
Abstract
Background:
The purpose of this study is to establish the scope of literature surrounding the concordance between patients and surrogates when making decisions about life-sustaining therapies in the perioperative setting. This review will lay the foundation for future studies and interventions optimizing perioperative concordance.
Methods:
To understand the performance of surrogates in the context of surgery and the potential for further studies and interventions, we performed a scoping review, according to Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines, of MEDLINE (Ovid SP), Embase (Elsevier), Web of Science Core Collection (Clarivate), and the Cumulative Index of Nursing and Allied Health Literature (EBSCO) for studies published before May 5, 2023.
Results:
A total of 18 records met inclusion criteria. Fifteen were removed because they included the wrong patient population (at least half the study patients were not surgical or article did not discuss patient–surrogate concordance) or were done in the wrong setting (not perioperative) leaving three studies for analysis.
Conclusions:
There is limited evidence surrounding the concordance of patients and surrogates in the perioperative settings and suggests an unmet need requiring further studies and intervention analysis. Recognition of this gap is important, as it may indicate that an assumption between surrogate and patient concordance may be incorrect, and studies demonstrating how to achieve concordance by piloting educational innovations are necessary.
Keywords
Introduction
Achieving high-quality surgical shared decision making requires delivering surgical care concordant with patient goals, which entails an understanding of patients’ priorities and integration of that information into real-time clinical decisions. 1 Since surgical patients may be unable to fully participate in choices about their care due to sedation and/or effects of surgery and postoperative trajectories, providers may need to rely on designated health care proxies or de facto surrogates to weigh competing priorities and guide clinical decisions.
This strategy rests on the assumption that proxies have unique insight into patients’ preferences; however, even during medical, nonoperative care the literature available indicates the concordance between patients and surrogates regarding medical decisions is poor. 1 A recent qualitative study done in China showed that there were multiple factors that could contribute to the lack of concordance, for example, when the patient’s health was relatively stable, the surrogates were reluctant to discuss patient preferences, which may impede the possibility of concordance between surrogates and patients. In addition, involvement of surrogates can be influenced by ethnic and cultural factors around surrogate and family involvement.2,3 The inadequacy of proxies’ perspectives in guiding goal-concordant care in medical patients has been attributed to limited knowledge of patients’ goals and preferences, complexity of the issues under consideration, interpersonal dynamics, unforeseen scenarios, and instability of treatment preferences over time.3,4 Such limitations may be of particular importance in the context of surgery, where patients’ trajectories are frequently nonlinear. For example, recovery from surgery may involve complications requiring temporary escalations of care or further procedures. Perioperative events and new diagnostic information may also result in an evolving calculus of what goals are realistically achievable. Proxy’s and provider’s knowledge of patient preferences is therefore an important basis for delivery of goal-concordant care and avoidance of unwanted treatment.
Understanding the performance of surrogates in the context of surgery and characterizing their alignment with patient values is necessary to guide interventions aimed at promoting goal-concordant surgical care. We therefore performed a review of the literature to establish the scope of evidence regarding the concordance between patients and surrogates regarding decisions about life-sustaining therapies in the context of surgery. We hypothesized that (1) there is not adequate information about the concordance of the health care proxy and patient around decision making in the perioperative setting and (2) there is limited information about education and implementation of a standardized format for health care proxies and surrogates to ensure concordance and help surrogates make the decisions their role requires. This scoping review has the potential to improve shared decision-making in advance care planning and the role of surrogates and providers. Furthermore, the results of this review will offer valuable insights that may serve as a foundation for future studies and interventions in this domain.
Materials and Methods
We performed a scoping review of the concordance of patients, proxies, and providers regarding life-sustaining therapies in the context of surgery. This scoping review was guided by methods reviewed by Peters et al. 5 The creation of this report was guided by the PRISMA-ScR extension for scoping reviews. 6 Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) was used to manage and screen results. As a scoping review, an institutional review board’s approval and informed consent were not part of the methodology.
