
Abstract
Background:
The debate over legalizing medical assistance in dying (assisted dying) is ongoing, also in Nordic countries such as Sweden where assisted dying is illegal. A 2020 survey by the Swedish Medical Association highlighted varied perspectives, with 41% of physicians supporting and 34% opposing legalization. Professionals in palliative care were more negative toward it.
Objective:
To assess attitudes toward the legalization of, and the need for education about, assisted dying among Swedish palliative care professionals.
Study Design:
A survey with 19 closed- and 2 open-ended questions was administered to the participants of the 2023 Swedish National Conference on Palliative Care (including physicians, nurses, assistant nurses, administrators, and researchers).
Results:
Of the 866 conference participants who were invited, 444 (51%) participated. Predominantly, the cohort comprised women (89%); 60% were nurses and 17% physicians. The results showed that 38% opposed euthanasia, 36% supported it, and 26% remained undecided, with similar findings regarding physician-assisted suicide. There was a significant trend of increasingly negative attitudes with age and experience in palliative care (p < 0.01). Physicians emerged as the group most opposed to euthanasia (80%), whereas assistant nurses were the most positive, with 13% opposing legalization, and 33% of the nurses opposed euthanasia. The open-ended questions revealed thoughts regarding the complexity of the issue and the need for further discussion and education.
Conclusion:
In Sweden, where euthanasia and physician-assisted suicide is illegal, more than one-third of palliative care professionals were in favor of legalizing these practices while one-fourth were undecided, these proportions differed markedly between professions. Further, we uncovered a significant need for further discussion and education.
Key Message
Our survey of palliative care professionals’ attitudes toward assisted dying in Sweden shows high correspondence between attitudes toward euthanasia and physician-assisted suicide. It also shows that younger respondents exhibit greater support for legalization, as do nurses and assistant nurses compared with physicians. Further, respondents report a desire for more discussions on the topic and for improved communication skills regarding existential aspects of care.
Introduction
Whether to legalize medical assistance in dying (assisted dying) is a matter of heated debate in numerous countries. The international debate on assisted dying as well as other end-of-life medical decisions is influenced by various factors, including legislation, culture, education, and tradition. Assisted dying is commonly understood to encompass (voluntary) euthanasia and physician-assisted suicide. 1 Euthanasia as practiced in, for example, the Benelux countries involves a physician administering lethal drugs to end a patient’s life at the explicit request of the patient. Physician-assisted suicide, in contrast, refers to the patient self-administering medication prescribed by a physician that is intended to end their life.
Assisted dying in any form is currently prohibited in all Nordic countries, including Sweden. Under Swedish legislation, a physician performing euthanasia could be charged with manslaughter. As for physician-assisted suicide, no law would be breached in Sweden, but as witnessed by a much-publicized recent Swedish case it is considered a breach of professional conduct. 2 In contrast, Swedish health care law does not prohibit ending life-sustaining treatment by discontinuation of, for example, mechanical ventilators, fluid support, antibiotics, and dialysis. Such discontinuation can be done at the explicit request of a decision-capable patient or if the treating physician deems the intervention to be futile. 2 A contrast can be drawn with those countries where this practice is considered a form of “passive euthanasia” and seen as controversial and/or illegal. Additionally, Swedish health care law allows for palliative sedation in selected cases with refractory distress, by the administration of medications that may potentially shorten life, such as carefully titrated doses of midazolam, 3 when a patient’s condition has progressed to a point at which death is imminent.
