
Abstract
According to Greek mythology, Sisyphus frustrated the other Gods in the Olympus, and they condemned him to carry a heavy rock up a hill that rolled back down when he got to the top, forcing him to repeat this action for eternity.
For more than 40 years, we have known that effective palliative care needs an interdisciplinary team (IDT) led by a palliative medicine specialist. However, this is still not happening in most hospitals and cancer centers in the United States and the rest of the world. Executives in these institutions pose structure (not enough team members) and perhaps more importantly process (administrative arrangements) barriers that make this complex care very difficult for all clinicians. This commentary addresses some of the challenges and opportunities in the creation and operation of the IDT.
Why do we need interdisciplinary teams in palliative care?
Hospitals and cancer centers are very good at diagnosing and treating disease. Structures, processes, and outcomes are oriented to these goals. When the disease progresses, there are less biomedical resources at a moment when the physical, psychosocial, and spiritual suffering increases dramatically. Personhood care is always multidimensional. 1 Even symptoms that are apparently purely physical, such as pain and fatigue, are heavily influenced by psychological, family, and spiritual suffering. Members of an interdisciplinary team work together to diagnose and manage these multiple and quite personal components of suffering. They also identify sources of joy, legacy, meaning, and anticipatory bereavement, and those are always personal and contextual. This is always complex work.
Patients and families may be able to “open up” to the physician, nurse, pharmacist, chaplain, or social worker, or psychologist according to their level of trust in their different roles. The IDT frequently has members from different demographics such gender, race, ethnicity, age, and cultural background, and this helps patients and families from multiple backgrounds feel safer at an extremely vulnerable time in their lives.
Multiple randomized controlled trials have demonstrated that interdisciplinary palliative care teams lead by a palliative medicine specialist improve symptom burden, quality of life, multiple end of life metrics, and the cost of care.2–3
On the other hand, palliative care delivered by a single specialized discipline and primary palliative care have not been consistently successful in randomized controlled trials.2–3
The ideal IDT structure and function.
Figure 1 summarizes the IDT circle of care. Some programs need other disciplines as part of the circle, depending on the patient population. All American hospitals and cancer centers employ individuals from each of these disciplines.
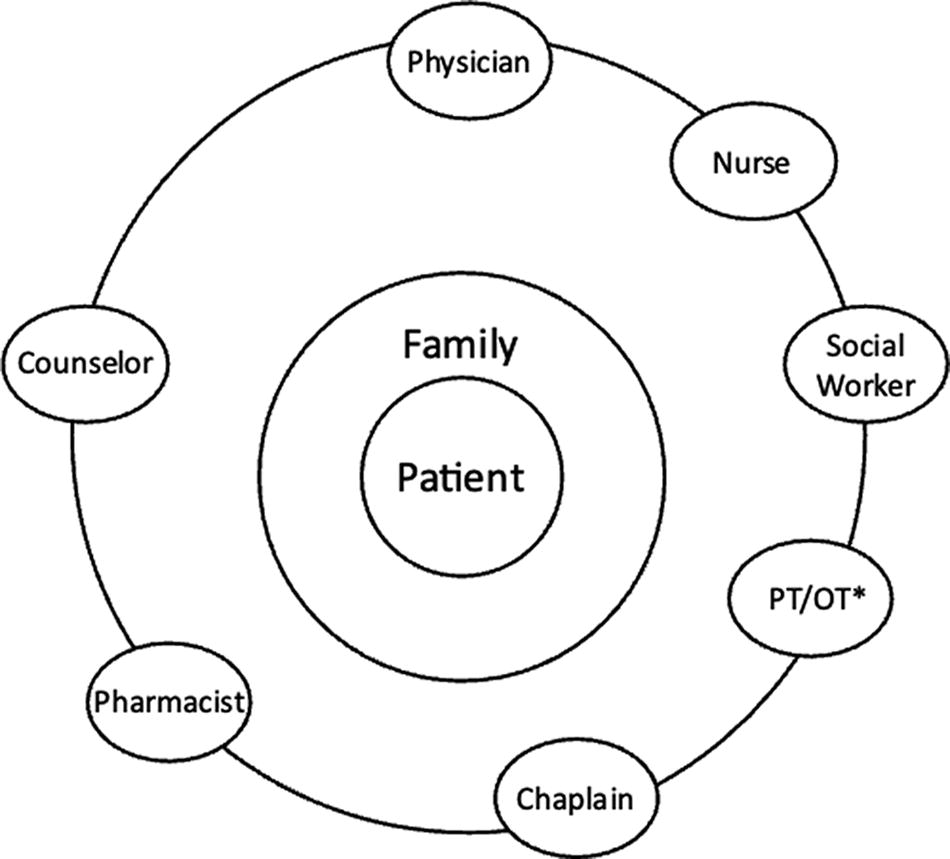
The interdisciplinary team circle of care. *PT/OT, Physiotherapist/Occupational Therapist.