We identified studies that examined the concordance of goals and decisions among patients, proxies, and providers regarding life-sustaining therapies in the context of surgery by searching the electronic databases MEDLINE (Ovid SP), Embase (Elsevier), Web of Science Core Collection (Clarivate), and the Cumulative Index of Nursing and Allied Health Literature (EBSCO). The search was designed and executed by a medical librarian (P.A.B.) and included controlled vocabulary terms when available (Supplementary Table A1).
No date limits were applied. Searches were carried out on May 5, 2023. Articles met inclusion criteria if they were in English, peer reviewed, included patients 18 years of age or older, and at least half of the study population were surgical patients (defined as patients who had or were undergoing surgery). Experimental, quasi-experimental, observational, metanalyses, and review articles were included.
Articles were excluded if they were clinical conference notes, comments, editorials, letters, or lectures. All articles meeting inclusion criteria were screened by title and abstract for relevance by two reviewers. Articles meeting inclusion criteria were reviewed in their entirety by three reviewers. Articles of uncertain relevance were reviewed by the senior authors prior to study inclusion. Assessment criteria included appropriateness of outcomes, patient population, study design, and setting. Specifically, outcomes focused on patients, proxies, and providers’ concordance regarding life-sustaining therapies in the context of surgery in the perioperative setting.
Results
Electronic database searching returned 734 unique records (Fig. 1). Of these, 716 records were deemed irrelevant and were removed. Of the remaining 18 records that were selected for full-text review, 15 were removed because they included the wrong patient population (n = 10) (at least half the study patients were not surgical, or article did not study patient–surrogate concordance) or were done in the wrong setting (n = 5) (setting was not perioperative). In the end, three studies were left for analysis.7–9 Details regarding study selection can be found in Figure 1.
