
Abstract
The previous century was characterized by tremendous advances in reducing maternal mortality and morbidity, as well as dramatic improvements in perinatal outcomes for fetus and newborn. However, there has now developed a plateauing or even a worsening in some of the commonly tracked indicators of reproductive health. In this section, leading policy experts focus on redefining how the health system approaches the task of continuing to improve the reproductive outcomes of women and their offspring. They analyze key underlying fundamentals and offer their individual suggestions for new initiatives to reverse these disturbing negative trends.
Introduction
A nonatypical case report
A 23
This case highlights many failures encountered in healthcare in the United States, ranging from the personal to the societal. The focus of this article and the subsequent articles is a reconsideration of the healthcare system's approach to women's reproductive care with a lifetime perspective and were selected from the Department of Obstetrics & Gynecology and Women's Health of the Albert Einstein College of Medicine and Montefiore Medical Center's annual Autumn in New York Symposium, entitled, Preconception and Prenatal Care: A Life Course Perspective on Women's Reproductive Health and the Outcome of Pregnancy.
Historical Perspective on Prenatal Care
The concept of prenatal care has evolved from one in which there was an original narrow focus on preventing eclampsia to the more current expectation that it is one of the most commonly accessed and broadest preventive healthcare programs in the developed world. Prenatal care has been credited with bringing about dramatic improvements in rates of maternal and newborn morbidity and mortality. Nonetheless, the exact mechanism has been challenged, and in recent decades, those improvements observed over the last century have now leveled off or the situation has worsened (Figs. 1 and 2). This observation raises important issues about the current design and goals of prenatal care. It forces us to question how we are to achieve continued improvements in pregnancy outcome for mother, baby, and family, and even more broadly, it raises a fundamental concern about this nation's approach to women's health for society as a whole.
