
Abstract
Objective:
Interstitial cystitis (IC) is a visceral pain syndrome with a profound impact on quality of life (QOL). The main aims of the current study are as follows: (1) to determine possible factors that may increase the severity of symptoms and decrease QOL in women diagnosed with IC; (2) to study how symptom severity affects QOL adjusting for these factors; and (3) to investigate which symptom is most likely to impair IC patients' physical and mental QOL.
Methods:
Forty-one women (age, 20–71 years) with moderate/severe IC enrolled in a clinical trial of intravesical pentosan polysulfate sodium in California (USA) were included in this cross-sectional analysis. Demographic and clinical characteristics were evaluated at baseline using the O'Leary-Sant Interstitial Cystitis Symptom Index (ICSI), pain assessment, urgency scale, voiding log for 24 h, and the Short Form-36 (SF-36).
Results:
Being currently unmarried was associated with more severe symptoms. Being unemployed, currently unmarried, obese, never pregnant, and ever use of oral contraceptive were associated with a decrement in at least one QOL domain. Symptom severity was an independent predictor of worse QOL on three domains: bodily pain, general health, and mental health. Pain and nocturia were the only symptoms found to be associated with decline in overall physical quality of life. None of the symptoms had significant impact on the mental component summary of QOL.
Conclusions:
Symptom severity and being currently unmarried were found to be associated with impairment in QOL in IC patients. Managing pain and nocturia may improve the patients' overall physical QOL.
Introduction
Interstitial cystitis (IC) is a devastating urinary bladder condition characterized by pelvic pain, urinary frequency, urgency, and nocturia. 1 Recently, researchers have started to use the term “painful bladder syndrome” (PBS) to describe cases with painful urinary symptoms that may not meet the strictest definition of IC. The term “IC” is used alone when describing cases that meet all of the IC criteria established by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). 2
The actual prevalence rate of IC is unknown, and estimates range widely from 67 per 100,0003 to 575 per 100,0004 based on the diagnostic criteria and methods used in estimating the rate. IC is mainly diagnosed among white females, with a median age at diagnosis of 42–46 years old. 3 Although IC has been known since 1836, 5 its etiology and pathogenesis are still unclear. Therefore, it is not surprising that IC patients suffer 5–7 years on average and often visit as many as eight physicians before the correct diagnosis is made. 6 The debilitating symptoms of IC leave many patients unable to cope with basic daily function. In severe cases, patients often need to void more than 60 times a day and experience severe pelvic pain and dysparunia, 7 which can isolate them from social life and result in severe depression.
Previous epidemiological studies of IC have measured Quality Of Life (QOL) in either IC patients only, 8,9 or IC patients and a control group. 6,10 Comparison across these studies is limited because each used different measurement instruments. In addition, very few studies have assessed the impact of IC symptoms and their severity on QOL. 8,11 None of these studies considered covariates that may confound the association between symptom severity and QOL. Moreover, none of these studies used a validated instrument to measure the severity of IC symptoms.
To the best of our knowledge, this is the first evaluation of the association between severity of IC symptoms and QOL taking into consideration a wide variety of possible covariates that may modify the direct association. The main objectives of the current study were as follows: (1) to determine to what extent socio-demographic, lifestyle, reproductive, and clinical factors are associated with symptom severity and impairment in different domains of QOL among women diagnosed with IC; (2) to assess if the severity of IC symptoms is associated with impairment in all QOL domains after adjusting for the important covariates; and (3) to investigate which symptom is most likely to impair IC patients QOL summary components (physical and mental).
Methods
Subjects and study design
This is a cross-sectional analysis of 41 subjects enrolled in an 18-week randomized double-blind placebo controlled clinical trial to assess the efficacy and safety of a combination of intravesical and oral Pentosan Polysulfate Sodium (PPS) compared to placebo as a new therapeutic option for IC. 12 In brief, females ≥18 years old who recently met the NIDDK criteria for IC and were previously untreated with PPS were recruited from IC patients of Citrus Valley Medical Research, Inc. (Glendora, CA). Women were also required to have negative urine culture, a score of at least 4 on a nine-point pain scale and 5 on the O'Leary-Sant Interstitial Cystitis Symptom Index (ICSI) at baseline. All subjects signed informed consent, and the study design was approved by the Institutional Review Board (IRB) of Foothill Presbyterian Hospital (Glendora, CA) and the IRB of the University of Pittsburgh (Pittsburgh, PA).