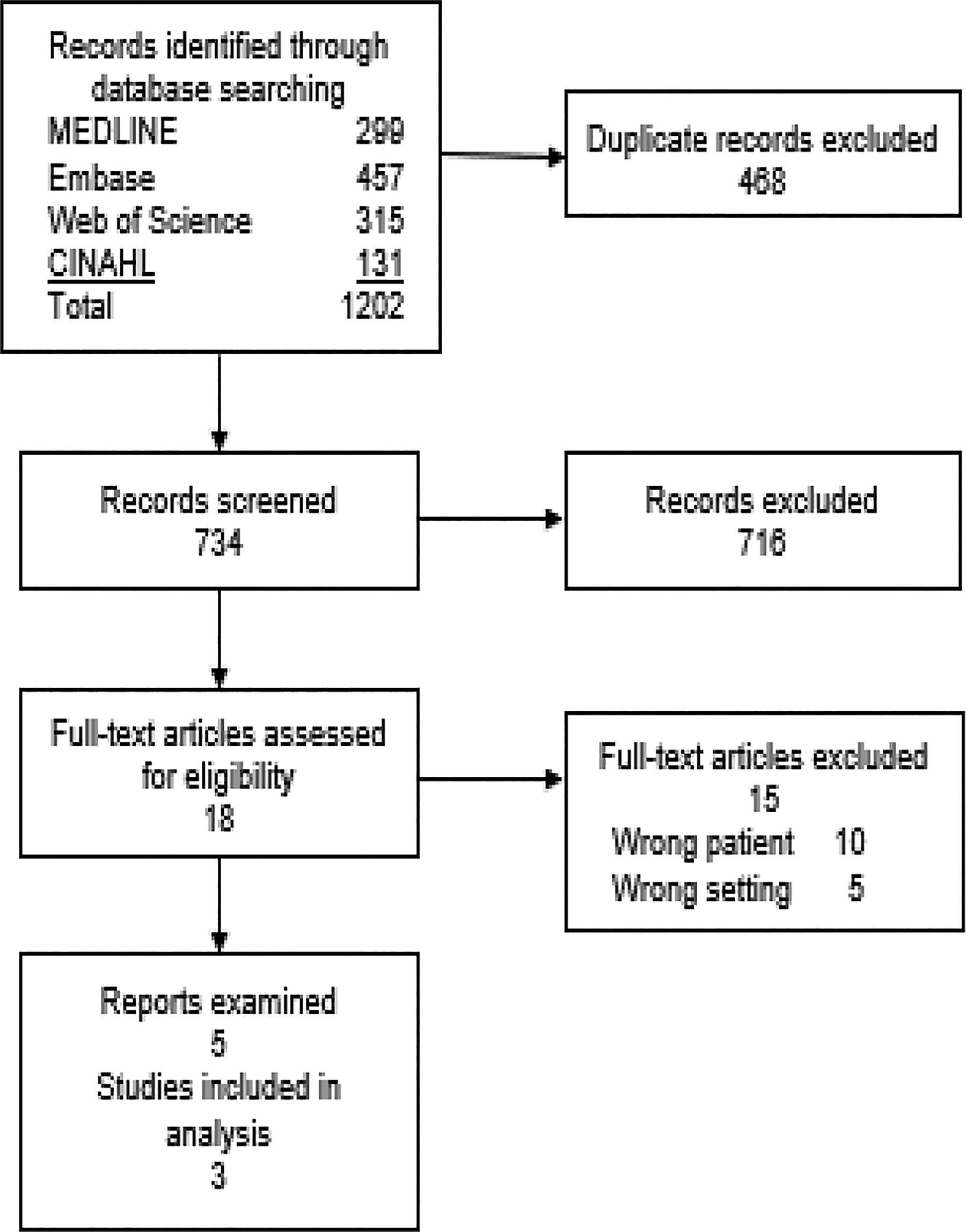
Selection of studies.
Study characteristics
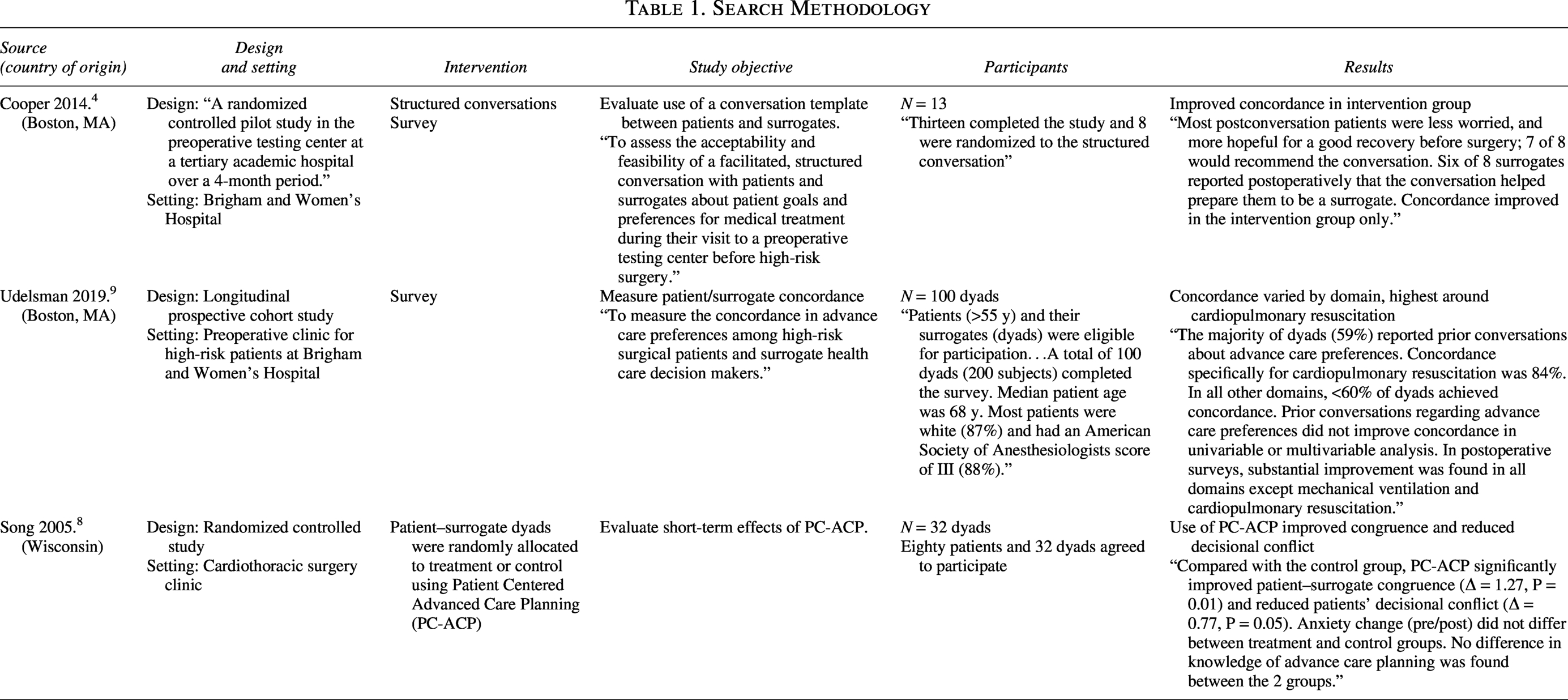
All publications were single-center studies performed at academic medical centers in the United States. Two studies involved interventions aimed at improving concordance between patients and surrogates.8,9 Specifically, Cooper et al. and Song et al. randomized patient–surrogate pairs to undergo structured interviews/conversations designed to explore goals and values guiding treatment compared with usual care.
Participants
The overall number of participants was 258 (129 patients and 129 surrogates). The sample sizes in the three studies were 26, 32, and 200. One publication focused specifically on patients undergoing cardiac surgery and their surrogates, 9 while another focused on patients undergoing general, vascular, or cardiothoracic surgery with planned admission to the intensive care unit (ICU) postoperatively. 8 The third included patients aged ≥55 years undergoing in-person preoperative evaluation for surgery of any type. 10
The overwhelming majority of participants were white (100% in Cooper et al. and 87.5% in Udelsman et al.) and non-Hispanic (92.3% in Cooper et al. and 87.5% in Udelsman et al.). Characterization of education level was heterogenous, but 73% in Cooper et al.’s cohort had more than a high school education, 94% in Song et al.’s cohort had at least a high school education, and 50% of Udelsman et al.’s cohort had a college degree. All were English-speaking.
Decision content
