
Abstract
Background:
Patients with severe and life-limiting illnesses transitioning out of the hospital often rely on family caregivers (FCGs) to manage communication with health care teams during hospitalizations and outpatient care. However, FCGs infrequently receive adequate training or support to prepare for these responsibilities. Effective communication between FCGs and health care teams is critical for preparing FCGs and reducing risks for poor outcomes. This study tested an eight-week intervention to improve FCG preparedness and communication practices during transitions out of the hospital.
Methods:
Conducted from 2018 to 2022, this randomized controlled trial included adult FCGs in rural areas in the United States (Minnesota, Wisconsin, and Iowa). FCGs caring for adults who received inpatient palliative care and were transitioning out of the hospital were eligible. The intervention group received teaching, guidance, and counseling from a palliative care nurse interventionist via video visits before and for eight weeks after discharge. The control group received monthly phone calls but no intervention. Outcomes included changes in FCG-reported preparedness for caregiving and communication with health care teams.
Results:
Of the 429 consented, 367 (183 intervention and 184 control participants) initiated the intervention; 164 had complete preparedness data, and 161 had complete communication data at baseline and eight weeks. In unadjusted analyses, the intervention group showed statistically significant improvements in preparedness but not communication practices. After adjusting for factors associated with care transitions, the findings persisted.
Conclusion:
Partnering rural FCGs with palliative care nurses via video can improve caregiver preparedness during care transitions. Improving communication practices may need more targeted strategies.
Key Message
Rural caregivers of people with life-limiting illness often face changes in responsibilities during transitions out of the hospital. Identifying and addressing unmet needs with video visits during the care transition can improve caregiver preparedness for these responsibilities, thus reducing their risk for poor outcomes associated with caregiving.
Introduction
People with severe, life-limiting illnesses face serious risks for adverse events, symptom escalation, emergency room visits, and hospital readmission when transitioning from the hospital to home or another care setting.1–5 Increased risks have multifaceted causes, including breakdowns in communication about discharge plans, medications, and addressing symptoms.6,7 Patients with complex needs are often too sick or cognitively impaired to fully manage their care during transitions,8,9 leaving family caregivers a (FCGs) responsible for communication with health care teams and ensuring patient safety and quality of care. 10 However, FCGs infrequently receive the training or post-discharge support for these responsibilities, 11 even though this preparation is likely a critical step toward preparing FCGs for their role and reducing the risks for poor patient (hereafter referred to as care recipients or CRs) and FCG outcomes. 12 Communication during care transitions is especially critical for FCGs in rural areas, where limited resources and access to care complicate the process.13,14
The duration of and responsibilities during the care transition phase can vary significantly depending on the complexity of the CR’s condition and health care settings involved. The transition phase can be more prolonged and complex for those with life-limiting illnesses and require significant coordination to execute the discharge care plan. Inpatient palliative care consultation can reduce symptom burden and improve quality of life,15,16 and extending this care through the transition out of the hospital can reduce hospital readmissions and acute care utilization and continue improvements in quality of life.17–19
We developed a transitional palliative care (TPC) intervention for rural FCGs to address unmet CR and FCG self-care needs during care transitions out of the hospital.8,20 Our previous results showed TPC significantly improved depression symptoms and quality of life for FCGs and quality of life and reduced hospital stays in the six months following hospital discharge for CRs.21,22 This study tested the hypothesis that change in caregiving preparedness and communication with health care teams during the intervention period would be significantly greater among FCGs in the TPC intervention compared with the attention control (AC) participants and that change in communication was necessary for improving preparedness.
Materials and Methods
Overview
Full details of the study and its protocol have been published elsewhere.20,22 The protocol was registered with ClinicalTrials.gov on November 13, 2017 (No. NCT03339271). The Institutional Review Board approved the study on October 30, 2017 (No. 17-005188). All FCGs and CRs provided informed consent before participation began.