Several studies have investigated support for assisted dying among health care professionals in the Nordic countries. Two articles found a slight increase in support for assisted dying among Swedish physicians between 2007 and 2020, with the later study finding 47.1% of physicians in favor of legalizing assisted dying, with young physicians being more in favor than other age groups.4,5 A survey conducted by the Swedish Medical Association in 2020 reveals somewhat more negative views, with 41% of physicians in favor of legalizing assisted dying, while 34% clearly stated they were against it. 6 In a recent questionnaire survey from 2020, it was found that Finnish physicians’ ambivalence toward euthanasia has decreased over the past decades with 42% of physicians working in the care of dying patients now in favor of the legalization of euthanasia in Finland, compared with 49% of physicians working in other fields. 7 A Norwegian study of nurses’ attitudes toward assisted dying found a slight majority in favor of assisted dying, 8 whereas a Norwegian study of physicians’ attitudes instead showed only 30.6% in favor. 9
A Swedish study showed that physicians working in palliative care were more negative toward assisted dying than physicians from other fields. 4 An international comparative study of seven countries showed that Swedish physicians to a higher degree than physicians from other countries thought that good palliative care may make assisted dying redundant. 10 International studies also indicate that health care professionals within palliative care may be more negative to assisted dying than health care professionals within other fields.8,11
At the 2023 Swedish National Conference on Palliative Care, participants (physicians, nurses, assistant nurses, administrators, and researchers) were invited to complete a survey about attitudes to assisted dying. By intentionally and nationally addressing assisted dying within the context of a conference on end-of-life patient care, rather than avoiding the topic, we aimed to stimulate further discussions about this dimension of palliative care. With the survey, a secondary aim was to shed light on the educational needs of health care professionals, highlighting the importance of education in navigating discussions about assisted dying with seriously ill patients and their closest relatives. It is important to understand the attitudes specifically of palliative care professionals toward assisted dying as they are strongly affected by current practices and possible legislation and are well positioned to advocate (or not advocate) for change.
Aim
To assess attitudes toward the legalization of, and the need for education about, assisted dying among palliative care professionals in Sweden.
Methods
Study design
This study was a cross-sectional online survey of attendees at The National Conference of Palliative Care, which collected palliative care professionals from all Sweden and took place in Malmö, Sweden, from October 2 to October 4, 2023. This was a unique opportunity to reach a sample of the palliative care professionals in Sweden, not selected on regional area or profession. All attendees to the conference were invited to take part in the study anonymously.
The study questionnaire comprised 19 closed-ended tick-box questions (17 multiple-choice questions and 2 dichotomous questions) and 2 open-ended questions (Appendix A1). The questionnaire was pretested for length, comprehensibility, and feasibility for online use by five health care professionals with extensive clinical and academic experience in palliative care: two medical doctors and three registered nurses. Based on their feedback, minor adjustments were made to improve the consistency of response alternatives and to refine the terminology used, particularly regarding “euthanasia,” “physician-assisted suicide,” and “assisted dying.” Furthermore, we replaced the term “guidance” with “education and training.”
The survey collected data on respondent characteristics, opinions concerning euthanasia and physician-assisted suicide, and the respondents’ experience in addressing these questions from patients and their next of kin. Characteristics such as gender, age, profession, specialized training in palliative care/medicine, years of professional experience, and highest level of education were sought. Additionally, the survey included questions to assess respondents’ views on the need for educational and communication training in addressing questions about assisted dying.
The two open-ended questions invited respondents to share their perspectives on the survey and any matters related to euthanasia and physician-assisted suicide.
In addition, anonymous data on all the participants’ professions (regardless of whether they participated in the survey or not) were collected from the congress’s organizing agency; this was the only available information on the characteristics of all the delegates.
Distribution of the web survey
Invitation e-mails were dispatched to those registered for the conference in three batches from June 2, 2023 to August 29, 2003. Each invitee received one initial invitation, and a reminder was sent two weeks later, irrespective of whether the invitee had responded or not. The survey closed on October 1, 2023. The e-mail included a hyperlink to the questionnaire and provided information regarding the study along with concise details about euthanasia, physician-assisted suicide, and the legal framework on these issues in Sweden.
Statistical analysis
The quantitative data were analyzed with descriptive statistics, statistical significance was tested with chi-squared test or Fisher’s exact test as appropriate, and trend tests were performed with logistic regression. To investigate the separate effects of the correlated factors gender, profession, age, and years of experience, we used restriction and stratification. Owing to the uneven distribution of gender among the professional groups and the relatively small sample, the analysis of gender was restricted to nurses and physicians. For the effects of age and experience, we categorized age as a binary variable (above/below 50 years of age) and in these strata reported the attitude toward euthanasia among levels of experience working in palliative care. Missingness was relatively low, and a complete-case analysis was employed. All data cleaning and analyses were done in SAS Enterprise Guide Version 8.3 (SAS Institute Inc, Cary, USA).
