
Abstract
Background:
Palliative care delivery in oncology is challenging and referral practices vary widely. Standardized, needs-based screening and triage systems are essential to more effectively address patients’ palliative care needs.
Objective:
Assess the feasibility, acceptability, and appropriateness among patients with advanced solid cancers of using electronic patient-reported outcomes (ePROs) to screen for palliative care needs.
Design:
We developed a 13-item ePRO palliative care survey to assess multidimensional palliative care needs and conducted a pilot study (n = 25) of a palliative care screening intervention using ePRO monitoring and presentation of ePRO reports to a multidisciplinary care team. Feasibility was assessed through enrollment, retention, and ePRO adherence rates. Acceptability and appropriateness were evaluated through exit surveys of all participants and semistructured interviews of a subset of participants (n = 10).
Results:
From May 2022 to April 2023, 68% (25/37) of eligible patients consented and enrolled on the ePRO platform. Overall, 96% (22/23; 2 censored for death/hospice) of participants completed the study and 96% of participants met predefined ePRO adherence thresholds. Overall, 84% (21/25) of patients reported a severe response during the study period, of whom 95% (20/21) received supportive services during the study period. Patients found the ePRO palliative survey acceptable and appropriate. Qualitative interviews found patient-identified barriers to the intervention and areas for improvement.
Conclusions:
Screening patients for unmet palliative needs using ePRO monitoring is feasible, acceptable, and appropriate among patients, but more work is needed to understand the perspectives of diverse patients and how to integrate ePRO palliative care screening into clinical workflows.
Key Message
Electronic patient-reported outcomes monitoring to identify palliative care needs coupled with presentation to clinical teams to facilitate palliative care delivery is feasible, acceptable, and appropriate. This approach should be further tested to evaluate the impact on palliative care use and downstream clinical outcomes in future studies.
Introduction
Early palliative care for patients with advanced cancer is an evidence-based practice that improves patient and caregiver outcomes, including patient-reported quality of life (QoL), symptom burden, and mood.1–6 Patients who receive early palliative care are also more likely to receive high-quality end-of-life care.1,7 Despite this evidence base, uptake of early palliative care in standard oncology practice has been difficult to implement, partly due to palliative care workforce shortages. 8 Rapid therapeutic advances in oncology have also changed the disease course of many poor prognosis cancers, effectively outpacing models of early palliative care delivery for patients with metastatic disease. 9
To address these challenges, the field has shifted toward tailored, patient-centered models of palliative care delivery that are scalable and more resource-efficient.10,11 These models focus on referring patients based on unmet needs or poor prognostic factors. Studies of automatic or triggered referrals to palliative care based on electronic health record (EHR) data have shown efficacy in increasing referral rates.12–14 However, these models are limited by low specificity for unmet needs reported directly by patients, high opt-out rates, and potential disengagement of the oncology team with palliative care management. 15 Another promising approach is stepped models of palliative care, in which patients are systematically monitored for unmet needs and palliative care treatment is increased for those who do not benefit from less intensive therapy. Recent data from stepped models of palliative care demonstrate a strong signal for using patient-reported outcomes (PROs) to identify those who require more intensive specialty palliative care.9,16,17
Remote symptom monitoring (RSM) is an electronic PRO (ePRO) intervention rapidly expanding in oncology practice driven by strong data that patients directly reporting symptoms improves care quality and patient outcomes.18–23 RSM provides the infrastructure and opportunity to link palliative care screening and service delivery into oncology workflows, yet it has not been well tested for monitoring palliative care needs and facilitating multidisciplinary management. 24 Furthermore, it remains unknown how to best deliver patient-reported information to clinicians and use PRO data to navigate patients to palliative care services. We sought to address this knowledge gap by testing a novel PRO screening strategy designed to engage patients and clinical teams in ePRO monitoring of palliative care needs.
In this work, we report the pilot testing of a novel 13-item ePRO palliative care survey developed to screen patients for multidimensional palliative care needs. We assessed feasibility and patient perceptions of acceptability and appropriateness of the intervention, which consisted of ePRO monitoring using the ePRO palliative care survey in combination with RSM and presentation of ePRO reports to a multidisciplinary team to facilitate palliative care.