Conceptual framework
Transition theory 23 posits that transitions are complex, multidimensional processes that create vulnerability in individuals lacking knowledge, support, or self-efficacy. Optimal transitions depend on the nature and conditions of the transition. We considered the nature of the transition to be determined by CR factors, such as transition types (e.g., curative to palliative care, transition out of the hospital), patterns (e.g., multiple, inter-related transitions occurring sequentially), and properties (e.g., discharge disposition, mortality risk, inpatient time exposed to palliative care) (Fig. 1). Transition conditions were considered to be FCG factors (e.g., available help, relationship quality, coping skills) that affect the ability to manage transitions. Modifying transition conditions through targeted interventions is expected to enhance outcomes associated with the transition. Our intervention combined objectives of both transitional 24 and palliative care 18 and used teaching, guidance, and counseling to modify FCG preparedness and communication skills with health care teams.
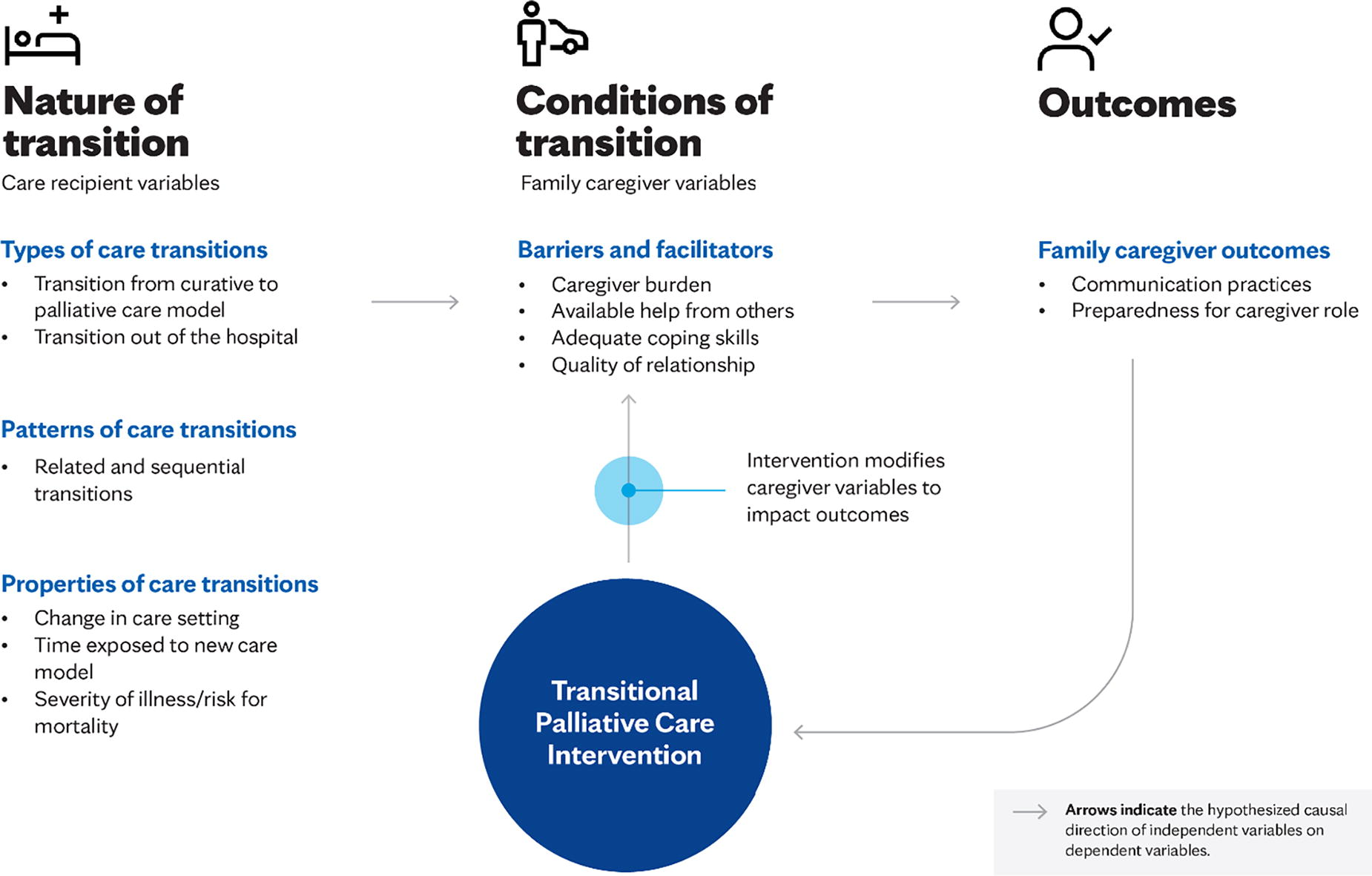
Transition theory used to conceptualize the function of a transitional palliative care intervention on family caregiver outcomes.
