
Abstract
Background:
The Well-Integrated Screening and Evaluation for Women Across the Nation (WISEWOMAN) program in California (Heart of the Family) implements lifestyle interventions to improve health behaviors while reducing cardiovascular disease (CVD) risk factors among low income, uninsured, or underinsured Hispanic women aged 40–64 who participate in the Cancer Detection Programs: Every Woman Counts (CDP: EWC). This study reports the first-year results of the California WISEWOMAN program.
Methods:
Heart of the Family is a within-site randomized controlled study with an enhanced intervention group (EIG) and a usual care group (UCG). The study was conducted between January 2006 and June 2007 at four community health centers in Los Angeles and San Diego counties. Lifestyle counseling focusing on health behaviors was provided by bilingual, bicultural (Spanish and English) community health workers. The study examines two outcome measures: changes in health behaviors; and changes in the CVD risk profile, as measured by the 10-year probability of having a coronary heart disease (CHD) event.
Results:
Women in the EIG group (n = 433), compared to those in the UCG group (n = 436), experienced more improvements in health behaviors, both eating habits and physical activity. The improvement in the 10-year CHD risk was greater for EIG than UCG women. Multiple regression results indicate that this improvement was significantly greater when the women's CHD risk levels were in the upper quartile at baseline.
Conclusions:
Compared with UCG women, women in the EIG were more likely to improve their health behaviors. The CVD risk profile, as measured by the 10-year CHD risk, improved in women with the highest baseline risk.
Introduction
Hispanic Americans, constituting 37% of the California population in 2009, are projected to become the largest racial/ethnic group (40%) by 2016. 1 The rapid growth of Hispanics has been similarly observed in the rest of the United States. Hispanics increased by 28.9% between 2000 and 2007 in the nation, while the growth rates for non-Hispanic whites and African Americans were 1.8% and 8.5%, respectively. 2 Yet, from a health perspective, Hispanic Americans continue to be underserved, and disparities still exist. 3,4,5
Cardiovascular disease (CVD), the leading cause of death in the United States, significantly impacts Hispanic Americans. 6 Studies have shown that Hispanic Americans, particularly Mexican Americans, have a high prevalence of CVD risk factors, in some cases, such as diabetes and obesity, higher than African Americans and non-Hispanic Whites. 3,5,7,8 In addition, compared with non-Hispanic whites, Hispanics are less likely to have health insurance and a usual source of care, resulting in fewer general healthcare and screening office visits. 9,10 Lack of access to healthcare has been shown to be related to untreated conditions and complications, e.g., untreated hypertension, hemorrhagic stroke, and diabetic complications. 11,12,13
As one of the WISEWOMAN (Well-Integrated Screening and Evaluation for Women Across the Nation) programs funded by the Centers for Disease Control and Prevention (CDC), 14,15,16,17 the California WISEWOMAN project provided screening and lifestyle intervention for CVD risk factors. The California project targeted middle-aged, underserved Hispanic women with one or more CVD risk factors. Lifestyle intervention has been shown by various studies to be effective in improving the CVD risk profile, including blood pressure, serum cholesterol levels, smoking status, diabetes, and overweight/obesity. 18,19,20,21 To further enhance effectiveness, the lifestyle intervention in the California WISEWOMAN project was delivered by community health workers (CHWs) who were bilingual and bicultural.
This study, based on the comparison of two groups with and without intervention, evaluated how effective culturally appropriate lifestyle intervention was in improving, over a relatively short-term period (12 ± 2.5 months), health behaviors and the CVD risk profile.
Materials and Methods
Study design, procedures, and baseline statistics
The study design, procedures, and baseline statistics are reported elsewhere. 22 Briefly, the California WISEWOMAN project, named Heart of the Family (Corazón de la Familia), is a within-site randomized clinical trial at four health centers in Los Angeles and San Diego counties. The purpose of the study is to evaluate the short-term impact of lifestyle intervention on CVD risk factors. The lifestyle intervention focused on health behavior counseling and was provided by bilingual, bicultural, female CHWs. Each site was staffed with two CHWs who were supervised by a clinical staff member (RN).