Severely distressed patients and families referred to palliative care are frequently diagnosed with psychiatric, personality, or substance use disorders, family or clinician conflict, and financial and spiritual suffering. The IDT needs to function extremely well under pressure. A patient may present with persistent pain of 8/10 due to problems with opioid titration, depression/anxiety, fear of death/loneliness, concerns about their children/spouse, substance use disorders, or disinhibition due to early stages of delirium. Frequently several or all these factors coexist. Each team member contributes a piece to the puzzle and understands the multiple other dimensions of patient and family suffering. This way they can all provide consistent communication and care. This only happens after hundreds of IDT encounters with patients and families. Repeatedly working together, members develop trust in the ability of this interdependent team to alleviate complex patient and family suffering. The process can be lengthy and painful sometimes. I heard several times Balfour Mount say: “So you have been in a team: show me your scars!”.
So why bother? Simply because a group of us working in an IDT can achieve much better results than those of the best solo practitioner. Palliative care is a team endeavor similar to multiple areas of human interaction in music, sports, and business. Team members do not need to be outstanding, but they need to be able to work with mutual respect, continuous communication with other team members, a shared vision, willingness to learn from each other, and generosity to support other team members who need help.
The IDT leader has ultimate ethical and legal responsibility for the team’s function and outcomes. Their role is to ensure that the team works harmoniously and that all members feel safe. The leader also needs to be able to remove from the team those members that are consistently disruptive or non-contributory, since those members demoralize and burn out other team members with resulting poor patient care.
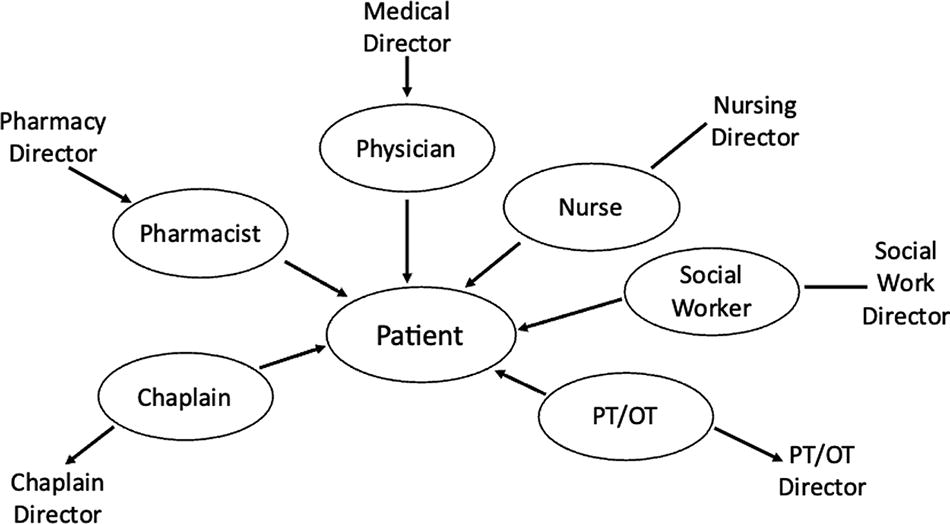
The real structure and function: the Sisyphus job.