Study measures
Socio-demographic, lifestyle (Body Mass Index [BMI] and smoking status), reproductive (ever pregnant, number of pregnancies, using oral contraceptive (OC), and menopausal status) and clinical factors (presence of Hunner's ulcer, severity of glomerulations and co-morbid conditions) were evaluated at baseline. Symptom severity was measured using ICSI, a well-known, validated, self-administered instrument. 13
ICSI includes four items that measure the frequency of IC main symptoms and provide a symptom severity cumulative score (range, 0–20; 0 = no symptoms, and 20 = severe symptoms). The severity of each symptom was also assessed separately for a 24-h period using a voiding log to measure both urinary frequency and nocturia; a pain assessment scale (range, 1–9; 1 = no pain, and 9 = severe pain) to assess pain at the time of each void and an urgency scale (range, 1–5; 1 = no urgency, and 5 = severe urgency) to measure level of urgency at the time of each void. QOL was assessed using Short Form-36 (SF-36), 14 a widely used, validated instrument that assesses eight different domains of QOL: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and mental health. The eight domains of the SF-36 can be grouped into two summary scales: the Physical Component Summary (PCS) and the Mental Component Summary (MCS). The PCS assesses physical health based on physical functioning, role limitations due to physical problems, bodily pain, and general health scales. The MCS assesses mental health based on the mental health, role limitations due to emotional problems, vitality, and social functioning scales. Each of the eight domains, as well as the two summary component scales (range, 0–100), is presented in the norm-based score format. 15
Statistical analysis
The inferences of the parametric technique are based on the large sample properties. With a sample size of 41, the properties may not be applied. Therefore, we used non-parametric approach to assess the study aims. 16 Continuous variables were presented as median, and 25th and 75th percentiles, while categorical variables were presented as percentages. Spearman correlations, Mann-Whitney U-tests, and Kruskal-Wallis tests were used to assess the univariate associations. Multiple median regressions were used to investigate the impact of symptom severity on QOL as well as to determine factors that impair the severity of symptoms and the QOL. All the covariates with a p-value of <0.1 in the univariate analysis were included during model building. Both age and co-morbidity were forced in all models because of their well-known significant impact on study outcomes (symptom severity and QOL). 10,17 All statistical tests were two sided and used a significance level of 5%. All analyses were conducted using STATA version 10.0 (StataCorp LP., College Station, TX).
Results
The study population consisted of 41 IC female patients with a median age of 38 years (range, 20–71 years). The socio-demographic and clinical characteristics of the study population are summarized in Table 1.
Body Mass Index (BMI) was based on self-reported weight and height.
Concomitant conditions, e.g., endometriosis, irritable bowel syndrome, stress, depression, fibromyalgia, hypertension, diabetes.
Severity of interstitial cystitis (IC) symptoms was based on the O'Leary-Sant Interstitial Cystitis Symptom Index score, range of 0–20.
Pain score: 1 = no pain; 9 = severe pain. Urgency score: 1 = no urgency; 5 = severe urgency.
QOL of the study population
Figure 1 shows QOL scores of the eight domains and the two summary components of SF-36 in the current study population compared to those of a normative sample of U.S. females (age range, 18–65+ years). 15 Importantly, all the scores of the different domains and the summary components were substantially below the 50 score value, which indicates that the QOL of IC patients is markedly lower than that for women in the United States in general.