We used the following outcome measures: Change in health behaviors measured by a stage-of-readiness questionnaire; Change in CVD risk factors: total cholesterol, high-density lipoprotein cholesterol (HDL), systolic and diastolic blood pressure, and body-mass index (BMI); Change in the 10-year coronary heart disease (CHD) risk—the likelihood of a CHD event occurring during the next 10 years, where a CHD event is defined as angina pectoris, myocardial infarction, coronary insufficiency, or sudden CHD death. CHD risk was estimated based on an equation developed by Anderson et al.
23
Study participants were recruited from the California National Breast and Cervical Cancer Early Detection Program (NBCCEDP), entitled the Cancer Detection Program: Every Woman Counts (CDP: EWC). To be eligible for CDP: EWC, women are required to be 40 to 64 years of age, having a lower income (less than 200 percent of the federal poverty level [FPL]), and under- or uninsured for their healthcare coverage. In addition to these CDP: EWC eligibility criteria and Hispanic ethnicity, women were invited to participate in the study if their blood pressure or total cholesterol levels were considered at-risk for developing CVD, where “at risk” was operationalized as either ≥ 120 mm Hg systolic or ≥ 80 mm Hg diastolic for blood pressure or currently taking medications to lower blood pressure; and either ≥ 200 mg/dL for total cholesterol or taking medications to lower cholesterol. Women were excluded from the study if their blood pressure was greater than 180 mm Hg systolic or 110 mm Hg diastolic or their cholesterol was greater than 400 mg/dL. Women with these “alert values” were referred to a physician for diagnosis and treatment. Also excluded from the study were women who were pregnant or had past or current CVD events/conditions.
The study participants were randomized at each site to two groups: an enhanced intervention group (EIG) who received lifestyle intervention and a usual care group (UCG), a control group who received usual clinic care only, but no lifestyle intervention. Usual care generally consisted of the distribution of educational pamphlets covering issues related to high blood pressure and high cholesterol. At three of the four sites, the UCG women were also referred to educational classes, and at one site they were provided verbal education. Both groups were assessed for CVD risk factors and health-related behaviors at enrollment and at one-year follow-up. Clinical measures of blood pressure, total cholesterol, HDL, weight, and height were obtained by clinical staff, while behavioral assessments were conducted by CHWs.
The study protocol was approved by CDC's Institutional Review Board (IRB) and the California Committee for the Protection of Human Subjects IRB.
Participants
During the 7-month enrollment period from January 1, 2006 to August 1, 2006, 1,332 Hispanic women were screened at the four sites. Of these, 1,093 women met the socioeconomic eligibility criteria and had at least one CVD risk factor, while 239 women did not meet the criteria. The enrollment process ended on August 1, 2006 to ensure that all the enrollees would have sufficient time to obtain an annual follow-up before the study ending date, June 30, 2007. On enrollment, women were randomized to the intervention group (EIG, n = 552) or the control group (UCG, n = 541). Of the 1,093 women enrolled in the study, 869 women (433 in EIG and 436 in UCG) completed both the baseline screening and annual follow-up. In this paper, we present the analyses of change between the baseline and annual follow-up assessments based on these 869 women.
Lifestyle intervention
The lifestyle intervention for the EIG participants consisted of three face-to-face sessions of assessment and counseling for nutritional and physical activity. Intervention sessions were provided by CHWs, approximately at one, two, and six months after enrollment. CHWs used the 2001 version of the New Leaf curriculum (formally entitled A New Leaf … Choices for Healthy Living) and its Spanish version entitled Vida Saludable, Corazón Contento!
Prior to the study onset, CHWs received a comprehensive, 2.5-day hands-on training on conducting the study. The trainers included professionals who specialized in lifestyle counseling, evaluation, and cardiovascular health. The training consisted of an overview and orientation to research activities, including human subject protection, the research protocol, and data collection; cardiovascular health and the burden of CVD in California; and an introduction to the National and State WISEWOMAN programs. Further details on training for CHWs and RNs and on quality assurance are provided in our earlier paper on the study design. 22
The New Leaf curriculum, a structured intervention program to facilitate CVD risk reduction, was developed by the University of North Carolina at Chapel Hill and used by the North Carolina state WISEWOMAN program. 24 With its 13-page assessment tool, along with a 60-page counseling manual for nutrition, physical activity, and smoking, New Leaf facilitates a lay health counselor to quickly identify and address major problem areas as well as strengths. In the California WISEWOMAN program, culturally competent, bilingual CHWs administered New Leaf interventions in one-on-one sessions. Within two weeks of enrollment, CHWs conducted the initial assessment, spending 40 to 70 minutes with the study participants. The post-intervention assessment was given at the annual visit. Between these assessments, three lifestyle intervention sessions, each lasting from 30 to 45 minutes, were provided to establish goals for behavioral modifications and assess progress.