Methods
Study design, setting, and participants
We conducted a single-arm pilot trial designed to assess the feasibility, acceptability, and appropriateness of ePRO palliative care screening in combination with RSM. From May 9, 2022, through April 18, 2023, we enrolled patients at the University of Texas (UT) Austin breast, gynecological, and gastrointestinal oncology clinics. Eligible patients were adults (≥18 years) with a diagnosis of locally advanced unresectable or metastatic solid cancer, receiving active cancer-directed therapy, and a provider-assessed prognosis of >6 months. Patients were required to complete surveys in English. Those on clinical trials requiring structured symptom reporting were excluded. Patients were not excluded based on prior palliative care receipt.
Trained study staff reviewed patient charts and eligibility weekly with oncology providers before approaching potential participants. Patients provided written informed consent, completed baseline measures, and enrolled on a third-party web-based RSM platform for 12 weeks. Enrollment required baseline PRO survey completion. Time on the study was extended if patients paused for hospitalization. Participants completed study end measures within 30 days of study end. We sought anecdotal feedback from clinic providers and staff at monthly team meetings and adjusted workflows based on their recommendations. We purposively sampled participants (n = 10) for exit interviews to assess the perceived acceptability and appropriateness of the ePRO monitoring intervention. Patients were compensated $50 for study completion and $25 for the end-of-study interview. The study protocol was approved by the UT Austin Institutional Review Board (IRB) and Advarra, the central IRB for the third-party RSM platform.
ePRO palliative care screening intervention
Development
We developed an ePRO item set to screen patients for multidimensional palliative care needs for use with weekly symptom monitoring in ambulatory oncology settings. Using a rigorous, evidence-based approach,25–31 we identified key domains for ePRO monitoring of palliative care needs in patients with advanced cancer and used expert input from clinicians, researchers, patients, and caregivers to select the final PRO item set (Supplementary Data). Given the screening tool is designed to integrate with RSM workflows, we chose individual PRO items from validated measures and prioritized a short set of items to minimize the survey burden on patients and present data to oncology teams. The process resulted in a 13-item ePRO palliative care screening tool, that in conjunction with standard weekly symptom monitoring, screens for care needs in the following domains: physical symptoms, psychological, social support, spiritual/existential distress, caregiver burden, illness understanding, patient request for palliative care, and physical function (Supplementary Tables S1 and S2).32–39
Pilot testing
The intervention included monthly ePRO palliative care screening and weekly symptom monitoring, with ePRO reports presented to a multidisciplinary team to facilitate palliative care management. Patients received a brief introduction to palliative care from a trained research coordinator using a study flier and then enrolled on the RSM platform. The ePRO assessment schedule consisted of multidimensional care needs screening with the 13-item ePRO palliative survey on weeks 0, 4, 8, and 12, and symptom monitoring using the PRO version of the Common Terminology Criteria for Adverse Events (PRO-CTCAEs) weekly on weeks 0–12 per emerging standard of care.18–20,40 The platform generated automated alerts for moderate and severe PRO-CTCAE reports directed to nurse triage. Monthly ePRO palliative surveys were manually reviewed by the study coordinator and PI for severe responses. PRO responses were presented at a weekly interdisciplinary team meeting attended by a palliative care advanced practice provider (APP), oncology APP, psychiatrist, social worker, and dietician. After a lead-in period and feedback from oncology physicians, this process transitioned to secure emails to oncology and palliative care MD/APP teams, highlighting severe responses and changes from prior surveys. PRO responses were managed by oncology and palliative care teams per usual care. We adjusted workflows based on feedback from clinic providers and staff.
Study measures
Sociodemographic and clinical characteristics
Participants completed a baseline survey derived from the PRAPARE assessment tool, 36 capturing sociodemographic data and social determinants of health. Age, sex, tumor type, stage, and palliative care receipt were obtained from the EHR.