Design
We conducted a randomized controlled trial (RCT) to test the TPC intervention. FCGs were recruited after their hospitalized CR received a palliative care consultation in one of four participating hospitals (two academic health center hospitals and two community hospitals, all within the same health system). Recruited FCG participants were randomized into TPC or an AC arm using a computer-generated randomization list. 25
Participants
Figure 2 is the study’s CONSORT diagram. Enrollment ran from March 2018 to January 2022. Eligible FCGs were ≥21 years, spoke English, lived in an area in Minnesota, Wisconsin, or Iowa designated as rural (<50,000 people), 26 and cared for someone transitioning home or to a rehabilitation/short-term nursing facility before transitioning home. FCGs of CRs who died in the hospital or transferred to another hospital, had a left ventricular assist device, documented uncontrolled chronic pain, use of home infusion pain pumps, or active substance use were not eligible.
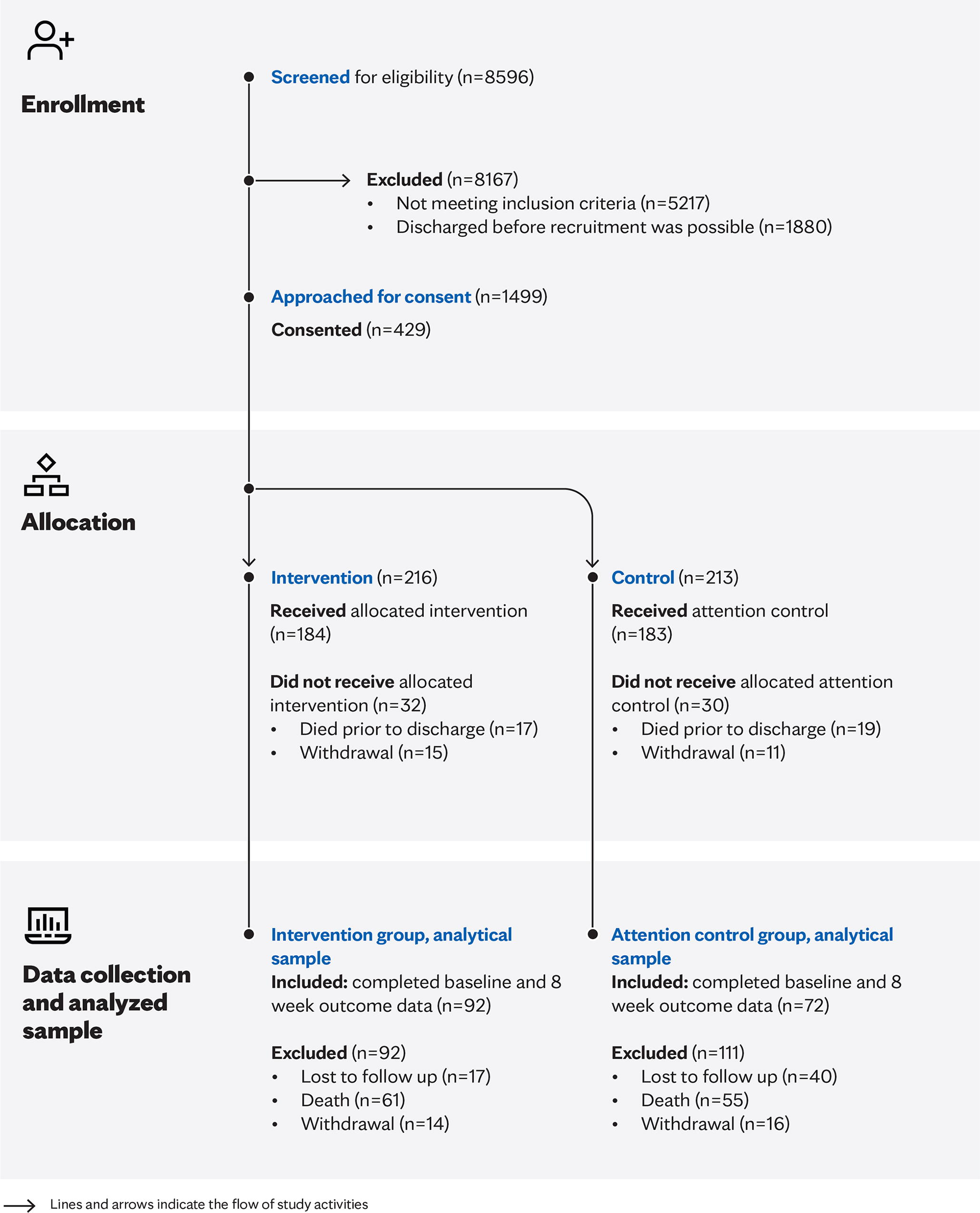
The Consolidated Standards of Reporting Trials (CONSORT) diagram.