Outcome measures
The baseline and follow-up visits included the assessment of stage-of-readiness for 12 eating and physical activity behaviors: eating habits (fruits, vegetables, fatty foods, low-fat dairy products, whole grains, sweets, and salt), smoking status, general activity level, engaging in new physical activity, adding intensity to daily activity, and changing daily habits to increase physical activity. Readiness to change was assessed for each behavioral item using a five-point grading scale that closely follows the transtheoretical model of behavioral change. The transtheoretical model suggests that individuals move through different stages from precontemplation to contemplation, preparation, action, and then maintenance. The stage-of-readiness instrument was developed by Dr. Regina Otero-Sabogal (University of California, San Francisco) for the California WISEWOMAN project. Although this instrument has not been validated, the design was based on previous applications of the transtheoretical model. 25,26,27
In analyzing behavioral changes, we focused on a shift from nonaction to action in stage-of-readiness responses. The five-point scale was translated into a binary indicator of “action” when the responses were action or maintenance stages, or “no action” when the responses were stages of precontemplation, contemplation, or preparation. Behavioral change between the baseline and the annual follow-up visits was assessed by counting and comparing the number of items in the action stage.
Clinical measurements of height, weight, total cholesterol, HDL, and blood pressure (systolic and diastolic pressure) were obtained by clinical staff at baseline and at the annual screening visits. The Cholestech LDX® was used for the lipid profile. For practical and economical reasons, serum cholesterol was measured on a nonfasting basis. Two readings of systolic and diastolic pressures were obtained with an interval of at least five minutes between them. Clinical measurement procedures were monitored by the state WISEWOMAN staff during their site visits at least twice a year. Clinical data were validated continuously by the state data management staff by identifying suspected values and inconsistencies using a computer algorithm.
As a composite measure of CVD risk and its change, we used the 10-year CHD risk, defined as the probability of having a CHD event during the next 10 years. The 10-year CHD risk was estimated using the CHD risk equation developed by Anderson et al. 23 The equation was derived from the Framingham Heart Study data; its input parameters are gender, age, smoking status, diabetes, the ratio of total cholesterol to HDL, left ventricular hypertrophy (LVH) as measured by electrocardiography, and blood pressure, either systolic or diastolic. For our estimates, we assumed that the participants did not have LVH. The Anderson equation was used to estimate the 10-year CHD risk change because it is a summary evaluation measure used by the national WISEWOMAN program and its designated evaluator. 28
Statistical analysis
Within-group changes of CVD risk factors between baseline and follow-up were compared using the two-sided paired t-test for continuous variables and the McNemar test for dichotomous variables. For univariate comparisons of changes between the two groups, we used mixed-effects regression models with a random intercept (to account for within-subject correlation) and obtained p-values from the interaction term of intervention (EIG) and time. For binary variables such as prevalence of smokers, mixed-effects logistic regression was used.
In comparing the behavior change between the two groups, we used multinomial logistic regression with a categorical dependent variable of improvement, grouped into “high,” “low,” “no change,” or “worse,” based on the degree of improvement. The “no change” group was used as the reference group in multinomial logistic regression. The degree of improvement was calculated by dividing the number of action stage items added at follow-up by the potential number of items that could be added. The degree of improvement was considered “high” when the actual change was 50% or more of the potential, and “low” when the actual change was greater than zero and less than 50% of the potential. The underlying assumption using the degree of improvement was that the addition of action stage items was influenced by the baseline level of health behavior. Women who were practicing no or very few behavior items at baseline were likely to engage in more action items than those who were already practicing most of the items. Accordingly, we controlled for the baseline levels of health behavior in the regression. Other baseline characteristics, such as age and medication use, were tested as potential confounders, but not included in the final model because of the lack of statistical significance. The measure of improvement that we used, however, had a ceiling effect, such that if a woman was already practicing all the behavioral items in the questionnaire, then there was no room for improvement at follow-up. These women were therefore not included in the analysis of improvement, and their behavior change, which was limited to “no change” or “worse,” was analyzed separately.