The survey was completed anonymously, thus ethical approval was not required under the Swedish legislation. However, we sought an advisory opinion from the Ethics Review Authority regarding the questionnaire, and they raised no objections (Dnr 2022-07261-01). Data collection, handling, and storage complied with the EU general data protection regulation.
Analysis of open-ended questions
The comments related to assisted dying were transcribed verbatim and analyzed with thematic analysis inspired by Braun and Clarke. 12 First, all comments were read to obtain a sense of the whole. Next, comments were coded, then compared, discussed, and finally developed into three themes.
Results
Study population
Among the 866 participants at the conference, of whom all were invited to complete the survey, 444 (51%) chose to take part. The nonresponders were relatively evenly distributed among the professions, apart from the psychosocial professionals, for which a larger group (76%) chose not to participate. The study population is largely made up of women (89%); 60% are nurses and 17% are physicians, but rehabilitation staff and psychosocial staff are also represented (Table 1). The participants are fairly well distributed over years of experience in palliative care and 40% hold a specialization within their profession in palliative medicine/care. Two participants did not answer the question on euthanasia and were omitted from the analysis.
Characteristics of Respondents in Relation to Attitude Toward Euthanasia
Number of observations missing: gender: 3, age: 2, profession: 1, specialization: 2, physician-assisted suicide: 4.
Chi-squared test.
Physiotherapist, occupational therapist, dietician.
Social worker, priest.
Results from quantitative analyses
The overall attitude toward euthanasia showed that 38% were negative toward the legalization of euthanasia in Sweden, 36% were positive and 26% were undecided (Table 1). When asked about their attitude toward physician-assisted suicide, 38% responded with a positive attitude, 36% reported a negative attitude and 26% were undecided. The opinions regarding euthanasia and physician-assisted suicide corresponded to a large degree (79%); 8% were in favor of one of the concepts and negative toward the other, and the remaining 13% were decided about one of the concepts but undecided regarding the other. Because of this correspondence, and in the interest of brevity, we will from hereon report the results for euthanasia, and not physician-assisted suicide, as euthanasia might be regarded as the more controversial concept.