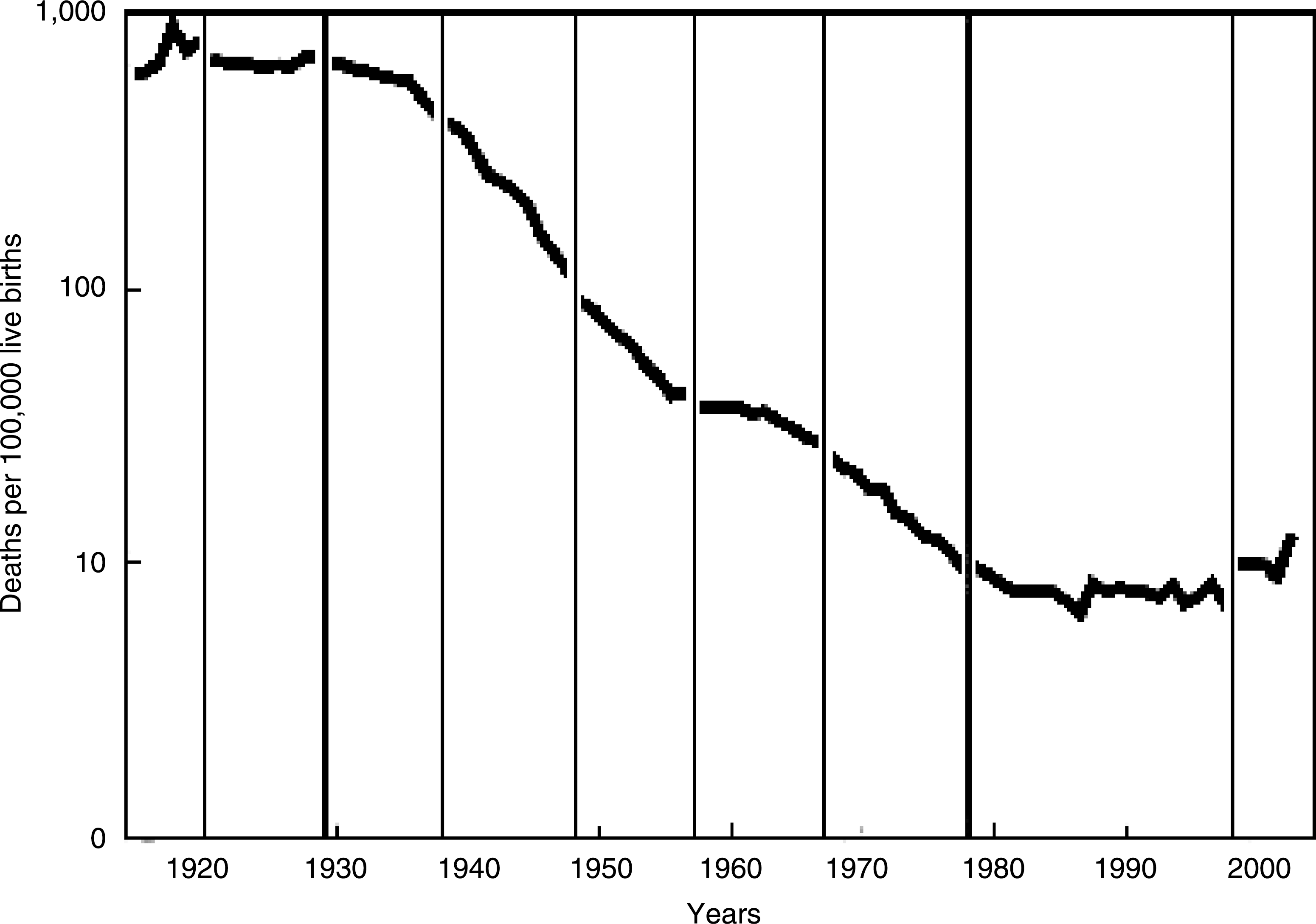
Maternal mortality rates, United States, 1915–2003. (Note: Prior to 1933, data for birth registration states only) Line breaks are shown between successive International Classification of Diseases revisions. Source: Hoyert DL. Maternal mortality and related concepts. National Center for Health Statistics. Vital Health Stat 3(33), 2007.
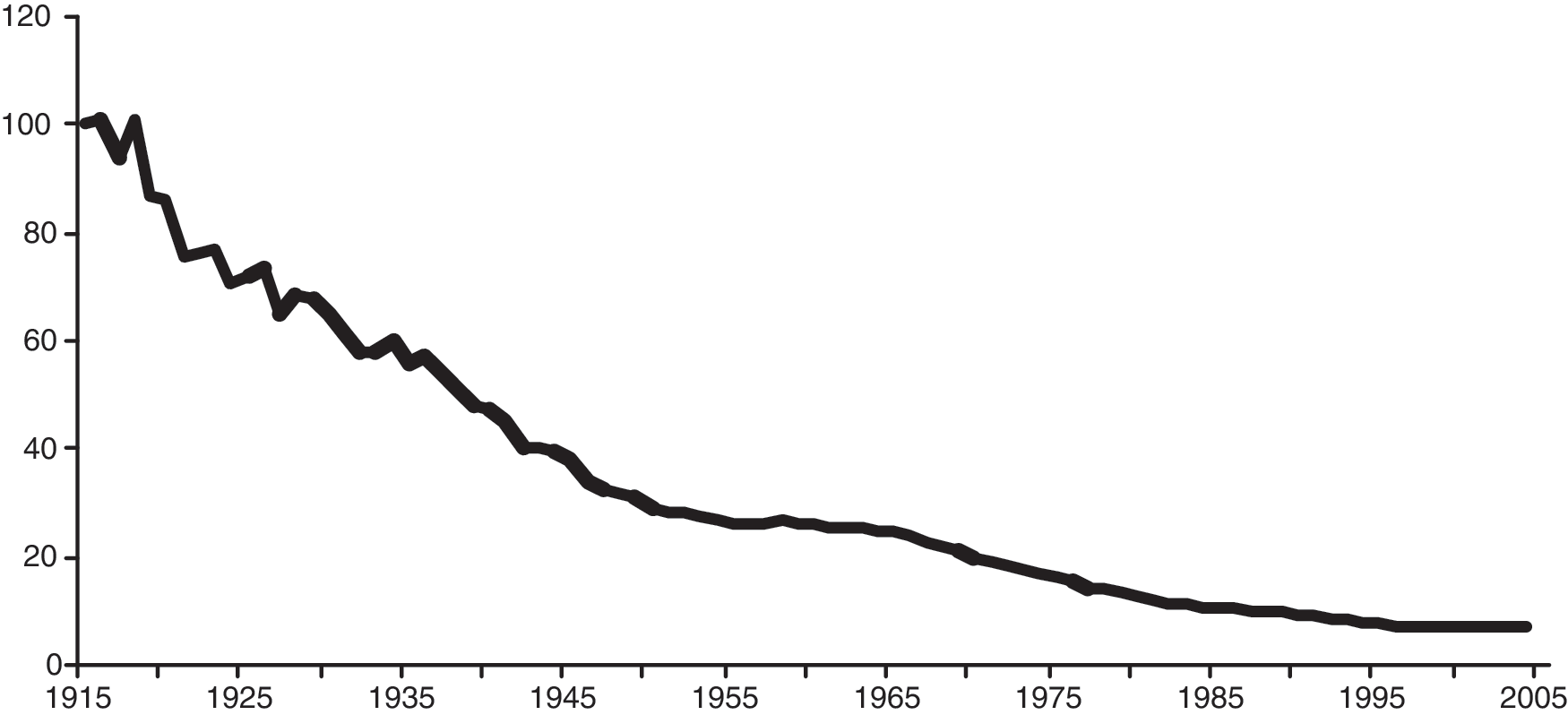
Infant mortality rates, United States, 1915–2004 (rate per 1000 live births). Source: National Center for Health Statistics, final mortality data, 1915–1994, and period linked birth/infant death data, 1995–present. Accessed December 30, 2008, at
The first major event in the development of prenatal care came with the observation by J.C. Lever in 1843 in England that albumin in the urine of pregnant women was associated with the subsequent development of eclampsia. This was followed by a better understanding of the signs and symptoms of preeclampsia and eclampsia. 1 Soon thereafter, in 1858, Sinclair and Johnston founded the world's first prenatal clinic at the Dublin Maternity Hospital as a result of an accident of circumstances. In Dublin, at this time, a pregnant woman had to register and see a physician before receiving permission to give birth at the hospital. Overcrowded conditions necessitated that women apply several months before their expected delivery date. Physicians in the community took the opportunity to take a brief history from each woman, to perform a physical examination, and to check her urine for the presence of protein. Those women with edema, headaches, or proteinuria were empirically treated with bed rest, light nourishment, and purges. It was an unanticipated finding that the incidence of eclampsia was reduced among those women who attended the clinic. 2,3 Thus, prenatal care began with a focus on the detection and prevention of hypertensive disorders of pregnancy.