Multiple regression was used to assess the changes in the 10-year CHD risk between the baseline and follow-up visits. The models were adjusted for age and CVD risk levels at baseline, and behavioral improvement. As a sensitivity analysis we computed a10-year CHD risk using an equation introduced by Wilson et al. 29 with a set of coefficients presented by D'Agostino et al. 30 In this equation, blood pressure, total cholesterol, and HDL levels are grouped into three to four categories, while in the equation by Anderson et al., risk factor inputs are used as continuous variables.
To see how much of the change in the 10-year risk was attributable to the change in blood pressure level, we computed a simulated risk estimate using the baseline risk profiles, but replacing the systolic blood pressure value with that of the follow-up visit.
In a post-hoc exploratory analysis, we compared the changes in CHD risk among four groups based on their medication use (i.e., blood pressure, cholesterol, and diabetes)—those who were on medication at both assessments, those who were never on medication, and two other groups of women who were on medication at one of the assessments (EIG and UCG combined). The purpose of the analysis was to explore whether better medical treatment, in which medication plays a major part, may have contributed to the study outcomes. Multiple regression was used to test this hypothesis.
To assess the representativeness of our study population, we compared the WISEWOMAN study participants with respondents in the California Health Interview Survey (CHIS). The CHIS analysis was performed using the CHIS Web-based tabulation tool. 31
We used both SAS version 9.2 and STATA version 10 for the statistical analyses, including SAS's GLIMMIX and STATA's mlogit, xtmixed, and xtmelogit.
Results
The EIG and UCG women who underwent both the baseline and annual screenings were evenly matched in their demographic characteristics, medication use, and CVD risk factor levels at baseline (Table 1). There were no statistically significant differences between the two study groups.
Fasting was not required for serum cholesterol measurements. All values except for prevalence and proportions are means.
EIG, enhanced intervention group; UCG, usual care group; CHD, coronary heart disease.
There were 224 women who did not return for the annual follow-up, 119 from the EIG and 105 from the UCG. Although the dropout rate for EIG was slightly higher than for UCG (22% vs. 20%), the difference was not statistically significant. There were no statistically significant differences in demographic characteristics and risk factor levels between those who completed both assessments and those who did not.
Compared to the California population with similar socioeconomic and demographic characteristics (ages 40–64, Hispanic women, uninsured, and less than 200% FPL), as estimated from the 2007 California Health Interview Survey (CHIS), the study population included a slightly greater percentage of women who were overweight (90% vs. 78% in CHIS), but a lower percentage of women who took medicine for high blood pressure (31% vs. 37% in CHIS) and a considerably lower percentage of women who were currently smoking (4% vs. 9% in CHIS). Compared to the Framingham Heart Study (FHS) of white women (N = 2,812) reported by D'Agostino et al., 30 our study population exhibited lower total blood pressure levels (17% vs. 29% in the FHS had systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg) and lower total cholesterol levels (13% vs. 29% in the FHS had total cholesterol ≥ 240 mg/dL).
Changes in health-related behavior
Table 2 shows that a greater percentage of the EIG women made behavior improvements (“high” and “low” improvements combined) in both eating habits and physical activity, as measured by the net number of action stage items added. For eating habits, 71% of the EIG women made improvements at follow-up, compared with less than half of the UCG women (48%). Similarly, the percentages of women who made improvement in physical activity were 68% for EIG and 50% for UCG.
Multinomial logistic regression conveys the same information in the form of relative risk ratios after controlling for the baseline level of action stage items (Table 3). The EIG women were significantly more likely than the UCG women to make improvements. The odds of making a “high” degree of improvement in eating habits relative to “no change” were more than three times greater (relative risk ratio = 3.3, p < 0.001) for the EIG women than for the UCG women. Similarly, achieving a “high” degree of improvement in physical activity was twice as likely (relative risk ratio = 2.1, p < 0.001) for EIG than for UCG. The EIG women were also slightly less likely, though not statistically significantly, to become “worse” in their eating habits or physical activity (relative risk ratios = 0.90 and p = 0.226 for eating habits and 0.83 and p = 0.507 for physical activity).