Decision content differed between the studies. While Song et al. and Cooper et al. evaluated decisions regarding continuation or discontinuation of treatment in scenarios with varying chances of survival, invasiveness of treatment, disability, and burden of care, Udelsman et al. elicited decisions regarding use of specific life-sustaining therapies (cardiopulmonary resuscitation, mechanical ventilation, hemodialysis, and artificial nutrition), as well as tolerability of specific health states (physical disability, cognitive disability, and severe pain). Udelsman et al.’s survey elicited decisions regarding life-sustaining therapies without defining likelihood of success or untoward outcomes.
Interventions
Two of the studies examined interventions intended to improve surrogates’ level of preparedness for their role. Song et al. evaluated Patient-Centered Advance Care Planning (PC-ACP), a structured interview based on the Representational Approach to Patient Education. This intervention included exploration of patients’ experience of illness, concerns related to medical decision-making, and presentation of a document describing potential complications and decisions a surrogate may face. The PC-ACP was delivered by a trained nurse facilitator and lasted between 20 and 45 minutes. Cooper et al. developed a structured conversation guide incorporating expert opinion from surgeons, intensivists, anesthesiologists, psychiatrists, and palliative care specialists. The guide spanned multiple domains including expectations for outcomes of surgery, worries about recovery, health states that the patient would deem unacceptable, and anticipation of need for temporary escalations in care (“If you become sicker, how much are you willing to go through for the possibility of living longer?”). The guide also encouraged further discussion with the surrogate and emphasized the key purpose of the conversation was to help surrogates prepare. These conversations were led by palliative care specialists and their duration was not reported.