Organized prenatal care in the United States came later and was largely the result of efforts of nurses and social reformers. In 1901, Mrs. William Lowell Putnam of the Boston Infant Social Service Department began a program of home nurse visits to some of the pregnant women enrolled in the home delivery service of the Boston Lying-In Hospital. The work of this program expanded, and by 1911, an outpatient clinic was established, and women were urged to enroll as early as possible. 1 Mrs. Putnam subsequently convinced Professor J. Whitridge Williams to support systematic prenatal care in Baltimore. In a 1914 study of 705 fetal deaths that occurred among 10,000 consecutive admissions to the Johns Hopkins Hospital, he estimated that prenatal care could have reduced this mortality by 40% through an emphasis on detection and treatment of syphilis. 4
The focus of federal efforts at the time was on addressing the problem of infant mortality. In 1909, President Theodore Roosevelt convened what came to be known as the White House Conference on Children. The Conference recommended the establishment of the United States Children's Bureau, which was eventually created in 1912. In 1924, the bureau published a report entitled Prenatal Care 5 and created a committee whose charge was to establish the standards for prenatal care. The report, published in 1925, set standards of prenatal care and outlined a series of medical and educational components for each visit, which have changed surprisingly little to the present day. 6 Whereas prenatal care was initially developed to respond to complications of preeclampsia and infection, its focus in this report was expanded to foster the well-being of the mother and her fetus in order to ensure healthy outcomes for both.