The attitudes toward euthanasia were statistically significantly different over age, profession, experience in palliative care and whether or not the participant held a specialization in palliative care (all p < 0.05). The difference between genders was not statistically significant (p = 0.06) (Table 1). With regard to age and experience, there was a statistically significant linear trend of a more negative attitude the older the respondent (p < 0.01) and among those with greater experience (p < 0.01). Regarding professions, the most negative group was the physicians (80% opposing legalization of euthanasia), while assistant nurses were the most positive with 13% opposing legalization (Fig. 1).
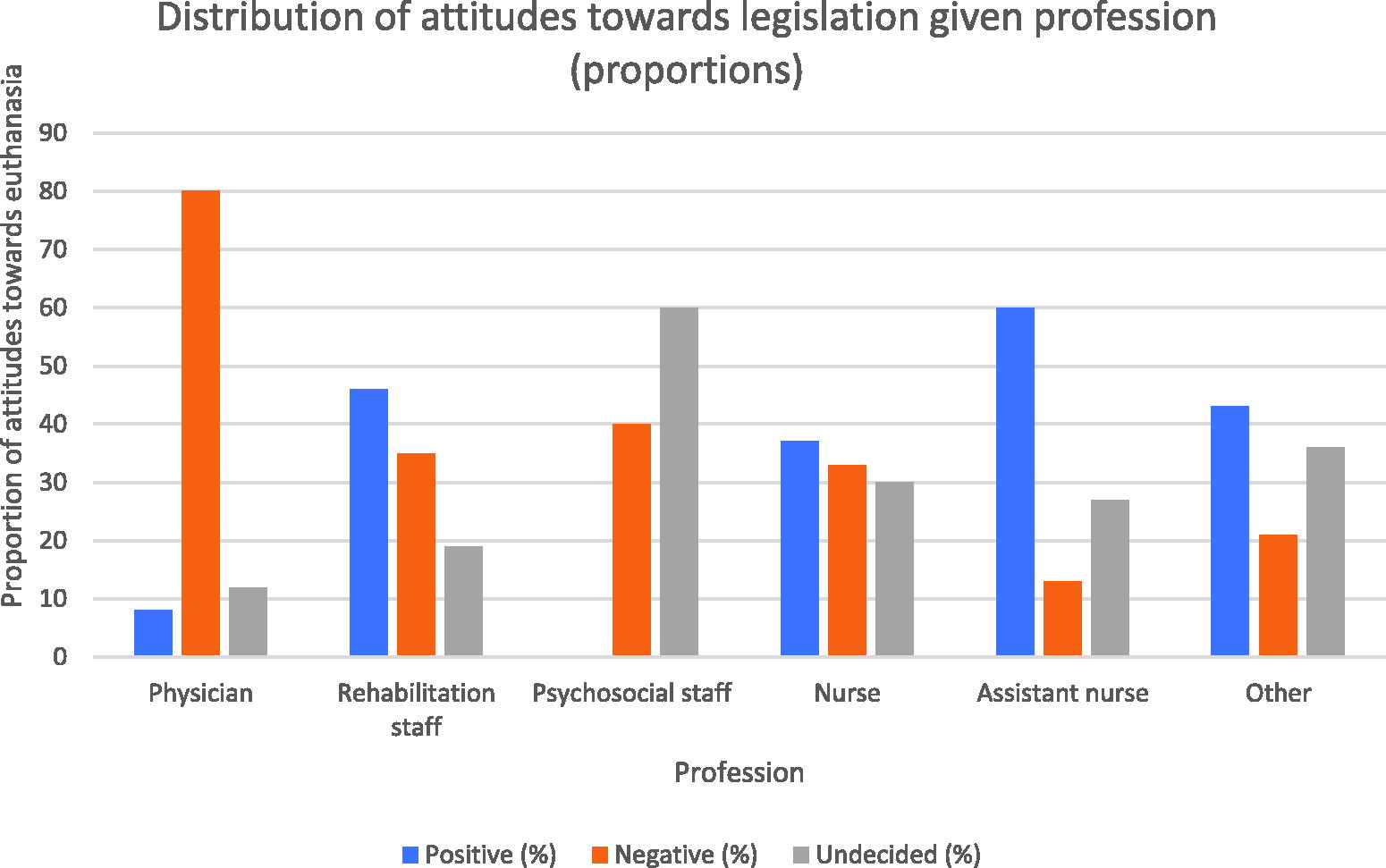
Distribution of attitudes toward euthanasia given the profession (proportions). The X-axis represents different professions, while the Y-axis shows the proportion of attitudes toward euthanasia, expressed as percentages. The blue bars represent the proportion of negative attitudes, the yellow bars indicate the proportion of positive attitudes, and the gray bars reflect the proportion of individuals who are undecided. Data are presented as percentage distributions within each profession.
To disentangle the effect of gender and profession, we restricted our analysis to nurses and physicians. Female and male nurses have similar attitudes toward euthanasia with no statistically significant difference between the groups (33% and 38% opposing legalization, respectively, p = 0.24). We similarly found no statistically significant difference between physicians of different genders (females 81% opposing legalization, males 77% opposing legalization, p = 0.5) (Table 2). To investigate the effect of experience in palliative care in relation to the age of the participant, we stratified the analysis into two age groups: below and above 50 years of age. In these two groups, there was still a statistically significant difference in attitude toward euthanasia depending on the number of years in palliative care (p < 0.01 for the younger group, p = 0.03 for the older group). However, the numbers in each category are relatively small and the proportions show no linear trend, hence we conclude that there is an inconsistent relationship between palliative care experience and attitude toward euthanasia.
Attitudes Toward Euthanasia in N (%) Over Gender in Panel A and Over Age (±50 Years) in Panel B
Panel A is restricted to analyzing nurses and physicians only. In panel B, the sample is stratified on respondents’ years of experience in palliative care.
Chi-squared test.
Fisher’s exact test.