Quality of life
Participants self-reported QoL at baseline and study end using the Functional Assessment of Cancer Therapy–General (FACT-G), a validated instrument for adults with cancer and a common outcome measure in palliative care studies.41,42
Feasibility
Feasibility was assessed through (1) enrollment (proportion of eligible patients who enrolled on the ePRO platform), (2) study retention (proportion of patients completing the FACT-G at study end), and (3) ePRO adherence rates.
Acceptability and appropriateness
We administered study end surveys to all participants composed of the Acceptability of Intervention Measure (AIM), Intervention Appropriateness Measure (IAM), and open-ended questions regarding what participants liked or disliked, suggested changes, additional symptoms, and general feedback. 43
Statistical analyses
The primary endpoint was feasibility, defined as ≥55% enrollment rate, ≥70% study retention, and ≥70% ePRO survey adherence.42,44 ePRO palliative survey adherence was defined as completing three of four monthly surveys. PRO-CTCAE survey adherence was defined as completing at least two weekly surveys during each month of study. Feasibility targets considered the serious illness of the patient population. Patients were censored for death or hospice enrollment and considered lost to follow-up if they didn’t complete an ePRO survey for six consecutive weeks. 45
Qualitative analyses
Semistructured interviews (n = 10) were conducted with purposively sampled study participants aiming for variation in age, sex, ethnicity, race, and tumor type. Guided by Proctor’s Implementation Framework, an interview guide was developed to assess the acceptability and appropriateness of using ePRO monitoring for palliative care needs and elicit feedback on PRO items. 46 Interviews were conducted by JS in-person or via virtual conferencing software (e.g., Zoom, Microsoft Teams) and lasted approximately 45–60 minutes. All interviews were audio-recorded and transcribed verbatim.
We conducted a rigorous thematic analysis and manually coded all transcripts. A codebook was developed based on open-reading of selected interview transcripts (Supplementary Table S3). The codebook included both a priori and emergent codes. 45 After finalizing the codebook, two members (C.S. and T.L.K.) of the study team jointly coded a shared selection of transcripts (20% of sample) to evaluate the codebook’s suitability. Coding and evaluating interrater reliability (IRR) were facilitated by NVivo software (Version 12). We used the Kappa coefficient to assess IRR between coders. 47 After resolving discrepancies through team discussions, we determined IRR to be acceptable and approved the codebook for application to the full study sample (Kappa: mean = 0.79, median = 0.92). An anthropologist (M.K.) and sociologist (D.C.) trained study team members and provided oversight for qualitative methods.
Results
Participant characteristics
Table 1 displays baseline characteristics of the study population (n = 25). Patients had a median age of 54 years (range 29–77) and most were female (68%), married/partnered (72%), insured (84% commercial or Medicare), and well-educated. Overall, 32% of patients self-reported an Eastern Cooperative Oncology Group performance status 2–3. Ten participants were already receiving palliative care, defined as a visit within 120 days of enrollment with a palliative care team member. Baseline mean FACT-G score was 74.7 (standard deviation [SD] 17.5). 48
Baseline Characteristic of the Study Population
Gynecological includes ovarian (1), endometrial (3), and cervical (1).
ECOG, Eastern Cooperative Oncology Group; FACT-G, Functional Assessment of Cancer Therapy–General; SD, standard deviation.
Feasibility
We screened every patient in clinic during the study period (n = 275) to identify 82 patients with locally advanced or metastatic cancer, of whom 37 were eligible for recruitment (Fig. 1). We approached all 37 eligible patients and obtained informed consent from 78% (29/37), of whom 68% (25/37) enrolled on the ePRO platform. The most common reasons for refusal were not enough time and not interested. Overall, 96% (23/24) of patients met predefined ePRO adherence thresholds for both the weekly and monthly PRO surveys, and survey compliance exceeded 83% at all time points in study (Supplementary Figs. S1 and Figs. S2). Study retention was high with 96% (22/23) of patients completing the FACT-G at the study end (mean score 76.3, SD 15.6). Two patients were censored for death or hospice enrollment.