Procedures
Daily reviews of inpatient palliative care consults were reviewed to assess eligible FCGs. When multiple caregivers qualified, the FCG who provided the most direct care was recruited. CRs were not directly engaged in the intervention, but consent or assent was obtained from them because data on their health and care were collected. CRs received usual hospital care regardless of FCG intervention condition, and hospital and palliative care staff were blinded to FCG assignment.
Intervention
TPC was a video-based, individually tailored intervention aimed at improving FCG self-efficacy in managing and negotiating care for themselves and the CR during care transitions and beyond. Two certified palliative care registered nurses were the study’s interventionists. They used teaching, guidance, and counseling during video visits to extend palliative care and address FCG unmet needs. The intervention began during the CR’s hospitalization and continued for eight weeks post-discharge, regardless of CR survival or hospice enrollment. The in-hospital component included a visit within 24 hours of enrollment and then up to twice-weekly visits with the FCG until CR’s discharge. Within 24–48 hours after the CR’s hospital discharge, an interventionist met with FCGs via video and then continued meeting at least twice a week for weeks 1–4 and once a week for weeks 5–8.
Interventionists partnered with FCGs to identify and develop a modifiable care plan to address the CR’s care requirements and FCG educational, emotional, spiritual, and social needs. Interventionists then provided corresponding teaching, guidance, and counseling to support FCGs. 27 They used a standardized assessment of needs that was reviewed at every visit.28,29 Unmet needs and corresponding actions were documented using a cloud-based electronic health record (EHR), (Nightingale Notes, Champ Software, Mankato, Minnesota, USA), allowing for intervention documentation independent of the CR’s EHR. The primary intention was to provide FCGs tools to prepare, manage, and negotiate care for themselves and the CR so that even those without specific communication or preparedness problems received support in managing CR symptoms and strategies in adjusting to the caregiver role.
Control
FCGs in the AC group received monthly phone calls from a team member to gather data on care-related costs 21 and provide some attention to the FCG to reduce attrition.
Fidelity
Fidelity assessment details are described elsewhere. 22 First, video visits were randomly sampled to assess the interventionist’s adherence to the protocol. Second, charted documentation was reviewed by study team members (D.E.H. and C.E.V.) to assess participant adherence to the number of scheduled visits (i.e., dose) and the mode of visits (i.e., video versus another modality).
Data collection and instruments
Study data were collected from March 2018 to July 2022. FCG data were collected at baseline (during the CR’s inpatient hospital stay), two and right weeks, with endpoint data collected approximately two weeks after the death, if applicable.30,31 Demographic data for the FCG and the CR were captured at baseline.
Outcomes
Endpoints were change in FCG caregiver preparedness and communication skills eight weeks after the CR’s initial hospital discharge. The Preparedness for Caregiving Scale32,33 assesses perceived readiness for different domains of caregiving, including physical care and emotional support. The scale has eight items using a 5-point Likert scale ranging from “not at all prepared” to “very well prepared.” Summed scale scores reflect the level of preparedness, with higher scores indicating greater preparedness. No specific guideline for missing responses was available, and therefore, missing items were replaced with the average score of the other completed items. FCG communication skills were assessed using the Communication with Physicians scale. 34 This 3-item scale includes questions on how often someone prepares lists of questions for the doctor, asks questions, and discusses personal problems, with six response options, ranging from “never” to “always.” Higher scores indicate better communication. Missing responses were handled using the published guidelines. 34
FCG and CR characteristics
Demographic factors for FCGs and CRs were captured at baseline. These included self-reported single questions on FCG/CR’s relationship, age, sex, education, marital status, race and ethnicity, and health insurance coverage.