With regard to questions, wishes, and requests for euthanasia, we found a wide variety: while 18% of the health care professionals reported that they never get questions on euthanasia from patients, 25% report questions once a year, 38% report receiving questions 2–6 times/year and 19% reported that they get questions 7–12 times/year or more (Table 3). Questions about euthanasia were more common than requests for it, and patients more commonly both asked questions and requested euthanasia than family members. Family members of the patient expressing requests were the least common, with 54% of the health care professionals reporting never receiving them. There was a statistically significant association between how often one receives questions/wishes/requests of euthanasia and one’s own attitude toward the concept (p < 0.01). People who encountered the topic 7–12 times/year or more were more strongly in favor of legalizing euthanasia (49%) and less undecided (17%) in comparison to people who encountered the topic once per year, among whom 22% were in favor and 33% were undecided (Fig. 2).
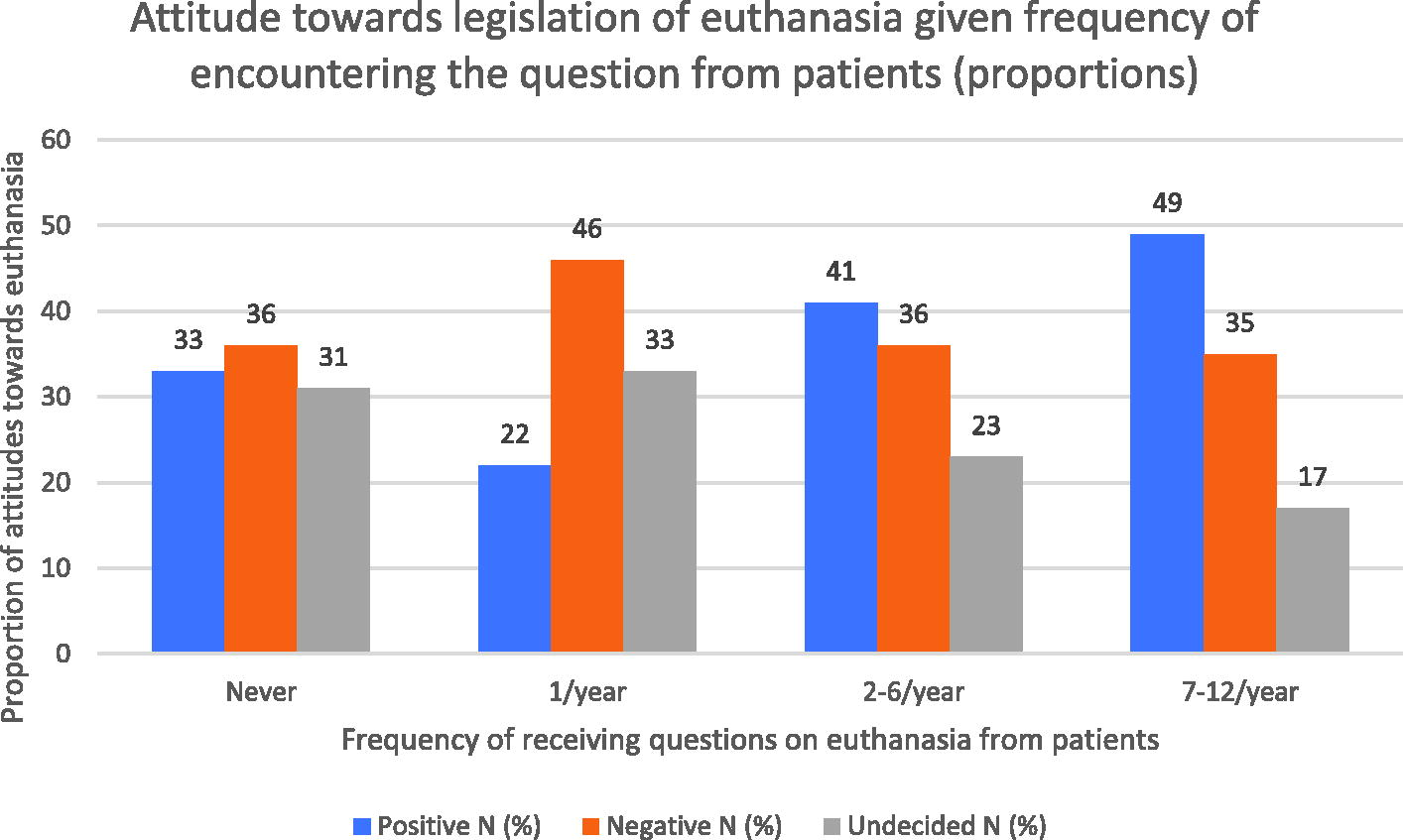
Distribution of attitude toward euthanasia given the frequency of encountering the question from patients (proportions). The X-axis represents the frequency with which health care professionals encounter questions, wishes, or requests for euthanasia from patients, shown as proportions. The Y-axis indicates the proportion of attitudes toward euthanasia among health care professionals, expressed as percentages. The blue bars represent negative attitudes, the yellow bars indicate positive attitudes, and the gray bars reflect undecided attitudes. Data are presented as percentage distributions for each level of encounter frequency.