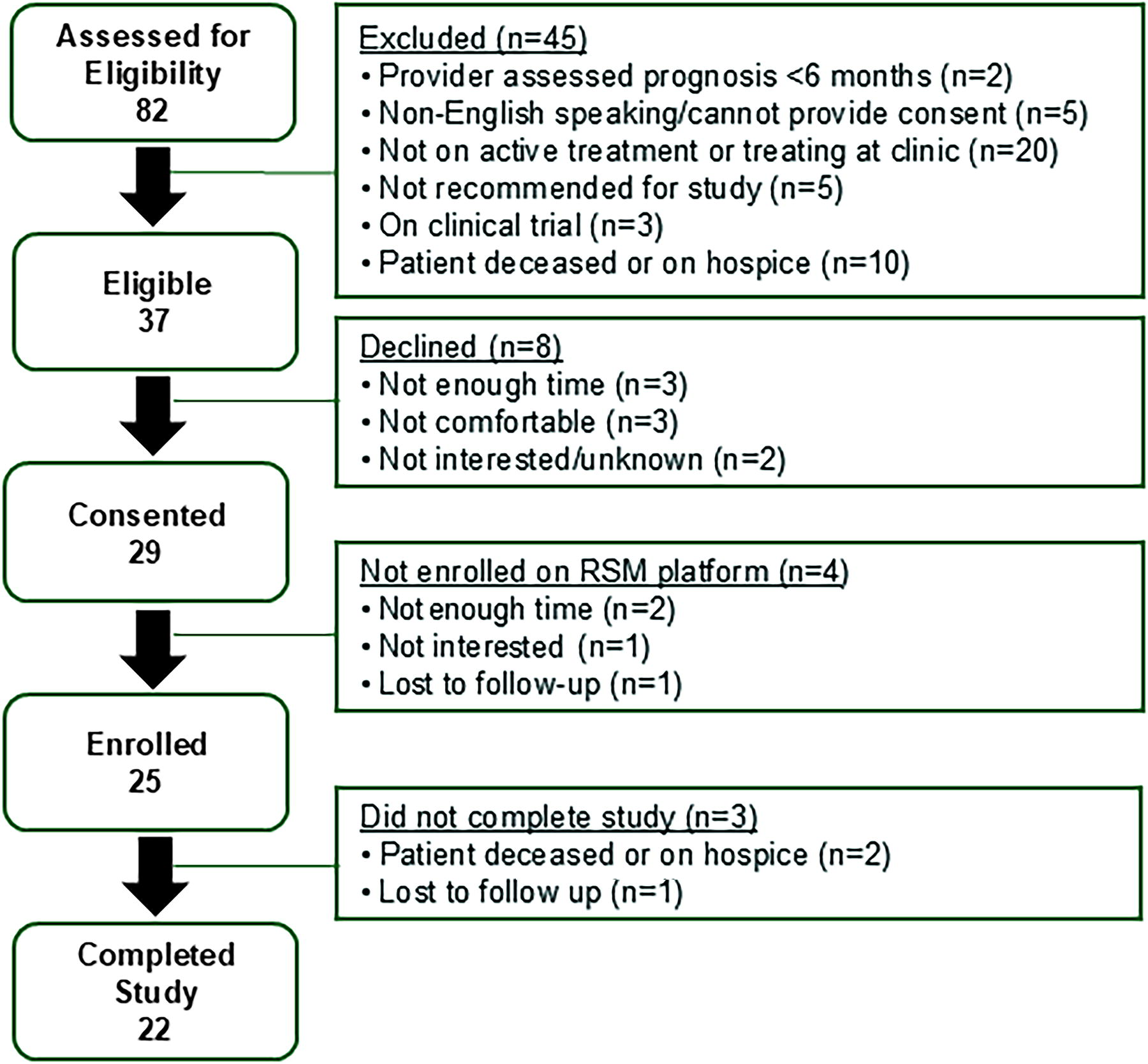
CONSORT diagram.
ePRO palliative care survey
Table 2 shows aggregate survey responses to the ePRO palliative care survey (n = 93) and clinically determined thresholds for severe responses. The distribution of patients with severe responses at each survey time point and in aggregate are shown in Figure 2 and Supplementary Figure S3, respectively. 84% (21/25) of patients reported a severe response during the study period, of whom 10 were already established with palliative care and 10 received a new palliative care referral. Of the four patients who never received palliative care during the study, three had no severe responses on the palliative care survey and one had severe responses but declined referral.