Nature of the transition
CR’s condition and transition variables were extracted from the EHR. Variables included the discharge disposition, age-weighted Charlson Comorbidity Index (CCI) scores 35 derived from International Classification of Diseases, Tenth Revision, Clinical Modification codes, time from the inpatient palliative medicine consultation to the CR’s hospital discharge, and, to account for variations in CR severity of illness, a binary variable identifying those who survived (survived = 0) and those who died (died = 1) during the study period. CCI scores are used to predict mortality risk within one year of hospitalization. Scores range from 0 to 39, with scores ≥5 considered to be at risk for mortality. 36
Transition conditions
Factors that could influence FCG involvement during the transition, including FCG’s health status, hours per week they provided care, duration of caregiving prior to the hospitalization, care provided to others, if they lived with the CR, and the availability of help with caregiving, were evaluated. Also assessed were FCG coping mechanisms and the quality of the FCG-CR relationship. Coping at baseline was measured using one item from the Carer Support Needs Assessment Tool. Four response options were available, ranging from “no” to “very much more.” 37 The 15-item Bakas Caregiving Outcomes Scale-Revised was used to assess caregiver burden.38,39 Mean scores ranged from 1 to 7, with higher scores representing better FCG outcomes. The quality of the FCG-CR relationship was measured using the Mutuality Scale of the Family Care Inventory,32,33 with scores ranging 1–4, with higher scores indicating better relationship quality.
Statistical analyses
The analytic sample included 367 FCGs (183 control and 184 intervention). The total number of participants included 164 FCGs with complete change in preparedness (72 control, 92 intervention) and 161 FCGs with change in communication scores (69 control, 92 intervention). We had 80% power at 5% level of significance to detect a medium effect size of 0.44 standard deviations or larger for preparedness and 0.45 for communication practices. 40 Although we met our a priori recruitment goal, our analytical sample is smaller than planned for due to higher-than-anticipated loss to follow-up (i.e., nonresponse) and a higher rate of expected CR death prior to the eight-week assessment.
Associations of FCG and CR characteristics, the nature of the transition variables, conditions of the transition variables and outcomes were described descriptively using two sample t tests, Wilcoxon signed rank tests, or chi-square tests as appropriate.
We conducted a longitudinal, intention-to-treat analysis to assess changes in preparedness for caregiving and communication skills from baseline to eight weeks. For participants without baseline data for outcome variables, missing scores for this analysis were replaced using the last observation carried forward (i.e., data from assessments at two weeks), when available. Change in outcomes from baseline to eight weeks was analyzed using univariable and multivariable linear regression with intervention (yes, no) as the primary effect of interest. The multivariable model was adjusted for potential confounding variables significantly associated with the outcomes in bivariate analysis or included in the conceptual model (e.g., discharge disposition, relationship quality). All tests were two-sided, with p-values <0.05 considered statistically significant. The analysis was performed using SAS version 9.4 (SAS Inc., Cary, NC).
Results
Results on recruitment and retention efforts have been published elsewhere and are reported again in Table 1. Of 8596 CRs screened, 87% did not meet either the FCG or the CR study criteria (n = 8167). Fourteen percent refused to participate (n = 1070); however, 429 FCGs enrolled. Of the 429 consented, 215 were randomized into the TPC arm, and 214 were assigned to the AC arm. Thirty-six (8%) participants became ineligible after consent because the CR died in the hospital or was discharged to another hospital. Another 6% (n = 26) decided against participation prior to the CR’s hospital discharge. In all, 367 initiated the study, with 184 receiving TPC and 183 receiving AC. Nearly equal proportions of FCGs in the TPC and AC groups did not complete both baseline and 8-week endpoint data because they withdrew (TPC: n = 14, 7.6%; AC: n = 16, 8.7%), or the CRs died (TPC=n = 61, 33.2%; AC, n = 55, 30.1%) before the intervention’s completion. Loss to follow-up was significantly higher in the AC group (TPC: n = 17, 9.2% vs., AC: n = 40, 21.9%, p < 0.01).