Frequency and Proportion (%) of Encountering the Topic of Euthanasia with Patients and Family
Characteristics of the Participants (N = 100) Who Gave Comments Related to Matters of Assisted Dying
Number of observations missing: gender: 1.
Physiotherapist, occupational therapist, dietician.
Social worker, priest.
Regarding the topic of “education and training,” 30% of professionals agreed or strongly agreed that they needed further training on handling patient and family questions about assisted dying and related existential issues (questions 18 and 19 of the questionnaire, Appendix A1).
Results from qualitative analyses
In total, 100 participants (22%) gave comments related to assisted dying (for demographics, see Table 4), and from these comments, three themes were developed:
A complex and difficult issue that requires discussions and investigation.
According to the comments, euthanasia is not a question that can easily be answered with a simple yes or no to legalization. Comments suggest that one reason for desiring euthanasia is to have control over one’s own life and death, but it was also reported that it is unclear whether a request for euthanasia is a probing question or a real wish to receive euthanasia. Patients often fluctuate between wanting to live and wanting to die, depending on their situation. Discussing assisted dying with colleagues and in society is important due to the complexity of concepts such as autonomy, suffering, and assisted dying as well as the distinction between treatment restrictions and euthanasia. The need to initiate a debate and investigate the issue further was emphasized in the comments.
I would like a discussion forum with other colleagues and a government investigation into this. (Physician, F, 11–20 years experience in PC)
In discussions about treatment limitations, ideas tend to emerge that equate it with issues of euthanasia. (RN, M, >20 years experience in PC)
Good palliative care and symptom relief counteract the desire for euthanasia.
According to the comments, there is no need to legalize euthanasia if patients’ suffering is alleviated, as the desire for euthanasia often stems from inadequate symptom relief, feelings of loss of control, fear, and crisis. A lack of resources results in patients not receiving good palliative care, which can lead to requests for euthanasia. Furthermore, patients in need of specialized palliative care are not always referred to palliative care by their physicians. Some comments emphasized the importance of supporting patients in living their remaining time, even when they feel hopeless.
If we can sufficiently alleviate symptoms at the end of life and spread awareness about this, perhaps the need for assisted dying is no longer relevant. (RN, F, 5–10 years experience in PC)
Good palliative care can make euthanasia an undesirable concept. (AN, F, 5–10 years experience in PC)
Clinicians need skills to talk about existential issues including euthanasia.
Comments suggest that health care professionals do not talk enough with patients about death, feelings of discomfort, and fears about dying. They emphasize the importance of maintaining a continuous dialogue with patients and families, based on their wishes and concerns and with health care professionals they trust. However, knowledge and skills are needed to talk about the existential aspects of death and to talk with patients who express a wish to die. Some comments point to no training at all and others to their team discussing these issues every week. However, comments suggest that individuals are never full-fledged in their training but need continuous training and practice related to patients’ and families’ existential needs, suffering, and wish for death.