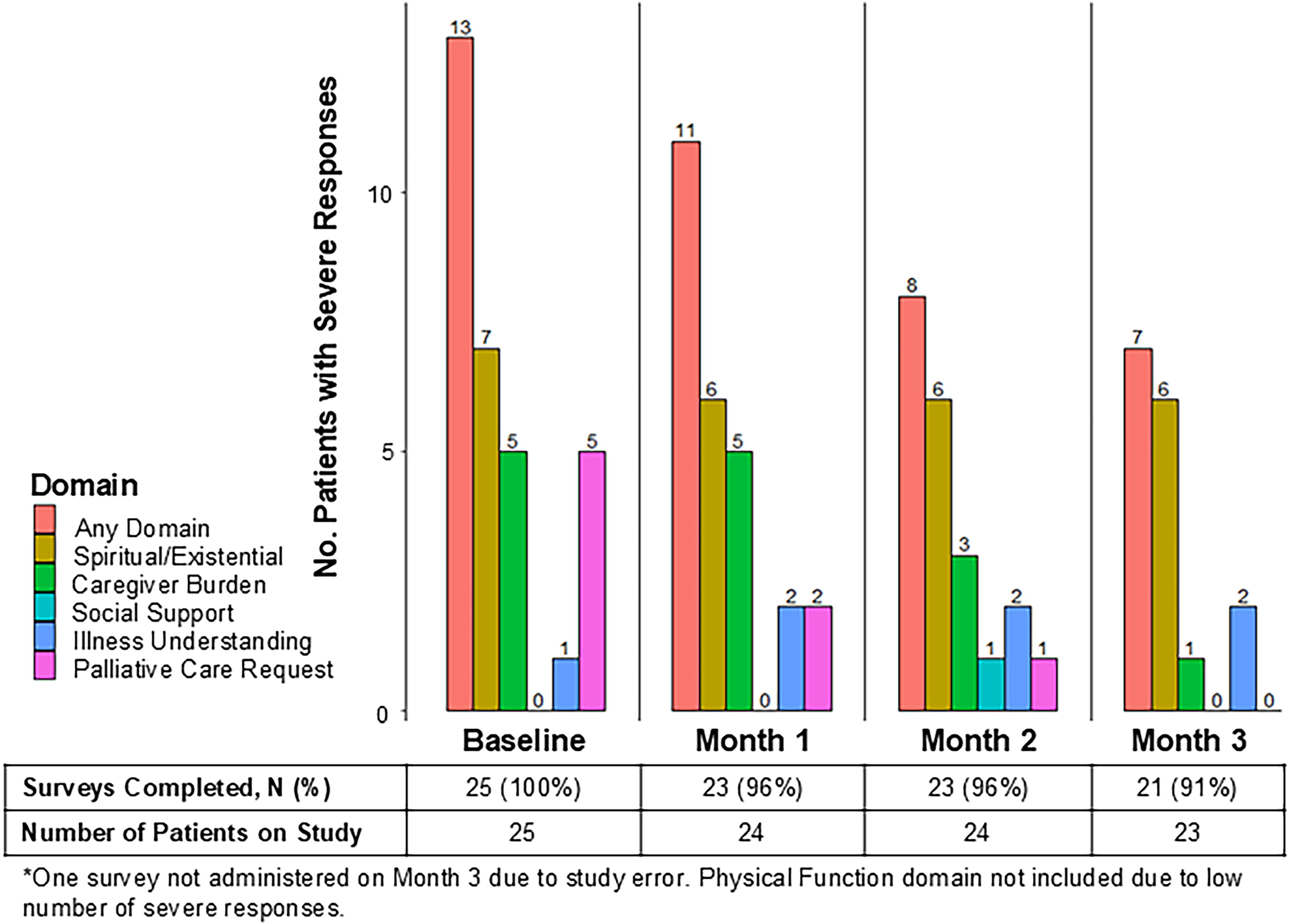
Severe responses on the ePRO palliative survey. Prevalence of patients with severe responses on the monthly ePRO palliative survey at each survey time point. The figure displays severe responses overall and by domain type to show the volume of alerts and characterize which domains generated alerts. ePRO, electronic patient-reported outcome.