Codification of the content of prenatal care remained largely unchanged until, in 1989, the U.S. Public Health Service Expert Panel on the Content of Prenatal Care issued its report, Caring for Our Future: The Content of Prenatal Care. 7 In this document, the contemporary goals of prenatal care were outlined (Table 1). In addition to setting goals for the pregnant woman and her infant, the Panel broadened the objective of prenatal care to encompass goals for the entire family as well. In recommending that a woman planning a pregnancy should have a preconception visit and that primary care providers of various backgrounds should be prepared to make appropriate recommendations to optimize the conditions in which pregnancy begins, the Panel also broadened the time frame encompassed by prenatal care. In fact, it was hypothesized that the preconception visit might be the most important prenatal visit of all. While expanding its view to include the period prior to pregnancy, the Panel also extended its vantage point well beyond pregnancy, asserting that services delivered during prenatal care can affect the well-being of a woman beyond the current pregnancy into her future pregnancies and, indeed, even beyond her childbearing years. In an expanded text, these recommendations were taken beyond the medical model and incorporated a full range of psychosocial issues. 8
Adapted from United States Public Health Service Expert Panel on the Content of Prenatal Care. Caring for Our Future: The Content of Prenatal Care. Washington, DC: U.S. Department of Health and Human Services, 1989. 7
