
Abstract

Introduction
The Surprise Question (SQ), “Would I be surprised if this patient died in the next six months?” is a screening tool for identifying patients at or near the end of life. 1 In hospitals, it may help trigger early palliative care (PC) consultation, which can enhance alignment of care with patient goals, quality of life, and improved health care delivery efficiency. 2 We implemented the SQ in the emergency department (ED) of a large academic health system and assessed its impact on time to PC consult, hospital length of stay (LOS), and cost savings.
Methods
We conducted a retrospective cohort study of adults aged 18 and older admitted to a seven-hospital health system in the year before and after SQ implementation on May 30, 2023. The SQ was integrated into the ED workflow through the electronic health record (EHR), requiring clinicians to respond when admitting patients to the hospital. If the response was “No, I would not be surprised if the patient died in the next six months,” the EHR prompted a PC consult. Primary outcomes included time from admission to PC consultation and LOS. Cost analysis was based on a conservative estimate of $900 saved per hospital day.
Results
The cohort included 5346 patients who received a PC consult one year before SQ implementation and 6058 one year after. Following SQ implementation, the average time from admission to PC consult decreased by 1.1 days (5.7 to 4.6 days) Fig. 1. In addition, the average hospital LOS among the PC-consult cohort was reduced by 3.3 days (16.2 to 12.9 days) Fig. 1. Using a cost per day of $900, before the SQ, 5346 patients receiving a PC consult stayed an average of 16.2 days, totaling $77,944,680. After the SQ, 6058 patients stayed an average of 12.9 days, reducing total costs to $70,333,380. This represents a savings of $7,611,300, or approximately $1,256 in cost avoidance per patient referred to PC, driven by shorter hospital stays.
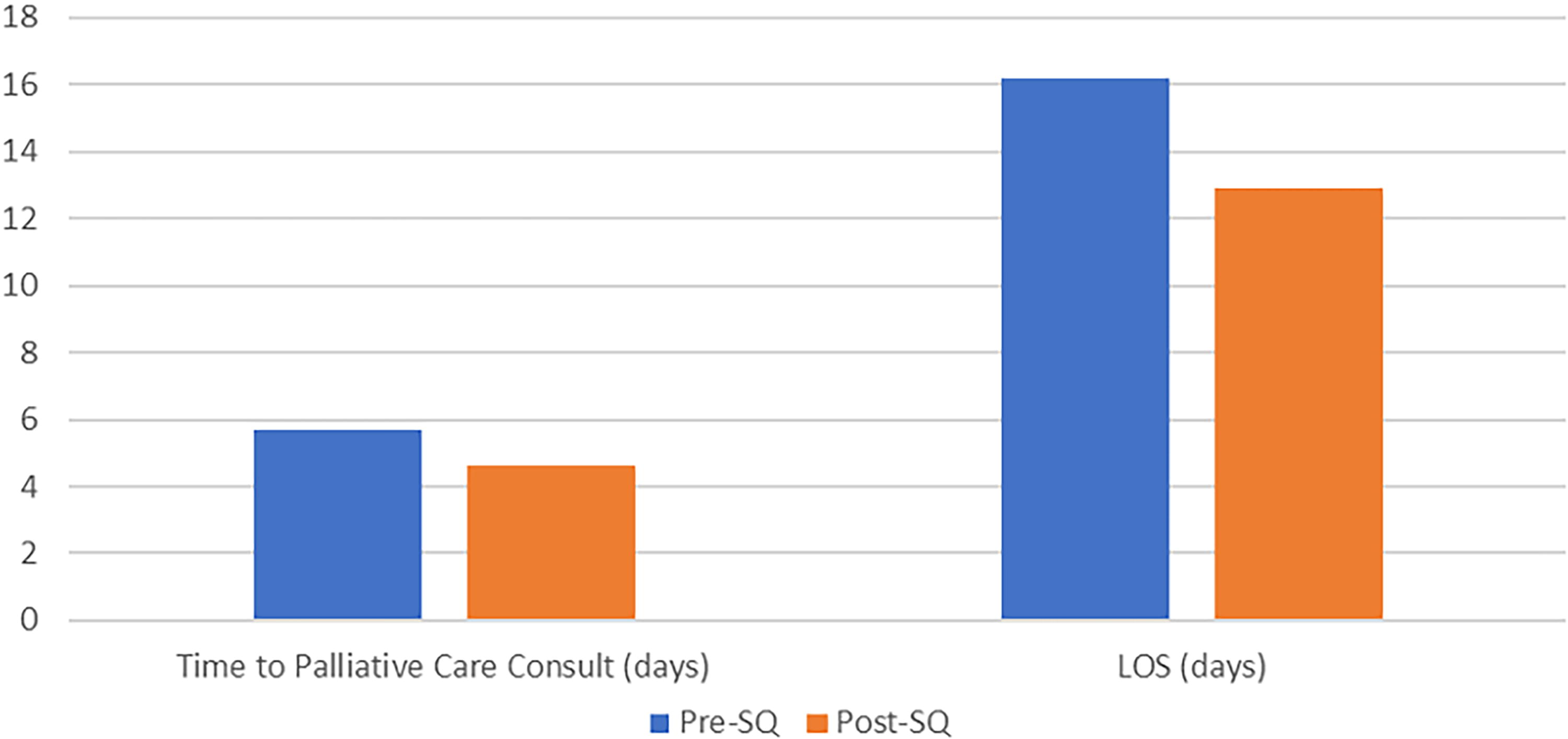
Impact of the Surprise Question on Time to Palliative Care Consult and Length of Stay.
Discussion
The SQ is an effective tool enabling early identification of patients who would benefit from PC, facilitating timely discussions of goals of care, symptom management, and potential hospice transitions. Our study shows that implementing the SQ in the ED reduces both time to PC consultation and hospital LOS, leading to meaningful financial savings. Notably, these results were achieved without increasing PC staffing, highlighting the cost-effectiveness of the SQ. We posit that earlier PC consults may have resulted in cases that were less complex with patients who had not yet received aggressive interventions that had to be withdrawn and families that had not heard multiple conflicting opinions from many different providers. This may in turn have increased the capacity of the existing PC workforce to see more patients. As such, our study adds to the burgeoning literature demonstrating that PC is cost-saving. 3
These findings are consistent with existing literature on early PC, which improves quality of life, reduces aggressive treatments, and lowers health care costs. 4 The reduction in hospital LOS supports the SQ’s role in optimizing hospital resources, which is important for institutions seeking to improve patient flow and reduce bed occupancy.
Conclusion
Implementing the SQ in the ED reduced time to PC consultation and hospital LOS, leading to an estimated cost savings of $1,256 per patient. Broad adoption can potentially improve end-of-life care and decrease health care costs, offering a practical tool for busy health systems.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.