I would like to participate in a course enabling me to talk with patients and relatives specifically about death, euthanasia, and thoughts on these difficult issues. (Rehab, F, <5 years experience in PC)
Discussion
This study shows conflicting attitudes toward the legalization of assisted dying among Swedish palliative care professionals, with 38% opposing the legalization of euthanasia, while a similar but slightly smaller proportion, 36%, are in favor, and 26% remain uncertain, and similar findings regarding physician-assisted suicide. Factors associated with being opposed to euthanasia include being a physician, being older, and having more experience with palliative care, whereas gender had no significant impact. Discussions about assisted dying were reported to be relatively infrequent occurrences, with questions being more common than actual requests for assisted dying. Those who reported discussing assisted dying up to once a month were more positive than those who discuss it more seldom or never.
Strengths of this study include that the sample consists of all palliative care professions, making the sample broader than in previous Swedish studies. The study participants also come from all regions of Sweden. These two facts make the results more generalizable. Further, facts that the study includes both quantitative and qualitative analyses help to shed light on this complex issue from several angles. The response rate for this survey is 51%, which is in line with many surveys of healthy people. However, since the underlying population, that is, the population that could have come to the conference and thereby been invited to the survey, is difficult to characterize, it is therefore also difficult to assess how our sample might differ from this underlying population.
Our study is consistent with a recent survey by the International Association for Hospice & Palliative Care, which showed ongoing debate and no consensus among members about assisted dying. 13 Our work also corroborates previous findings that nurses favor the legalization of assisted dying compared with physicians, 14 who tend to show a more negative attitude. 15 In the present study, the relationship between higher age and a more negative attitude toward euthanasia is both strong and linear, suggesting a potential causal relationship. In line with our findings, previous studies suggest that higher age but also male gender are correlated with more negative attitudes toward assisted dying among physicians and lay people, 16 and that younger individuals are more positive toward assisted dying compared with older adults and the general public.17,18 Surveys conducted among medical as well as nursing students in various European countries where assisted dying is not legal have shown a high level of support for assisted dying,19,20 a trend that has remained consistent over past decades.21–23 These attitudes may undergo reassessment owing to assimilation into a professional identity influenced by attitudes within the group. Changing attitudes may also be an expression of an ongoing liberalization concerning assisted dying in society.6,7,24
The qualitative analysis of the two open-ended questions and the comments related to assisted dying highlights the many complexities surrounding this issue. Comments underscore the need for a nuanced exploration, rather than a simplistic yes or no stance on legalization. Patients’ desires frequently vary, underscoring the significance of comprehensive palliative care and open dialogue between health care professionals and patients.
The results show great variation in the frequency with which participants receive requests for and questions on assisted dying, but in general, they are rare events. The variation may partly be explained by the fact that participants in this study come from different health care settings in the palliative care landscape. Studies from other countries similarly indicate that questions about or requests for assisted dying occur among a minority of patients. For instance, recent studies from France and Spain indicate that about 1 in 10 palliative care inpatients talk about assisted dying, and two to three in a hundred express a wish for assisted dying.25,26 It should be kept in mind that assisted dying was illegal at the time the studies were conducted, as it still is in Sweden. It has been previously shown, as in our study, that all the different professions working in palliative care may receive questions about assisted dying. 25 Previous studies also indicate that the frequency of such conversations is associated with the professional’s own attitudes and behavior. For instance, staff who ask patients if they consider hastening death, and have a neutral or positive attitude to assisted dying, are more likely to have conversations with patients, and next of kin, on this topic.26,27 This finding is fully consistent with ours that professionals who are more positive toward assisted dying report having more such conversations. We note that the causality in this association might conceivably go either way. Free-text answers in our study suggest that conversations about existential issues are perceived as difficult. Previous studies indicate that difficulties may relate to distinguishing temporary or insincere death wishes from more serious ones, and to a fear of appearing to suggest assisted dying.28,29 One may also speculate that the relative paucity with which most respondents have this kind of discussion may further contribute to the perception of the discussions as “difficult.” Although there are guidelines for having these difficult conversations in some countries, 30 no such guideline exists in Sweden.