Concordance
Concordance between patients and surrogates was the primary outcome of interest in all studies. No studies evaluated concordance between providers and patients. For decisions to discontinue treatment, Song et al. found baseline concordance of 38% in a scenario of low survival probability/high burden of care and 44% in a scenario of high survival probability/permanent disability/high burden of care. In Cooper et al.’s cohort, baseline concordance was 78% for a scenario of low survival probability/highly invasive treatment, 67% for a scenario of high survival probability/permanent disability/high burden of care and 75% for a scenario of high survival probability/permanent severe brain damage.
The two interventional studies yielded conflicting results with respect to concordance. While Song et al. observed a statistically significant difference in concordance between the intervention arm and the control arm (81% of intervention dyads achieved complete congruence versus 19% in the control arm), Cooper et al. observed differences between intervention and control dyads, with both intervention and control dyads demonstrating improvement in two of three scenarios (intervention dyads demonstrated no difference in concordance regarding the scenario describing low survival and invasive medical procedures, while control dyads demonstrated decreased concordance in this setting).
In Udelsman et al.’s cohort, concordance regarding cardiopulmonary resuscitation was 84%, while concordance for intubation, hemodialysis, and artificial nutrition ranged from 46% to 51%. When considering tolerability of specific health states, patients and surrogates agreed in 57% of cases regarding physical disability, 48% for cognitive disability, and 42% regarding severe pain. Only 11% of dyads demonstrated concordance across all domains studied. In cases of lack of concordance, surrogates tended to opt for more invasive treatment. No factors were consistently associated with high levels of concordance, including prior conversations regarding advance care planning. Interestingly, only 59% of dyads agreed on whether a conversation on LST had occurred.
None of the three studies evaluated concordance between patients and providers regarding LST in the perioperative period.
Other outcomes
In addition to congruence, Song et al. assessed anxiety, decisional conflict, and knowledge of ACP using the Spielberger’s State Anxiety Inventory, Decisional Conflict Scale, and an investigator-developed questionnaire, respectively. Cooper et al. elicited self-reported levels of worry about surgery and about making decisions (both patient worry about surrogate making decisions and surrogate worry about making decisions).
Song et al.’s study demonstrated a statistically significant decrease in decisional conflict in the intervention arm. They observed no changes in knowledge of ACP or anxiety. In Cooper et al.’s study, six of eight surrogates reported that the conversation helped prepare them as a surrogate. Thirty-seven and a half percent of participants reported that the conversation made them less worried about the surgery and 12.5% (one participant) reported that the conversation left them more worried. In terms of worry about decision making, most patients reported no change in worry about surrogates making a medical decision (87.5%). Likewise, most surrogates (60%) reported no change in worry about making a medical decision for the patient, while 40% reported an increase in worry about this.
Neither of the interventional studies formally assessed feasibility of the structured interview tools that were used.
Discussion
In this scoping review, we synthesized studies on concordance between patients and surrogates regarding the use of LST in the context of surgery. We identified only three studies including a total of 258 patients and surrogates (of whom only 58 were the target of interventions). Concordance and congruence were measured and the Song study included related outcome measures such as decisional conflict and decisional regret, more detailed outcomes for each are included in (Table 1). Of note, none of these studies examined the relationship between the providers and patient–surrogate dyads.
Surrogates for patients undergoing surgery face unique challenges requiring dedicated study. The clinical status of surgical patients may change rapidly in the setting of surgery and anesthesia and can include a wide variety of perioperative complications. In addition, surgery and anesthesia entail periods of patient incapacity, necessitating surrogate decision making. As noted by Lilley et al., previously realistic goals may suddenly become unattainable and new decisions may exceed surrogates’ level of understanding of patients’ preferences. 10 These challenges may be associated with unique stresses and untoward outcomes for surrogates.11–12 Understanding how best to prepare and support surrogate decision makers in the context of surgery and postsurgical intensive care therefore remains a research priority.
