithrombotic treatment.26–28 The incidence of bleeding during treatment with warfarin has been described as 15–20% per year, with severe bleeding at 1–2%. 29 Nowadays, the use of warfarin is decreasing in favor of DOACs. It is, however, reasonable that patients, in general, who are treated with antithrombotics have lower rates of bleeding than patients in palliative settings using antithrombotics due to the fragility of these patients.
The prevalence of prescribed antithrombotics in palliative care settings differs in studies from 7% to 60%.1,11 In this study, 60% of the screened patients were prescribed antithrombotics during the last year of life and 57% during the last six months of life, which is in line with other studies. 11 Kowalewska et al. reported that 7% of the patients admitted to a hospice in Oregon, United States, used antithrombotics. 1 However, this is very low and may be due to differences between the palliative care systems in the United States and European countries.
The reasons for the high prevalence of antithrombotic treatments in palliative care settings, and the difficulties in deprescribing these medications, are probably multifactorial. In patients with cancer, there is a high incidence of cancer-associated thrombosis and patients who have previously had a thrombosis are recommended life-long treatment with no guideline for how or when to deprescribe the treatment. Moreover, those with atrial fibrillation are recommended long-term anticoagulation to reduce morbidity and mortality from stroke.
There is no clear guideline for deprescription of antithrombotics in end-of-life care. Patients in late palliative phases often prefer to reduce the number of medications, but they can also have concerns about side effects in terms of bleeding and negative effects from ending the treatments.30,31 In a retrospective, observational study from The Netherlands, Riveras et al. reported the evaluation of a tool for deprescribing antithrombotics for patients with cancer in palliative care (n = 111). 32 This tool included consideration of the patients’ diseases, indication for antithrombotics, if there had been any bleeding, and the risk for thrombosis, and based on the information obtained, gave a recommendation for either deprescribing or not. 33 Eighty patients (72.1%) were treated using the tool. Seven experienced clinical events (2 bleeding and 5 thrombosis) in the tool group and 4 in the nontool group (3 bleeding and 1 thrombosis). There was no significant difference between the groups regarding clinical events. In the tool group, there were both patients who had been deprescribed or had continued antithrombotics. 32 To facilitate future guidelines for deprescribing, there is an ongoing European study, the SERENETY study (toward cancer patient empowerment for optimal use of antithrombotic therapy at the end of life). 34 The aim of the SERENETY study is to develop and evaluate a tool to support patients and their health care professionals in making evidence-based decisions regarding antithrombotics in the end-of-life situation. 34
Strengths and limitations
The strength of this study is the large sample size. In addition and to the best of our knowledge, this is the first study cohort that evaluates bleeding as a side effect of antithrombotic treatment in palliative care in a cohort including both patients with cancer and noncancer diagnoses, and all patients on antithrombotic treatment regardless of indication. The cohort includes a large variety of different diagnoses, both different cancer and noncancer diagnoses. The results from this study could, therefore, be generalizable to other palliative populations in Sweden, and probably also in Europe, since the frequency of antithrombotics in these populations is about the same.
The limitations of this retrospective study were that the variables were extracted from the medical records, which can involve some interpretation of the documentation. A prospective study would have given better quality data, but would have been more difficult to perform and the sample size would have been much smaller. Another limitation is that the variables were extracted from the medical records by only one person. Two people would probably have identified more accurate variables, but this would have taken considerably more time. A further limitation is that the overall deprescribing rate was very low, which makes it difficult to study the risks of deprescribing. Finally, the data were extracted from medical records documented between 2016 and 2018, and the pattern of both prescribing and deprescribing may have changed during the past 5 years. If the study had been performed today (2024), a higher proportion of patients would probably have been treated with per oral antithrombotic, since treatment recommendations changed in 2024 and DOACs became the first choice. 35 In the future, it would be interesting to repeat this study with the current practice of decreased use of LMWH and increased use of DOACs.
Conclusion
To conclude, antithrombotics are a common medication used by patients in palliative care and are often deprescribed very late, close to the person’s death. In this retrospective study, there was a high risk of bleeding in patients using antithrombotics during the last year of life, independent of age and indication for and type of anticoagulants, while the risk of thrombosis was very low after deprescribing in this setting. Patients with advanced prostate cancer had an increased risk of bleeding compared to patients with other cancer types and noncancer diagnoses, which may be clinically relevant in palliative care. However, this finding needs to be confirmed in future studies before firm conclusions can be drawn.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.