Electronic Patient-Reported Outcome Palliative Care Survey-Level Responses and Severe Response Thresholds
Bold value signifies severe responses for each PRO item.
PRO items abbreviated for length, see Supplementary Data for full question stem and response options.
Severe response thresholds determined by the research and clinical team prior to study start.
ECOG, Eastern Cooperative Oncology Group; PRO, patient-reported outcome.
Clinical team anecdotal feedback
Oncology providers reported that the ePRO palliative survey provided new information about patients’ unmet needs and the survey facilitated palliative care for patients, predominantly if a patient requested services using the ePRO survey. Palliative care providers reported the survey was useful for screening patients for care needs at the interdisciplinary team meeting as the clinical volume increased. Oncology physicians expressed difficulty reviewing the ePRO palliative survey responses and recommended integration into the EHR with visual displays prior to routine clinical implementation.
Acceptability and appropriateness
Exit surveys
Supplementary Table S4 presents responses to the AIM and IAM surveys (n = 23). Mean acceptability scores were 3.92 (range: 3.25–5) and appropriateness scores were 4.26 (range: 3.25–5) out of best possible score 5. Patients gave more neutral ratings for acceptability compared with appropriateness, particularly for the responses “I like the symptom survey” (35% neither agree/disagree) and “the symptom survey is appealing to me” (39% neither agree/disagree). Patients indicated they would like an open-ended question allowing them to report “anything else you would like your care team to know” to allow for further open-ended communication with the oncology team during treatment.
Patient interviews
Overall, 77% (17/22) of patients who completed the study consented to an exit interview, of whom 10 patients were purposively sampled. Table 3 presents acceptability and appropriateness themes regarding ePRO monitoring of palliative care needs with representative quotes. Comments illustrate the survey’s effectiveness in encouraging participants to reflect on their needs during treatment, plan for the future, and foster a sense of connection with the oncology team. Patients underscored the survey’s effectiveness in normalizing the serious illness experience and introducing the concept of palliative care. Some participants reported that they found it confusing to receive an additional survey monthly and suggested better clarification of the survey schedule at the start of the intervention. Table 4 presents patient perspectives on barriers to the intervention and suggestions for improvement. Comments illustrate the challenges some participants faced with certain survey questions, particularly those related to the unpredictability of treatment outcomes, a lack of understanding about palliative care, and the relevance of questions to their personal treatment experience. Some patients did not understand how their responses were used by the care team. Participants also discussed the importance of customization to improve the survey experience.
Acceptability and Appropriateness Themes Regarding Electronic Patient-Reported Outcome Monitoring of Palliative Care Needs
Patient Perspectives on Barriers to and Areas of Improvement for the Intervention
Discussion
We developed and pilot-tested an intervention designed to engage oncology and palliative care teams in ePRO monitoring of palliative care needs. We learned that ePRO screening is feasible, as demonstrated by robust enrollment, retention, and adherence rates for the ePRO assessments, and is also appropriate and acceptable to patients. The ePRO assessment schedule, which included weekly symptom monitoring and a monthly palliative care survey, did not add a significant burden to patients, with similar adherence rates for both weekly and monthly ePRO completion. Patients and providers gave positive feedback regarding the intervention, especially regarding its impact on facilitating palliative care needs assessment, communication with the oncology team, and encouraging self-reflection on multidimensional domains of care. However, some patients reported lower acceptability for specific PRO items, particularly questions assessing more sensitive domains. Future research will refine the ePRO palliative care survey with attention to these domains and explore strategies to tailor the depth of assessment to patients’ treatment experiences.