Without diluting its central primary focus on the traditional elements of care provided during pregnancy, prenatal care as currently envisioned constitutes a much broader preventive health concept. Unfortunately, although these broader recommendations for the content of prenatal care were visionary, they have yet to be realized in the ensuing 20 years.
Limitations of Prenatal Care
The way prenatal care is traditionally practiced in the United States makes achievement of the goals outlined in the U.S. Public Health Service Report 7 and the subsequent Merkatz and Thompson text 8 difficult to achieve. Prenatal care is still largely structured as a way to screen for infections and detect preeclampsia, with one comprehensive initial visit and then a series of short visits that increase in frequency later in the pregnancy to monitor for the development of hypertension and proteinuria. Added to this more recently has been screening for additional risks to the pregnancy, such as screening for fetal aneuploidies and gestational diabetes. Although these additional risk assessments have been formally added to the content of prenatal care, the reality is that the time available to address them properly has been compressed as the number of activities grows and as obstetrical practices have become so much busier.
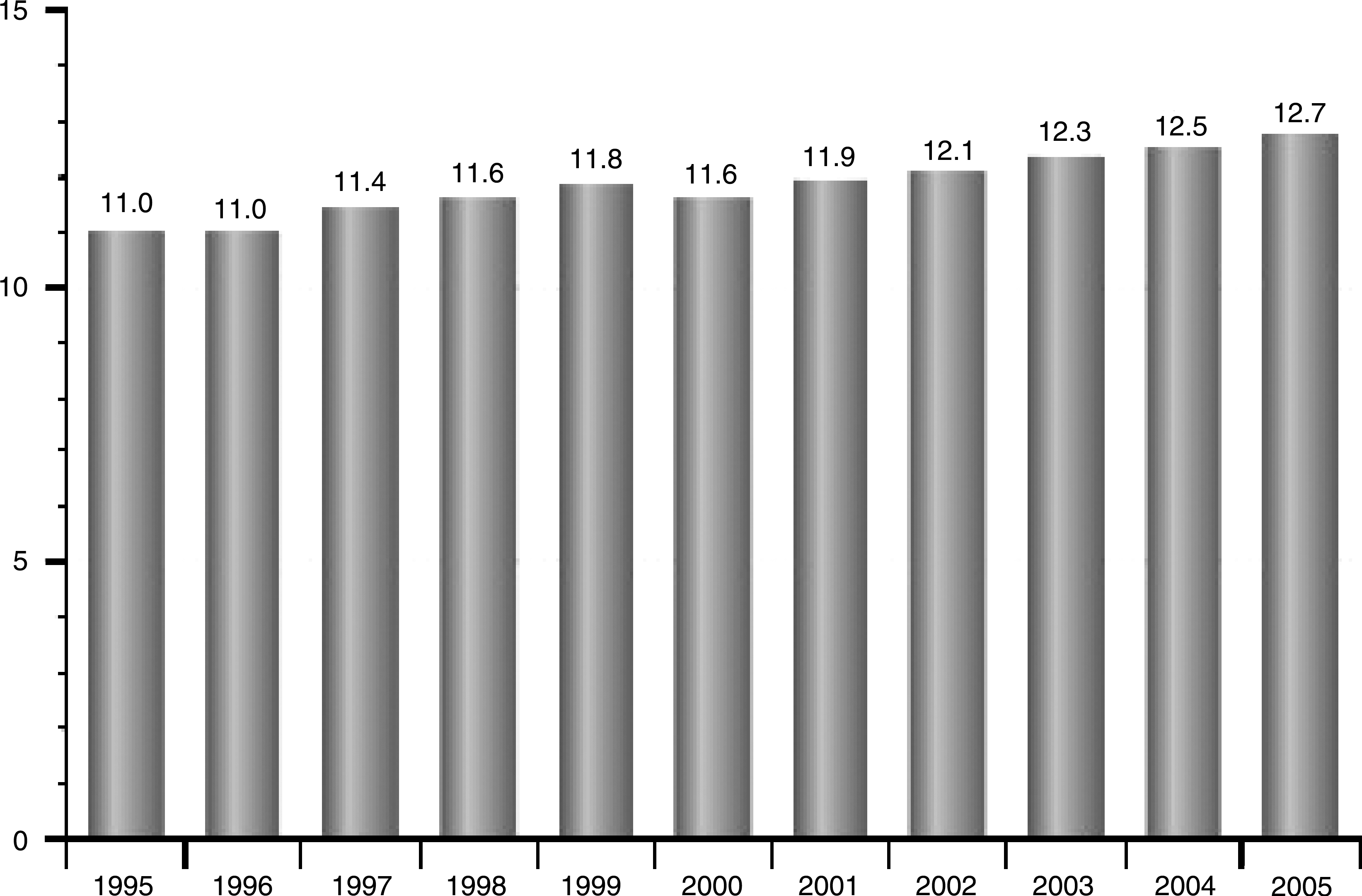
Traditionally, one success of prenatal care has been graded in terms of how it has impacted the rates of preterm birth and the delivery of low birth weight infants, yet as more women are enrolling in earlier prenatal care and more are attending the recommended number of visits, rates of these two indicators have worsened (Figs. 3, 4, and 5). This is not to suggest that there is a direct association between prenatal care and increasing rates of preterm birth and low birth weight babies, only that prenatal care, as currently designed, does not seem to provide an adequate solution for these specific pregnancy outcomes.