Interventional studies examining concordance regarding use of LST in this population had a small sample size. Although investigators observed some benefits including increased concordance, decreased decisional conflict, and decreased worry, the findings were not consistent and sample sizes were too small to support conclusions as to whether they merit implementation. Future studies should evaluate the use of ACP intervention modalities and outcomes in surgical populations using the ACP Outcomes Framework created in 2017. 13 In a scoping review from 2021 looking at ACP interventions including facilitated discussions, video-only, interactive, multimedia/multimodal online or educational programs, written-only materials, and clinician training for physicians, nurses, or nursing home staff, it was found that the most positive results came from written materials-only and multimedia programs with facilitated discussions to a lesser degree. 14 However, the settings in which these interventions were done spanned from primary care, oncology patients, and patients with COPD, so it would be helpful to investigate the effectiveness of these interventions in patient–surrogate dyads in the context of surgery.
It is also important to note that the studies span an increasingly relevant distinction between traditional ACP and serious illness communication. ACP is a goal-oriented care that aims to elicit the values, goals, and preferences regarding future potential medical care decisions and interventions like resuscitation and mechanical ventilation. It has been argued that this has failed to achieve its goal due to the gap between hypothetical scenarios and the decision-making process, which has led to a shift to serious illness communication.15,16 Serious illness communication tries to foster a conversation about health goals, major concerns, outlook on life and death ultimately providing a framework that will help decision making for events one cannot anticipate. 17 This allows for a more structured way of thinking for the patient/surrogate dyad and the ability to conduct these conversations over a period of time. In contrast, surgery often restricts the time available to promote patient/surrogate concordance and the understanding of more varied complications of anesthesia and surgery, potential unpredictable outcomes, and anticipated trajectories of recovery.
There are notable limitations of these prior studies. One of the most distinct limitations is the homogeneity of the populations studied. Cultural factors and health literacy are important considerations in advance care planning and surrogate decision making. For example, various studies have found that discrepancies in advanced care planning and surrogate decision, especially among minority and underserved populations, may be attributed to various barriers such as language, quality of care, health literacy, and historical distrust.18–20 Although achieving greater diversity in research populations presents methodological challenges, this should be considered a priority for future studies in this area.
Additionally, assessment of feasibility is essential in future studies as interventions must be integrated into complex and time-constrained clinical workflows. The studies discussed in the results section notably were all in-person based. As explained by Cooper et al., one of the key barriers to enrollment was lack of time in the preoperative testing center workflow, suggesting a need for process changes to enable engagement with patients and surrogates. Future studies may benefit from leveraging the shift in medicine with the use of telemedicine, video conferencing, and other technological tools to overcome enrollment barriers due to transportation and time constraints. This will likely help not only with enrollment but also provide a more diverse cohort of participants. Furthermore, implementation of interventions of this kind may overlap with other initiatives seeking to integrate palliative care specialists into preoperative care but approaches to optimizing surrogate decision making would ideally not require such a skill set or additional visits to perform.
In conclusion, this scoping review highlights that despite the growing focus on goal-concordant surgical care, evidence characterizing the performance and strategies for improvement of patient/surrogate concordance in the context of surgery is limited. Of interest, there were no studies that evaluated concordance between providers and the patient–surrogate dyad. Future research should investigate a variety of interventions that may improve the ability of surrogates to achieve concordance and fulfill their role appropriately. We feel it is important for the reader not only to be aware that there is little information provided as to how to successfully ensure surgical patient/surrogate concordance, but that despite this lack of guidance, concordance in this dyad is an important a factor that needs to be considered in their own situations with surgical patients.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
There is no relevant funding to disclose.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.