, statistically significant results at 0.05.
High, actual change was 50% or more of the potential; Low, actual change was less than 50%; Worse, net decrease in action stage items; No change, reference category.
A greater likelihood of adding more action stage items among the EIG women can be observed item by item in Figure 1, in which for each study group and at the two time points, the percentages of women in the action stage are shown by dots (smaller dots for baseline and larger diamonds for follow-up). Behavior items are grouped into eating habits (top seven items) and physical activity (bottom four items).
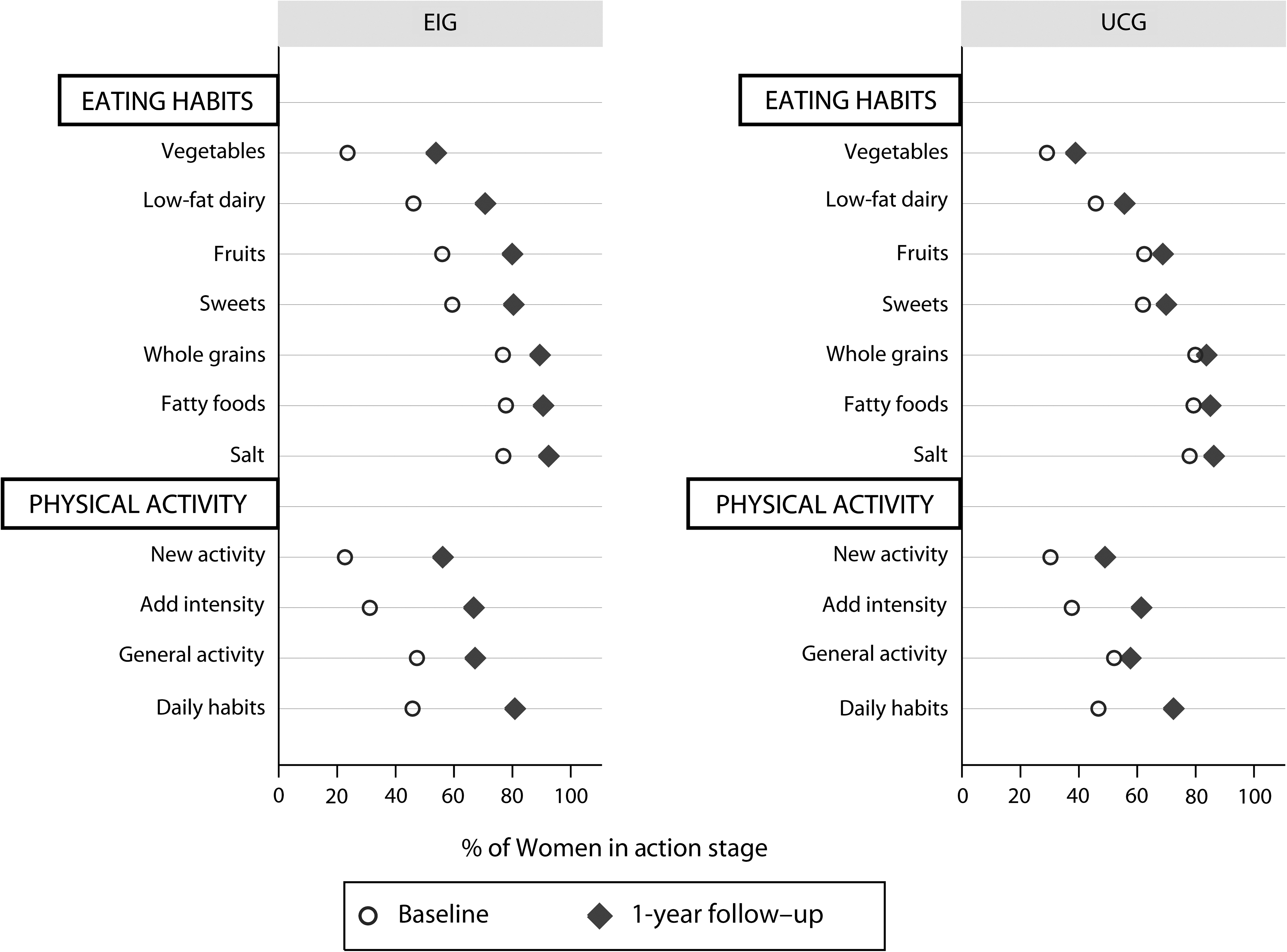
Percent of women in action stage by study group.