Family Caregiver and Care Recipient Demographics
Missing CR data were augmented using electronic health record data.
Wilcoxon rank sum.
Chi-square.
CR, care recipient; FCG, family caregiver; SD, standard deviation.
Table 1 shows no statistically significant demographic differences between the TPC and AC arms, except for race. Although 94% of the sample was White (94%), statistically more FCGs in the AC compared with TPC were not White. Forty-one percent of CRs (n = 150) died after consenting to the study, with no significant difference in mortality between intervention conditions (p = 0.22).
No statistically significant differences were found between the TPC and AC arms in CCI, lengths of stay, or time between palliative care consult and discharge (Table 2). Mean baseline scores for caregiver burden differed statistically by arm, with the AC arm having significantly lower scores, but the mean difference was not clinically meaningful (0.1 on a 1–7 scale). No statistically significant differences were found between the groups at baseline for preparedness, but the AC group reported significantly greater communication skills than the intervention group at baseline (3.4 vs. 3.1; p = 0.03).
Baseline Scores for Nature of Transition, Transition Conditions and Outcomes by Intervention Conditions
Equal variance t test.
Wilcoxon rank.
Chi-square test.
BCOS-R, Bakas Caregiving Outcomes Scale-Revised; CSNAT, Carer Support Needs Assessment Tool.
In unadjusted analyses, TPC participants reported significantly greater change in preparedness for the caregiver role than AC participants (AC: 0.0; TPC: 0.3; p-value 0.005) (Table 3). After controlling for gender, age, relationship, relationship quality, availability of other help, death during the intervention period, coping, predischarge exposure to the intervention, and discharge disposition, preparedness among AC participants got worse over time and significantly improved among TPC participants (AC: −0.21; TPC: 0.09; p-value 0.004). In contrast, in unadjusted analyses, TPC participants did not have significantly greater change in communication skills than AC participants (AC: 0.7; TPC: 1.0; p value 0.25). After controlling for gender, age, relationship, relationship quality, availability of other help, death during the intervention period, coping, predischarge exposure, and discharge disposition, change in communication did not differ between TPC and AC participants (AC: 0.7; TPC: 0.86; p value 0.41). Because there was no significant change in communication by arm, additional analyses to assess if communication modified the relationship between intervention arm and preparedness were not necessary.
Unadjusted and Adjusted Changes in Scores for Study Outcomes between Baseline and Eight Weeks
Models adjusted for sex, age, relationship between FCG and CR, relationship quality (mutuality), provision of other help, coping, time from palliative care consult to hospital discharge, death during the intervention period, and discharge disposition.
Mean (SD).
Two-sample t test.
Discussion
Following the eight-week TPC intervention for rural FCGs, TPC participants were statistically better prepared for their caregiving role than AC participants, although communication skills with health care providers did not significantly differ between groups. Change in preparedness was not directly or indirectly attributable to changes in communication skills.
FCGs of palliative care patients often need more education to develop requisite knowledge and skills to provide optimal care to CRs,41–44 and better-prepared FCGs experience lower caregiver strain after CR hospitalization.33,45 Our findings suggest preparedness can be fostered through teaching, guidance, and counseling delivered via video throughout the transition period. By reassessing unmet needs throughout the intervention, FCGs learned to manage complex problems and address emerging issues during the transition course. The United States and other countries are facing a “family care gap,” with fewer FCGs available. Consequently, it is likely that in the future, fewer FCGs will be available and prepared for their caregiver role. 46 Even when FCGs are available, they are often unexpectedly thrust into their caregiving role due to a health care crisis or to compensate for deficiencies in available care delivery services. 47 Our study shows benefit and utility of using video technology to reach even remote-dwelling FCGs to help address preparedness, a concept that includes mastery, self-efficacy, competence, quality of care, and self-care.