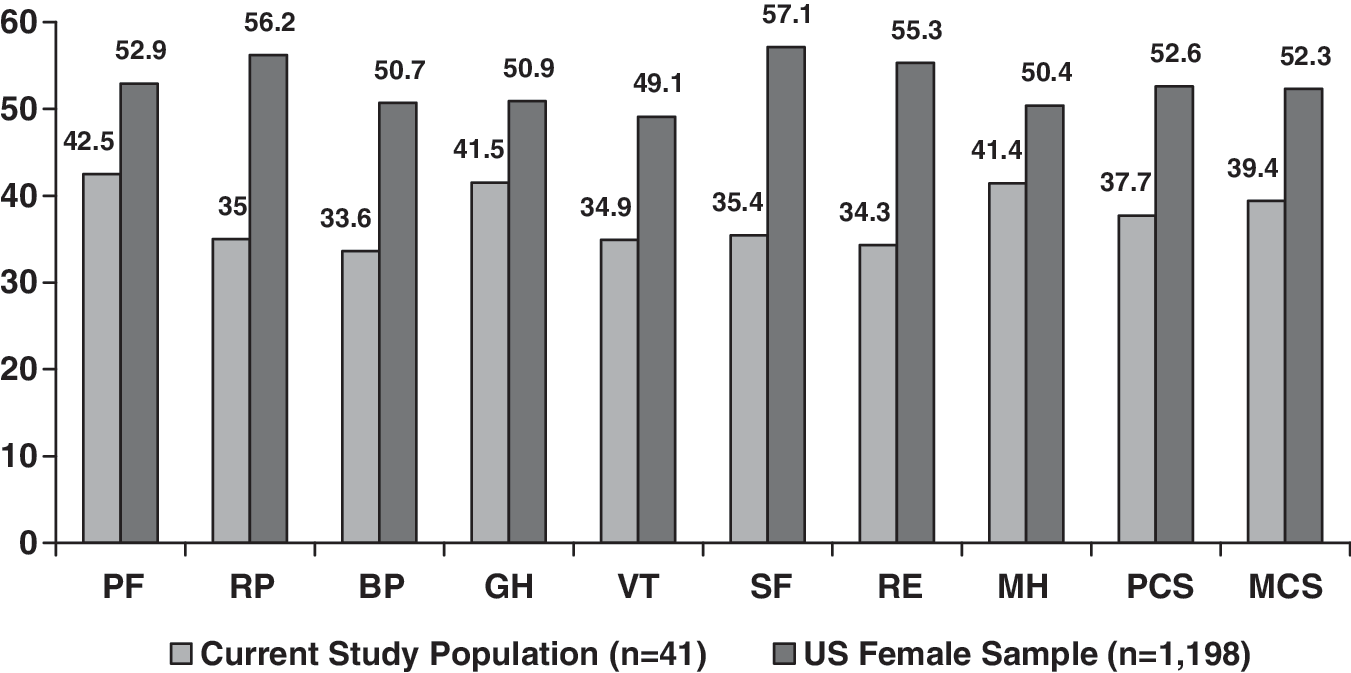
Quality of life scores of the study population and a normative sample of U.S. females (age range, 18–65+ years), General Social Survey, 1998. 15 PF, physical function; RP, role-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social function; RE, role- emotional; MH, mental health; PCS, physical component summary that assesses physical health based on physical functioning, role limitations due to physical problems and bodily pain scales; MCS, mental component summary that assesses mental health based on the mental health, role limitations due to emotional problems and social functioning scales. Each of the eight domains, as well as the two summary component scales (range, 0–100), is presented in the norm-based score format. Therefore, any score above or below 50 is above or below the average of the general U.S. population (General Social Survey, 1998) and each one difference in the score is one-tenth of a standard deviation. 15
Socio-demographic, reproductive, and clinical factors and symptom severity
Univariate analyses were carried out to determine if socio-demographic factors, reproductive, clinical and lifestyle factors were associated with an increase in the severity of IC symptoms. Results showed that only being unmarried (median ICSI score: 16 for unmarried and 11 for married, p = 0.02) and postmenopausal (median ICSI score: 16 for postmenopausal and 11.5 for not postmenopausal, p = 0.02) were each significantly associated with increased severity of IC symptoms (Table 2).
p value: Mann-Whitney U-test or Kruskal-Wallis test. Age, Body Mass Index (BMI), and number of co-morbid conditions were assessed using spearman correlations. None was found to be significantly associated with ICSI (data not shown).
Not Caucasian = Black, Hispanic, Asian, and other.
Currently not married = widowed, divorced, never married, and other.
All study participants had glomerulations. Severity of glomerulations was based on the following clinical definitions:
In multiple median regression and before adjusting for age and co-morbidity in the final model, both marital status and menopausal status had independent, significant associations with the severity of IC symptoms (β = − 4, p = 0.03; β = 4, p =0.04, respectively). After adjusting for age and co-morbidity, only marital status remained significant in the model. The median ICSI score for married subjects was approximately four points less than the median score for currently unmarried subjects, p = 0.03 (data not shown in the tables).