Changes in CVD risk factors
Table 4 shows the changes in the levels of CVD risk factors between the baseline and follow-up measurements. Average levels of blood pressure, both systolic and diastolic, at the annual follow-up visit were lower than those at baseline for both groups, resulting in fewer women with blood pressures greater than or equal to 140/90 mm Hg. The reductions were larger among the EIG women than the UCG women, though the only statistically significant difference in reductions was in systolic blood pressure levels (5.9 mm Hg reduction for EIG vs. 3.7 mm Hg reduction for UCG, p = 0.038). The total cholesterol level slightly increased for both groups. Although there were improvements in the HDL level, the ratio of HDL to total cholesterol decreased for both groups. The prevalence of women with high cholesterol (≥240 mg/dL) increased by 2.4 percentage points (12.6% to 15.0%) for EIG and 2.8 percentage points (13.4% to 16.2%) for UCG. BMI levels were virtually unchanged between the two assessments (although there was a small but statistically significant reduction in BMI among the EIG women). The differences in changes between EIG and UCG women, other than systolic blood pressure, were not statistically significant.
The numbers of women varied depending on how many women completed the measurement of a particular risk factor at both assessments. Statistical significance of within-group changes is indicated by an asterisk (*, p-value < 0.05) based on a two-sided, paired t-test. The column on the right shows p-values for the difference of changes between the two groups, which were obtained from the interaction term of EIG and time based on mixed effect model or mixed effect logistic model.
The smoking prevalence among California WISEWOMAN participants was very low at baseline. Nonetheless, the smoking prevalence for both groups decreased, with a statistically significant amount for EIG women. The difference in reductions between the EIG and UCG women, however, was not statistically significant.
Changes in 10-year CHD risk
For both groups, there was an improvement in the estimated 10-year CHD risk between baseline and annual follow-up—reductions of 0.009 for EIG and 0.005 for UCG, both statistically significant (Table 4). The between-group difference in the 10-year CHD risk improvement, though greater for EIG (EIG–UCG, 0.004), was not statistically significant (p = 0.051).
Greater risk reductions/improvements for EIG compared to UCG were evident at higher baseline CHD risk levels, as shown in Figure 2 by the median line inside each box (15 observations that lie outside ± 0.1 of risk changes are not shown). Among women in the lower quartile of the baseline risk, there was almost no change in the 10-year CHD risk. (Note that risk reductions are shown as positive numbers in this figure.) At the same time, the variation of changes (improvement and deterioration as indicated by the vertical size of the boxes) was larger among women at the highest baseline risk compared with those at lower risk. EIG women, except for those at the lowest baseline risk, appeared to have experienced slightly greater improvements than UCG women.
