
Abstract

Management of headache and facial pain in palliative medicine remains a challenge owing to complex anatomy of the area, mixed nature of the pain, and limits of pharmacotherapy. 1 Procedural techniques like Sphenopalatine ganglion (SPG) block can be an effective (Fig. 1) 2 treatment, regardless of the etiology of the pain. 1
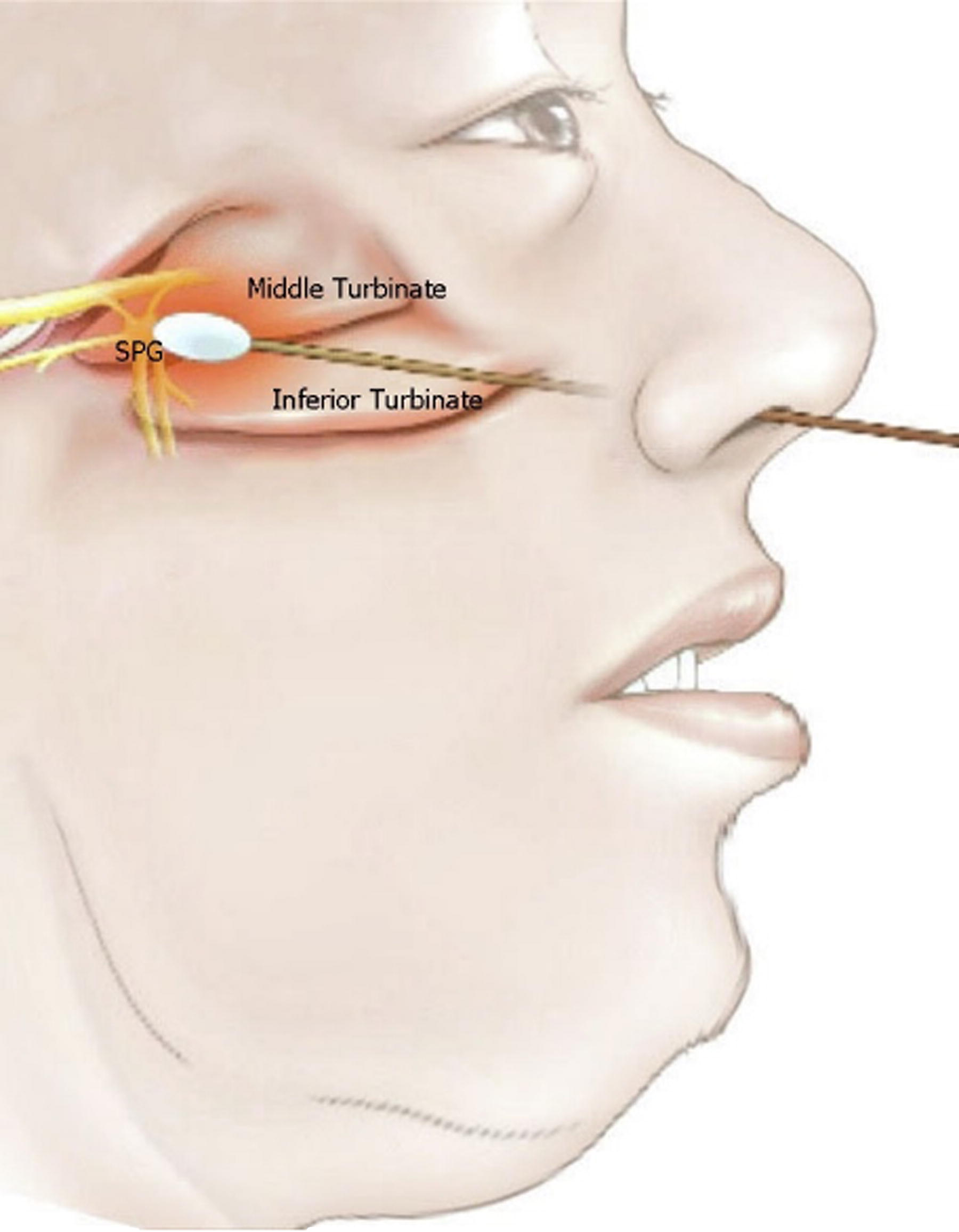
Intranasal transmucosal application of sphenopalatine ganglion block.
In this study, we explored patient satisfaction with the SPG block for management of headaches and/or facial pain. Ethics approval was obtained (St Vincent’s Health and Aged Care Human Research Ethics Committee HREC#19/17, Mater Misericordiae Ltd Human Research Ethics Committee HREC/MML/60129). Eligible participants recruited between July 2019 and November 2020 were over 18 years old, had advanced disease, received a SPG block for headache or facial pain, and provided written informed consent. Exclusion criteria included bleeding disorders, nasal obstruction or deformity, active nasal, sinus disease or recent surgery, confusion, dementia or delirium, and allergy or sensitivity to lignocaine. Data collection included patient demographics, details of procedure application, side effects, pain scores, and patient satisfaction.
Seventeen patients were recruited (aged 39 to 93) with primary malignancies including squamous cell carcinoma (face or tongue), Merkel’s cell carcinoma (neck), lung adenocarcinoma, cholangiocarcinoma, colorectal cancer, and gastro-esophageal junction carcinoma. Some participants had nonmalignant pathologies contributing to nociceptive, neuropathic, or mixed pain components of head and facial pain. Two participants did not complete the treatment; one deteriorated rapidly and one had an unsuccessful attempt, possibly due to a nasal obstruction.
The mean pain score was 5.7 before treatment. Thirteen patients reported significant reduction in pain scores, and 11 were pain-free at 30 minutes post application. While one patient had an increase in pain from baseline to follow-up (7 to 9), the average pain score decreased (7 to 5). Interestingly, one patient reported improvement (8 to 0) to chronic right arm neuropathic pain. Patient rated satisfaction, though initially high (with improvement of pain) post procedure, was lower after 24 hours. More than 50% (5 out of 9) of satisfied participants remained satisfied at 24 hours. This aligns with current evidence, although duration of action was less compared with other studies. 2 Factors that may contribute to lower satisfaction after 24 hours include short duration of effect of Lignocaine, 2 concurrence of opioid dependence and opioid use disorder, 3 and medication overuse headache. 4
Reported adverse events post procedure included mild transient paresthesia and stinging (n = 2), watery eyes (n = 2), and altered taste (n = 4), with no significant lasting adverse effects reported at 24 hours except for moderate altered taste (n = 1). This is consistent with reported safety and tolerability of the procedure, 2 and a possible advantage of using 2% Xylocaine viscous. Study limitations include the investigator’s implicit bias, patient susceptibility to perceived exaggerated benefits, placebo effect phenomenon, small sample size, limited follow-up and absence of a placebo control.
To conclude, SPG block appears a feasible treatment option for management of head and neck pain in selected palliative care patients—it is safe, patients are satisfied with it, and it improves symptoms. Further studies with a placebo control, and longer-term follow-up is warranted.