Low birth weight, United States, 1995–2005 (percent of live births). Source: National Center for Health Statistics, final natality data. Accessed December 30, 2008, at
Preterm birth, United States, 1995–2005 (percent of live births). Source: National Center for Health Statistics, final natality data. Accessed December 30, 2008, at
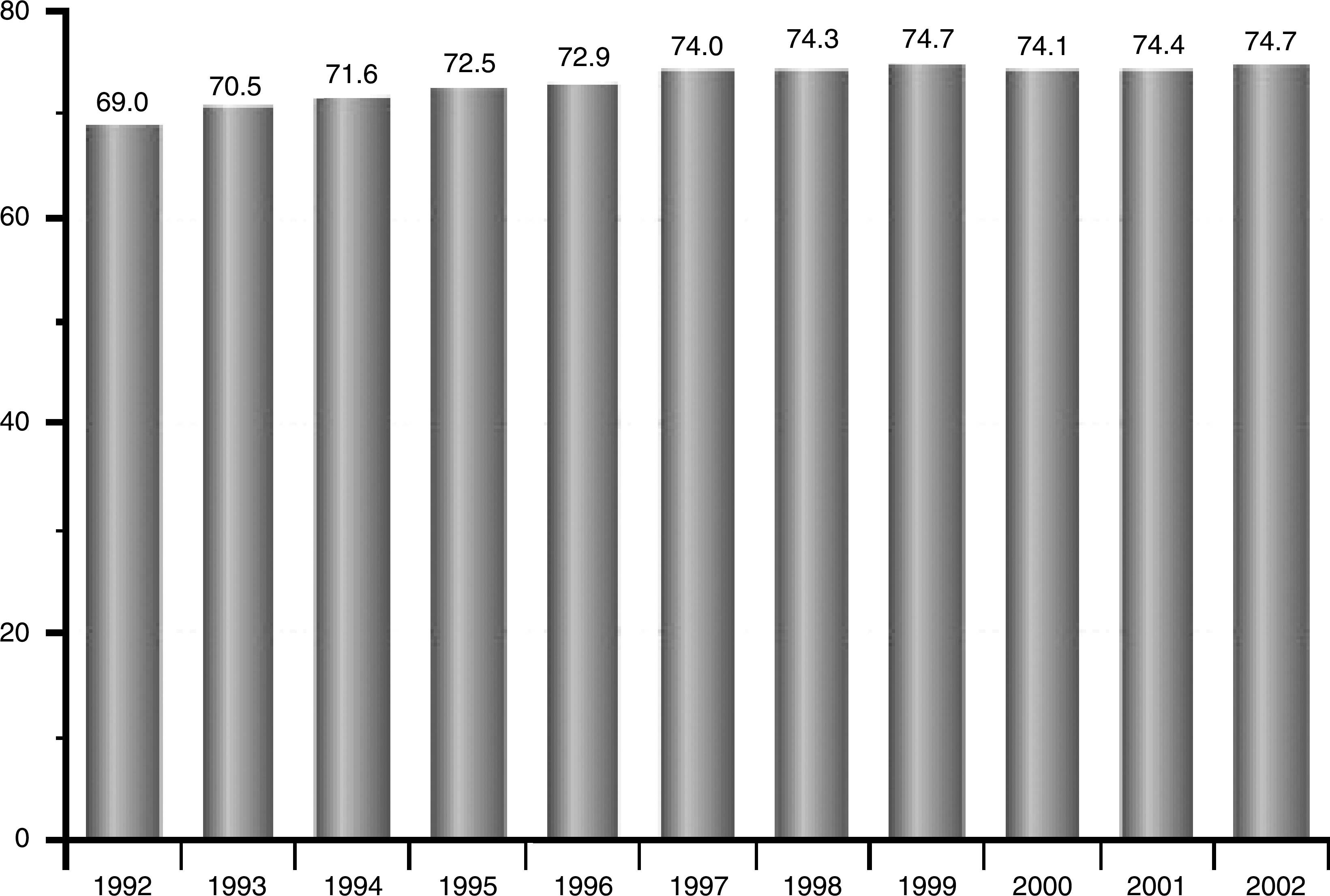
Adequate/better than adequate prenatal care, United States, 1992–2002 (percent of live births). Adequacy is measured using the Adequacy of Prenatal Care Utilization Index, which classifies prenatal care received into 1 of 4 categories (inadequate, intermediate, adequate, and adequate plus) by combining information about the timing of prenatal care, the number of visits, and the infant's gestational age. (From Kotelchuck M. An evaluation of the Kessner Adequacy of Prenatal Care Index and a proposed Adequacy of Prenatal Care Utilization Index. Am J Public Health 1994;84:1414–1420.) Source: National Center for Health Statistics, final natality data. Accessed December 30, 2008, at
Additionally, it is unrealistic to believe that prenatal care can address broader important outcomes, such as reducing rates of birth defects, as organogenesis in the embryo is well underway by the time a woman learns she is pregnant, let alone by the time she arrives for her first prenatal visit. Any effort to reduce exposure to environmental or medically prescribed teratogens or to provide an intervention that reduces rates of birth defects (e.g., folic acid supplementation) needs to occur prior to conception.