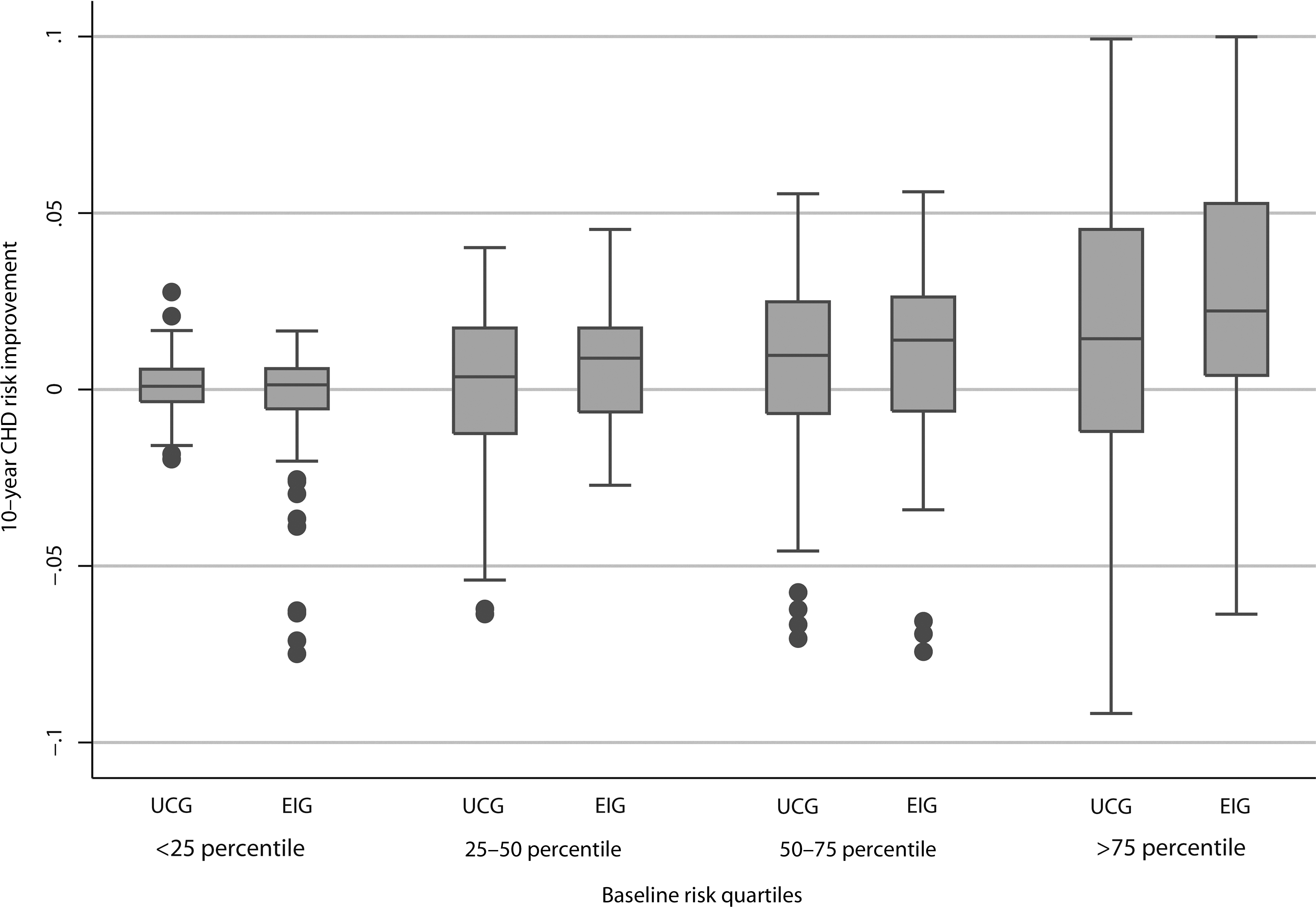
Improvement in 10-year coronary heart disease risk by baseline risk quartiles, by study group.
The regression results in Table 5 (risk reductions are in positive numbers) confirm that, after adjusting for baseline characteristics, the 10-year CHD risk improvement was the greatest among the EIG women who were in the upper quartile of the baseline risk. This is indicated by the statistically significant coefficient of the term “high baseline risk x EIG” (0.016 with p = 0.001).
, statistical significance at 0.05.
“High,” “Medium,” and “Low” baseline risk categories correspond to 75% or higher, 50%–75%, and 25%–50% of the baseline CHD risk levels respectively. The lowest risk category (0–25%) was omitted as the reference category. The risk category variable was coded using Helmert coding, so that the estimated coefficient of each risk level compares the mean value of that level (e.g., “High”) with the mean of all subsequent risk levels (“Medium,” “Low,” “and “Lowest”). F-test for interaction terms was statistically significant with F = 4.7 (df = 3, 851) and p = 0.003.
Baseline characteristics included in the multiple regression analyses showed a statistically significant association with the CHD risk reduction in two different ways: (1) women with high blood pressure or high cholesterol at baseline made greater improvements in CHD risk than women without these risk factors; and (2) for women who were obese or older than age 55 at baseline, the 10-year CHD risk increased during the study period. Another finding is that the CHD risk reduction was greater among women who made improvement in eating habits during the study period. The association between CHD risk reduction and improvement in physical activity was smaller and statistically not significant.