In the present study, many Swedish palliative care professionals rated their knowledge of assisted dying as low and identified a need for more education on the topic. Specifically, 30% of professionals agreed or strongly agreed that they felt a need for education and training on this topic. This finding aligns with previous international data, which suggest significant knowledge gaps.15,31,32 At the same time, it is likely difficult and perhaps less relevant to gain in-depth knowledge about assisted dying in countries where such practice is illegal. For instance, when Canada legalized assisted dying in 2015, there were no professional training programs on the topic, but today such training is becoming widely available 33 as well as guidelines on how to teach staff to handle the practical and emotional aspects of assisted dying.34–36 Hence, there may be reason to think that knowledge levels reflect an “as-needed” logic, and that knowledge would increase if legislation were to change.
In terms of implications for practice, the findings underscore the importance of professionals having or developing communication skills when it comes to discussions about refraining from or discontinuing treatment. In light of the expressed need for further training, future studies could be undertaken to assess what knowledge palliative care professionals already possess and what, more precisely, they may need.
In conclusion, this study shows the complexity of palliative care professionals’ perspectives on euthanasia and physician-assisted suicide and the great variation in attitudes among professionals. We determined that many palliative care professionals perceive discussions with patients and families on the topic to be difficult; additional communication training and communication guidelines could therefore potentially help.
Footnotes
Acknowledgments
The authors extend their appreciation to MKON AB for their work in distributing e-mails with research participant information outlining the study and links to the survey to conference participants. Additionally, the authors would like to thank Ola Stjärnhagen at Lund University or the valuable system support of the Sunet Survey tool.
Authors’ Contributions
Conception: M.S. and M.E.C.S. Design: M.S., M.E.C.S., I.B., J.B., C.J.F. and B.R. Thematic analysis of open-ended questions: B.R. and I.B. Conception of the article and continuous revision of the article: M.S., M.E.C.S., J.B., J.J., M.E., I.B., C.J.F., and B.R. All authors approved the version to be published.
Ethical Considerations
The application was submitted to the Ethical Review Authority on December 27, 2022 (2022-07261-01). Subsequently, a statement was issued by the Ethical Review Authority, indicating no ethical objections to the research project, on February 21, 2023.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Appendix A1
Survey of Palliative Care Professionals’ Attitudes Toward Assisted Dying in Sweden, Translated from Swedish to English, Containing 19 Closed-Ended and 2 Open-Ended Questions
| 1. | Background question: gender? |
| 2. | Background question: age? |
| 3. | Background question: profession? |
| 4. | Background question: specialist training in palliative care/medicine? |
| 5. | Background question: number of years in current occupation? |
| 6. | Background question: number of years working in palliative care/medicine? |
| 7. | Background question: in which activity are you employed? |
| 8. | Background question: with which principal are you employed? |
| 9. | Background question: do you have a higher academic education; PhD, Master, Master’s (any subject)? |
| 10. | Your attitude to assisted dying: do you think euthanasia should be legalized (= become legal) in Sweden? |
| 11. | Your attitude to assisted dying: do you think that physician-assisted suicide should be legalized (= become legal) in Sweden? |
| 12. | Assisted dying: how often do you get questions about assisted dying from a seriously ill patient? |
| 13. | Assisted dying: how often do you receive a request for assisted dying from a seriously ill patient? |
| 14. | Assisted dying: how often do you receive questions about assisted dying from relatives of a seriously ill patient? |
| 15. | Assisted dying: how often do you receive requests for assisted dying from relatives of a seriously ill patient? |
| 16. | Assisted dying: do you think you have enough knowledge about assisted dying? (Where 0 is no knowledge and 5 is that you have enough knowledge.) |
| 17. | Assisted dying: in the workplace where you work, do you think you have the resources and skills needed to alleviate symptoms and suffering at the end of life? (Where 0 is very inadequate resources and skills and 5 is very good resources and skills.) |
| 18. | Education and training: do you need education and training on how to deal with patients and relatives with questions about assisted dying? (Where 0 is no need and 5 is high need for education and training.) |
| 19. | Education and training: do you need education and training in talking about emotional and existential issues related to assisted dying? (Where 0 is no need and 5 is high need for practical training.) |
| 20. | Your further thoughts and comments on this survey? |
| 21. | Your additional thoughts and views on assisted dying? |