Overlaid on this are the startling facts attesting to a growing number of pregnancies occurring among older women and in the setting of a national epidemic of obesity. Additionally, medical advances have resulted in more women conceiving while suffering from a variety of chronic illnesses, such as diabetes, hypertension, cancer, heart disease, and autoimmune diseases. All of this is compounded by the scandalously high rate of unintended pregnancies in the United States, consistently at or near 50%. 9 Clearly, medicine and society need to take a new approach to women's reproductive health if we desire continued improvements in outcomes for women and their offspring. Focusing use of resources only on the brief period when a woman seeks prenatal care and using the current one-on-one model will not address these goals adequately.
A Life Course Approach to Women's Health
More and more evidence is accumulating that although genes may provide foundational building blocks for an individual in determining health and disease, environmental influences starting in utero and extending across the life span may play an equal, if not greater, role. Dr. David Barker of the University of South Hampton, U.K., and Oregon Health and Science University is credited with having pioneered this theory 10 and during his presentation at the meeting, reflected on recent advances in this area. Thus, from the prospective of the fetus, the health of the mother before she conceives impacts the in utero environment she provides for her pregnancy, and that in turn influences the health of her offspring into adulthood, setting the stage for a variety of conditions, such as chronic hypertension and type 2 diabetes mellitus. 11,12
The health of a woman entering a pregnancy impacts her well-being during and after the pregnancy. Thus, for example, if she is obese, she is at greater risk for additional weight gain and for the development of gestational diabetes. Not only does her health during pregnancy affect its outcome, but it may also provide a useful predictor of her long-term health status. 13 If she gains an excessive amount of weight during her pregnancy and does not lose it postpartum or if she has suffered from gestational diabetes during her pregnancy, she is at greater risk for the development of type 2 diabetes later in life. Similarly, women who suffer from preeclampsia during their pregnancies are at increased risk for the subsequent development of cardiovascular disease.
These are but a few examples. There are other more complex ones that have been suggested and are becoming clearer. The article by Lu 14 in this issue of the Journal explores the relationship between maternal exposure to environmental risk factors and emotional stressors that over time lead not only to poor pregnancy outcomes but also to chronic illness, such as cardiovascular disease and cancer.
Seen in this light, the goals for prenatal care set out by the U.S. Public Health Service Task Force in 1989 seem more relevant than ever, but making any headway toward their achievement seems unlikely when limiting ourselves to the 40 weeks of gestation. Efforts to focus on preconceptional health were pioneered by Cefalo and Moos, 15 and in the current issue of the Journal, Moos 16 updates the struggle to incorporate preconception care into everyday practice. More recently, the torch to promote preconception care has been picked up by the Centers for Disease Control and Prevention (CDC) Select Panel on Preconception Care led by Hani Atrash and culminating in the publication of its report in the Morbidity and Mortality Weekly Report. 17 This landmark publication defined the agenda moving forward for making preconception care a major focus of primary care. The first steps toward attaining this goal have already been achieved with the publication in December 2008 of a supplement to the American Journal of Obstetrics & Gynecology devoted to the clinical content of preconception care. 18
A focus on preconception care will not be enough, however, to address the health needs of women throughout their lives. What is needed are new models of care and ways to provide that care over the entire lifetime of the woman, not just during pregnancy. Consideration should be given to drastic innovations, such as the group model of care championed by such organizations as the Centering Healthcare Institute (CHI) and described at the meeting by the founder of that organization, Sharon Schindler Rising. Already, the CenteringPregnancy® group model of prenatal care has demonstrated remarkable improvements in pregnancy outcomes, including reduced rates of preterm birth and improved rates of breastfeeding. 19 This innovative model has been expanded to include CenteringParenting®, which incorporates well women and well child care into a common group visit. CHI is now developing programs to incorporate the Centering principles into care for people with such chronic conditions as diabetes and to support women during menopause. These group programs are also wonderful ways to train students and residents in primary care.
In this section, we explore these issues in greater depth, focusing on medical conditions to demonstrate the principles described, with speakers who presented topics ranging from family planning to the care of women who have received transplants. The conclusion was that it is only through “disruptive innovations” 20 in approaches to care that we will see the leap forward that we crave in women's healthcare.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.