Socio-demographic, reproductive, and clinical factors and QOL domains
In the univariate analyses (data not shown), multiple associations were found between the socio-demographic and reproductive variables and the individual QOL domains. Being unemployed was associated with lower physical functioning. Being unmarried and OC use were associated with lower role-physical. Being unmarried was associated with higher bodily pain. Being unmarried and having larger BMI were associated with worse general health and vitality. Unmarried individuals reported significantly lower social functioning; while women who were never pregnant reported worse mental health. Table 3 shows the results of the multiple median regressions for each of the eight domains adjusting for age and co-morbidities. Interestingly, independent of all other factors, being married was found to be significantly associated with better physical functioning, role-physical, vitality, and social functioning.
Norm-based scores, all scores above or below the 50 are above or below the average, respectively, in the 1998 general US population. 15
Reference category: not employed; currently not married; ever use OC; ever pregnant.
PF, physical function; RP, role-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social function; RE, role-emotional; MH, mental health; BMI, Body Mass Index; OC, oral contraceptive.
Symptom severity and QOL domains and summary components
The univariate analyses showed that symptom severity was significantly related to less physical functioning, role-physical and social functioning and more bodily pain (Table 4). After adjusting for study covariates, severity of symptoms was found to be independently associated with worse bodily pain, general health, and mental health in IC patients (Table 5).
Norm-based scores: all scores above or below the 50 are above or below the average, respectively, in the 1998 general U.S. population. Each one difference in score is one tenth of a standard deviation.
Interstitial Cystitis Symptom Index (ICSI): 0, no symptoms; 20, severe symptoms.
Age, co-morbidity, and marital status for the bodily pain model; age, co-morbidity, marital status, and Body Mass Index (BMI) for the general health and age, co-morbidity, and never pregnant for the mental health model.
Interstitial Cystitis Symptom Index (ICSI): 0, no symptoms; 20, severe symptoms.
SF-36, Short Form-36 Health Survey.
Table 6 shows the multivariate results for specific IC symptoms and PCS. Only pain and nocturia were found to be significantly inversely associated with the PCS after adjusting for age, co-morbidity, and marital status. Because we found significant correlations between IC symptoms (pain and urgency ρ = 0.4, p = 0.01; urinary frequency and nocturia ρ = 0.4, p = 0.004), we were not able to include all four symptoms in one model. Importantly, none of IC symptoms were significantly found to be associated with the mental component of the SF-36 (not shown in tables).
All models were adjusted for age, co-morbidity, and marital status.
Physical Component Summary (PCS): a norm-based score. A score above or below the 50 is above or below the average, respectively, in the 1998 general U.S. population. 15
Pain at the time of voiding (1–9). A score of 1 = no pain; a score of 9 = severe pain.
Urgency scale (1–5). A score of 1 = no urgency; a score of 5 = severe urgency.
Discussion
The results from the current study highlight the profound impact of symptom severity on IC patients' QOL. Our analysis showed that symptom severity significantly impairs two of the physical components and one of the mental components of QOL. Moreover, being unmarried was significantly related to both the severity of symptoms and multiple QOL domains. We also found that pain at the time of voiding and nocturia were the only symptoms that were associated independently with worse overall physical quality of life.
IC remains an idiopathic illness with substantial morbidity in those affected. Previous researchers have studied risk factors for IC, but few have focused on factors that increase symptom severity. 8,18,19 We investigated the effect of socio-demographic, reproductive, lifestyle, and clinical factors on the severity of symptoms among a clinical sample of females with IC. In contrast to other researchers, 8 we found a significant association between marital status and IC symptom severity. A partner or spouse may provide an additional source of social support not available to women without a partner. Social support may be a resource that helps women accommodate to the devastating symptoms of IC. Whether the IC patients who are married experience fewer symptoms or whether increased symptoms are related to not being currently married is a difficult relationship to study in a cross-sectional study, and a prospective study is necessary to confirm this observation.