Neil MacDonald was my first boss and mentor in Canada. As a wise Cancer Center director, he frequently advised me that “administrative arrangements are important”. As a junior faculty, I did not understand what he meant and did not ask. Only after many years, I was able to understand the power of his advice. Figure 2 shows the administrative arrangements and clinical deployment of different team members in most acute care hospitals and cancer centers in the United States. Each discipline reports to a different administrative director, and care metrics are mostly limited to the patient rather than the patient/family unit we emphasize in palliative care, as shown in Figure 1. Family care is frequently excluded by administrative directors due to lack of easy metrics and billing, even though guidelines support the importance of family care. 3 Recruitment, annual evaluation, and metrics for productivity are defined by the administrative director who has limited or no understanding of the complex delivery of palliative care, and therefore use metrics that are usually applied to multiple other areas of the hospital or Cancer Center. In this model multiple disciplines might parachute as silos to see a patient with limited understanding of what the other disciplines are doing and a different sense of interdependence and trust.
The real IDT structure and formation.
Over many years of visiting hospitals and cancer centers in the United States, Canada, Europe, and Asia, I have learned about countless examples of the problems associated with these structures. The following paragraphs summarize a small number of these clinical situations.
A patient with persistent high pain expression after multiple pharmacological and non-pharmacological interventions was diagnosed as having suffering contributing to the pain expression (defined by Dame Sicily Saunders as “total pain”).
4
This was related to the impending death, persistent family conflict, and severe financial distress. The counselor deployed by their director came to see the patient and left after a few minutes. Their note said that they should be called again “when the patient was in better pain control.” A “team member” received outstanding annual evaluations from their director year after year, although they were rarely seen by the rest of the team members. After a Sisyphus effort collecting data on clinical encounters by the rest of the team, it was possible to demonstrate that this person saw less than two patients per clinical working day, leaving the bulk of the burden to other IDT members. A “team member” focused their clinical encounters on the importance of smoking cessation and the investigation of potential sexual abuse in childhood. When the rest of the IDT advised that these interventions might not be useful, and might be harmful in the last days of life, the member responded that they were practicing as their director felt most appropriate with no intention to refocus their practice. Two different directors used productivity benchmarks for their palliative care member direct reports based on the much shorter encounters needed in other areas of the hospital. Consequently, their IDT members consistently received poor evaluations and over the years several left, burnt out, although they were highly appreciated by the rest of the palliative care team. Several years during the holiday week (the most distressing time for our patients and families receiving palliative care), there were no IDT members because all their directors decided to give them vacation or redeploy them to other clinical areas to cover for other employees who were on vacation.
Whenever I give a talk about the problems with nonfunctioning IDT situations, there are always multiple participants who report similar or much worse examples of IDT malfunction. This malfunction frequently can be traced to administrative arrangements and has serious impact on patient and family care, end of life care metrics, and professional burnout of team members as well as the referring teams, who lose trust in the ability of the palliative care team to help them with their most demanding cases.
Where do we go from here?
Many executives, whether they are clinicians or not, have completed MBAs, and they understand the value of an effective interdependent team to achieve their goals. Unfortunately, many of them also believe that clinicians (who are frequently described as “providers”) are interchangeable, and the vertical reporting in Figure 2 works just fine.
Most executives I have met state that this is a matter of cooperation, since at the end “we are all part of a big interdisciplinary team.” Cooperation requires a busy IDT clinical leader to collect data and clinician feedback, usually with no administrative support, and then meet with seven or eight different administrative directors who rarely understand the special clinical and metric palliative care challenges. This exhausts and demoralizes team leaders. The combination of high responsibility for complex patient care with no administrative autonomy results in frequent burnout, 5 and probably explains the very high turnover among IDT clinical leaders. The alternative to cooperation is integration: team members should not only be clinically but also administratively interdependent. Integration allows team members to develop and monitor consensual metrics, distribute workload according to the patient and family needs, and effectively support each other. When necessary for licensing and continuing education reasons, a dual reporting to a director and the team can be arranged, with primary responsibility to the IDT leader.
Ultimately, what is at stake is the alleviation of unnecessary suffering in our patients and their loved ones and the burnout of team members.
I personally never did an MBA, but after many years working within IDTs, I have learned (sometimes painfully) that an IDT only becomes successful after seeing together hundreds of patients. Monica Aldama, the cheerleading team coach behind the consistent phenomenal success of the small-town Navarro College said it best: “You keep going until you get it right, and then you keep going until you cannot get it wrong.” 6 Give us an integrated palliative care IDT, and we will make you proud.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.