Results from this study contribute to the emerging field of tailored palliative care delivery, in which patients are triaged to receive palliative care based on their reported needs. Recent work from Temel et al. demonstrated that using a decrement in patient-reported QoL scores and disease trajectory to trigger more intensive palliative care was noninferior to standard early palliative care for patients with advanced lung cancer and resulted in fewer palliative care visits. 9 This study provides evidence for using direct patient reports to guide palliative care intervention. However, implementing a longer QoL measure within ePRO monitoring may be challenging due to its length, particularly for patients with better prognosis cancers who require long-term monitoring. Furthermore, individual PRO item responses may offer more precision and actionable data for clinical management and triage. 11
To our knowledge, this is the first study of a multidimensional palliative care needs assessment operationalized with RSM workflows in oncology. Zimmerman et al. have demonstrated the feasibility of triggering automatic palliative care nurse calls based on symptom scores collected at the point of care, with confirmatory results from a larger trial pending.16,17 Their study uses the Edmonton Symptom Assessment System, which briefly assesses physical symptoms, anxiety, depression, and overall well-being but does not assess multidimensional care needs, such as spiritual/existential distress, caregiver burden, and illness understanding. 49 The optimal palliative care screening strategy is early in its development, and we expect ePRO screening tools will evolve over time based on many factors, including implementation considerations and advancements in PRO-based measurement of palliative care needs.
There are several advantages to using ePRO monitoring for tailored models of palliative care. First, PRO-based assessment integrates palliative care screening into oncology team workflows and provides a shared system for team-based triage. The oncology team may be able to address the issue for a patient, initiate referral to palliative care for complex cases, or refer to other ancillary services in resource-limited settings. Second, the ePRO survey facilitates patient engagement with palliative care during treatment which may overcome patient barriers to referral. We found in qualitative interviews that the ePRO palliative survey introduced palliative care to patients who had not heard of it before and helped patients anticipate multidimensional care needs that may develop during treatment. Third, ePRO palliative care screening is a resource-efficient solution for long-term monitoring of patients with better prognosis tumor types. As treatment options advance in oncology, patients will have longer and less predictable disease courses, which makes the scalability of longitudinal palliative assessments particularly critical as we build palliative care delivery systems for the future.
Our results contribute important findings to the field of developing scalable PRO-directed referral systems for specialty palliative care. Results from this study highlight the challenges of optimizing a general screening assessment for palliative care needs. Future work will incorporate more extensive supportive care education into the monitoring system to increase patient engagement with palliative care services. Future work should also focus on developing optimal referral systems, which should be tailored to institutional setting, culture, and available resources.
Limitations
There are limitations to this study. First, the pilot trial was conducted in a clinic setting that has a palliative care APP integrated within the care team. Future work should test ePRO palliative care screening in clinic settings with more barriers to palliative care access. Second, we did not formally assess acceptability and appropriateness among providers. Third, the patient population is highly educated and English-speaking, which does not inform use of the PRO item set among more diverse patient populations. Fourth, the sample size is relatively small given the large number screened for enrollment, demonstrating the challenges of recruiting patients with serious illness.
Conclusions
Our pilot results suggest that ePRO palliative care screening is highly feasible. Refining the ePRO survey items and offering customization options could enhance acceptability and support the sustainability of ePRO monitoring for palliative care needs throughout treatment. Further testing in diverse patient populations and clinic settings is needed to determine how best to implement alerts and link severe responses to team-based triage.
Footnotes
Acknowledgments
We are indebted to the patients who participated in the study. We gratefully acknowledge the contributions from the Patient and Family Advisory Council.
Author Disclosure Statement
G.B.R. received research funding from Genentech, Pfizer, and Daiichi Sankyo and consulting fees for Genentech, Pfizer, and Armada. A.M.S. received unrelated research funding from Pfizer Global, Sivan Innovation, and UroGen Pharma, Ltd.
Funding Information
T.L.K. is supported by an American Cancer Society Clinician Scientist Development Grant (CSDG-23-1019130-01-CTPS); G.B.R. receives funding through a National Institute of Nursing Research R01 grant (1R01NR019058-01). M.P. has received funding from the American Cancer Society. A.M.S. was partially supported for this project by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UM1TR004406.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.