Although preparedness was significantly different between intervention groups, the change in preparedness among the intervention group was relatively small, and to date there is no guidance on what proportion of change is clinically meaningful. It is reasonable, however, to consider that a clinically meaningful outcome is one that shows that caregivers became more prepared over time, and in our study, caregivers in the intervention group improved (albeit a small increment), while the AC group got worse over time. These findings are especially encouraging when considered together with the impact TPC has had on reductions in patient hospitalizations up to 6 months after hospital discharge 21 and benefits to health and well-being for FCGs and CRs. 22 With potential reimbursement strategies for TPC 48 coupled with newly approved billing codes to address caregiver training needs,49–51 it is possible that previous barriers for integrating caregiver-focused interventions into palliative care practice are surmountable.
Effective communication during care transitions includes sharing and exchanging information among all responsible for the CR’s care and care plan. Our findings suggest improving FCG communication skills may require more targeted communication strategies and refined assessments for determining optimal communication. TPC may not have significantly changed communication skills because the assessments used were adapted from CR to FCG communication with health care teams. Skills like preparing questions for the doctor, asking questions, and discussing personal problems are relevant skills used in shared-decision making 52 and advocacy training, strategies others have suggested are needed to promote communication between FCG needs to CR providers,53,54 but these strategies may be more suitable for chronic disease management than for shorter-term care transition needs for people with life-limiting illnesses. Interventionists, for example, may have helped FCG with skills to improve discussions about disease-directed care, palliative or goals of care, or death and dying for the CR but did not concentrate on identifying and promoting FCG self-care with providers. Refining assessments to determine appropriate and effective communication skills during care transitions is critical and may encourage greater engagement of FCG in CR care, which are priorities outlined in the National Strategy to Support FCGs 55 and in other studies.56,57
Interventions to change communication practices between FCGs and health care providers will likely require changes in provider practices. Providers are hesitant to address FCG unmet needs without protocols or resources for addressing them and, consequently, often avoid these conversations.58,59 More research is needed to develop acceptable and feasible provider communication interventions that they consider ethical and within their scope of practice.
Our study has several strengths. First, we included FCGs of CRs who received palliative care regardless of diagnoses, thus showing the intervention improved preparedness across various caregiving situations. Second, we had a higher proportion of male FCGs and younger CRs than typical in caregiving intervention studies, 60 yet outcomes did not vary by these characteristics, suggesting that our tailored approach improved preparedness across diverse groups of participants. Third, video visits could be effectively done among rural FCGs, thus providing an accessible and relatively low-cost intervention 48 to a population often facing a scarcity of services.
Our study has limitations. Although the percentage of CRs who died before completion of the intervention did not significantly differ across conditions, more data were missing among AC participants. Hence, outcomes may have been influenced by participant attrition or nonresponse before the conclusion of the trial. Recruitment and retention of FCGs is a known challenge, 61 and was a primary reason for including an AC condition instead of a standard control. Even with no active intervention delivered to AC participants during calls, however, the additional attention may have influenced outcomes. Moreover, we did not assess variation in care instructions, capacity, or willingness to provide care during discharge planning or the quality of discharge instructions. Although an RCT design should minimize variations in discharge quality, it remains possible.
Conclusions
Partnering rural FCGs with palliative care nurses and using tailored video interventions can improve caregiver preparedness during care transitions. This is critically important given the risks in care transitions among seriously ill patients. However, building FCG communication skills may require more targeted strategies for FCGs and providers. Research is needed to identify the most effective communication strategies associated with FCG preparedness and their impact on care transitions.
Footnotes
Authors’ Contributions
J.M.G.: Conceptualization, methodology, investigation, supervision, resources, writing—original draft, and writing—review and editing. B.G.K.: Methodology and writing—review and editing. C.E.V.: Conceptualization, methodology, investigation, and writing—review and editing. J.N.M.: Conceptualization, formal analysis, methodology, and writing—review and editing. W.S.H.: Formal analysis, writing—review and editing, and funding acquisition. A.M.G.: Methodology and writing—review and editing. C.I.: Writing—review and editing. E.M.W.: Data curation and writing—review and editing. A.M.D.: Data curation, and writing—review and editing. E.E.T.: Data curation and writing—review and editing. C.J.S.: Data curation and writing—review and editing. D.E.H.: Conceptualization, methodology, investigation, writing—review and editing, and funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
The study was supported by the National Institutes of Health, National Institute of Nursing Research (NIH-NINR R01NR016433).