We observed that postmenopausal women reported higher symptom severity scores. This association, though, was not significant after adjusting for age, co-morbidity, and marital status. Clemens et al. reported that postmenopausal status was associated with worse symptoms and that this association remained significant after adjusting for educational level, depression, frequency, and urgency. 19 After menopause, an alteration in the vaginal flora occurs, with decreased lactobacilli leading to increased colonization by pathogenic fecal flora. 20 This increases the incidence of urinary tract infections (UTI). Furthermore, estrogen deficiency after menopause results in generalized urogenital atrophy. Therefore, postmenopausal women are also at increased risk of dyspareunia, vaginal irritation, pruritus, pain, and symptoms of urgency, frequency, dysuria, and urinary incontinence. 20 While it seems probable that the postmenopausal decline in estrogen levels has a major impact on the lower urinary tract, it is possible that the increase in urinary symptoms at this time is simply due to the aging process, which may explain the attenuation of the significant effect that we found before adjusting for age. Previous studies in women have reported an increased incidence of urinary symptoms starting as early as 10 years before the menopause. 21
Our results are consistent with those from previous research showing that patients with IC reported significantly poorer QOL than controls across all SF-36 domains (p <0.01). 11 Although we did not have a control group, the negative impact on QOL was also demonstrated in our sample of IC patients when compared to a normative sample of U.S. females. 15 Ware et al. suggested that a five-point difference on SF-36 subscales is indicative of a clinically meaningful decrease in QOL. 14 We found subscale differences between 16 and 46.5 points (using the original score). Clearly, the degree of impairment experienced by patients with IC is substantial.
Limited studies have addressed how socio-demographic, reproductive, lifestyle, and clinical history factors affect QOL in IC patients. Although cross-sectional, our study is the first to assess the impact of each of these factors on all domains of SF-36. As expected, we found a significant association between employment status and physical functioning in analyses adjusting for age and co-morbidity. This may be due to the “healthy worker effect” reported in research on other diseases. 17 That is, healthier and better functioning individuals are employed.
As social support is an important predictor of QOL, 22 marital status might be expected to be significantly associated with lower scores of various domains of QOL. This was supported in our analyses. We consistently observed significant associations between being unmarried and worse role-physical, bodily pain, general health, vitality, and social functioning in the univariate analyses. Importantly, even after adjusting for age, co-morbidity, and certain study covariates, marital status was an independent predictor for physical functioning, role-physical, vitality, and social functioning, which suggests a possible substantial impact of marital status on the QOL of IC patients.
Data on the role of symptom severity in IC patients' QOL is limited and inconsistent. For example, Simon et al. showed that patients with severe symptoms report significantly greater limitations in basic daily functions, 8 and Rothrock et al. reported these greater limitations in physical, social functioning, and mental health. 11 More recently, Nickel et al. reported significant effects of IC pain on the physical component but not on the mental component of SF-36 after adjusting for employment status and sexual functioning. 23 Consistent with Nickel et al. findings, our study reported a significant effect of symptom severity on the physical components more than the mental components of QOL.
We investigated which IC symptoms were associated with impairment in PCS and/or MCS, and found that after adjusting for age, co-morbidity, and marital status, pain at the time of voiding and nocturia were significantly associated with impairment in PCS. No specific symptoms were associated with MCS. This was consistent with Nickel et al., who found a significant effect of pain on PCS but not on MCS in a similar study population. 23
The current study had several strengths and limitations. The main strengths were being the first to (1) comprehensively assess the extent to which a wide variety of factors affect both the severity of IC symptoms and the QOL and (2) to examine the association between symptom severity and QOL after adjusting for important covariates and using well-known validated instruments. On the other hand, the major limitations were (1) the cross-sectional design that limits our ability to determine the direction of causality between symptom severity and QOL; (2) the small sample size; (3) the strict application of the NIDDK criteria, which resulted in the exclusion of mild cases and having a sample of moderate to severe cases; and (4) including only female patients who were mainly white. Therefore, the results may not be generalized to mild cases, men with IC, and those of different racial or ethnic groups, although one can argue that mild cases would not necessarily be bad enough to seek care or to show improvement results.
Future studies should confirm what we have reported among mild and moderate cases of other racial and ethnic groups. Researchers should extensively investigate the role of marital status on both symptom severity and quality of life of IC patients. It will be of great interest to confirm the reported protective effect of being married prospectively, and to investigate the possibility that having severe symptoms can also be a reason for not being married or for getting divorced. Future studies should also assess the possible confounding effect of impairment in sexual functioning 23 on the reported associations between marital status, symptom severity, and QOL in IC patients.
Conclusions
The findings from the current analyses may have significant implications for both IC research and well-being of IC patients. Symptom severity and being currently unmarried were important factors found to be associated with impairment in QOL in IC patients. Managing pain and nocturia, in particular, may improve the patients' overall physical quality of life.
Footnotes
Acknowledgments
We thank Josephine Davis and Lisa Regan for their great cooperation and assistance. The clinical trial was supported by Ortho-McNeil Janssen Scientific Affairs, LLC (Raritan, NJ).
Disclosure Statement
No competing financial interests exist.