The sensitivity analysis using the equation from Wilson et al. 29 gave similar results to those based on the Anderson et al. 23 equation, but the regression coefficients for EIG interactions were no longer statistically significant. Since the equation from Wilson et al., unlike that by Anderson et al., uses categorical levels for three CVD risk factors (total cholesterol, HDL, and blood pressure), small improvements in these factors may not have been reflected in the CHD risk estimate and may have led to smaller mean differences of CHD risk between EIG and UCG.
According to the simulation analysis, the improvement in the 10-year CHD risk would only have been 55% to 60% of the actual improvement if the change in systolic blood pressure levels alone had taken place and other risk factor levels had remained unchanged. This suggests that other risk factor changes, though small in size, also contributed to the reduction in the overall risk.
Adding medication use variables to the 10-year risk regression (not presented) showed some, but not a consistent effect of medication use. Improvements in the 10-year CHD risk because of medication use were observed only among women who began using cholesterol medication sometime between baseline and follow-up. In these women, the 10-year CHD risk decreased by an additional 0.017. However, women who were started on cholesterol lowering medications during the study represented only a small percentage of the study population (7% of EIG and 5% of UCG).
Discussion
The results of our study suggest that a culturally appropriate lifestyle intervention focused on assessment and counseling was associated with improvements in health-related behaviors, systolic blood pressure levels, and the 10-year CHD risk assessment.
The size of the improvement in the 10-year CHD risk and systolic blood pressure levels is comparable to that observed in other WISEWOMAN sites. 28,32 The 10-year CHD risk reduction pooled from eight WISEWOMAN sites with multicomponent intervention (California, not included) was, on average, 0.005 (improved from 0.065 to 0.060), while the average reduction among EIG women in this study was 0.009 (improved from 0.069 to 0.060). The average reduction in systolic blood pressure levels found in other WISEWOMAN sites was 1.3 mm Hg (from 127.4 mm Hg to 125.8 mm Hg), which was smaller than that of this study (5.9 mm Hg reduction, from 125.1 mm Hg to 119.2 mm Hg).
There was no improvement in the average total cholesterol and BMI levels among our study population (EIG or UCG), although in other WISEWOMAN sites there was a statistically significant reduction of the average total cholesterol, 2.0 mg/dL, from 216.5 mg/dL to 212.1 mg/dL. One possible explanation is that the women in our study were, on average, healthier at baseline than those of other WISEWOMAN sites. The average EIG women's baseline total cholesterol level was 198.4 mg/dL, compared with 216.5 mg/dL at other WISEWOMAN sites, i.e., 9% higher. Nonetheless, when we consider all of the CVD risk factors simultaneously (the 10-year CHD risk), the simulation analysis suggests that a considerable portion (40%–45%) of the risk reduction may be attributable to improvements in risk factors other than systolic blood pressure. Further analyses are necessary to understand how changes in different risk factors are affected in response to lifestyle changes.
Improvement in the 10-year CHD risk was considerably greater among the EIG women whose CVD risk at baseline was higher than the 75-percentile of the study population, while there was little improvement among women in the lowest risk quartile at baseline. Our study suggests that, given these differential effects of lifestyle counseling and the associated cost (according to one study, the 6-month cost per woman was estimated to be $270), 28 it would be reasonable to tier the intervention, based on the baseline levels of CVD risk. The intensity of the intervention is one aspect that can be adjusted depending on the baseline risk level (e.g., for lower-risk clients, provide only the baseline assessment of risk and health-related behaviors and follow-up phone calls or provide a few group counseling sessions). Another aspect that can be adjusted is the focus of intervention (e.g., healthy eating, smoking, physical activity, stress reduction, etc.). Our results have shown a potentially larger impact of improvement in eating habits compared to physical activity. The design of counseling may be adjusted to place a higher priority on healthy eating.
Clients' characteristics, personality, and preference are important factors that must be taken into consideration in designing a tiered approach. For example, some individuals prefer group meetings, while others do better in one-on-one sessions. Our study showed that older and more obese women were differentially impacted in this study, with generally lower improvement in CHD risk. Clients with these characteristics may require a higher level of attention or different approaches from the counselor.
That the UCG women also experienced positive changes was not totally unexpected. 33,34 On enrollment, the UCG women, like the EIG women, were informed in Spanish or English, whichever was preferred, about the study as showing “how lifestyle, food choices, and exercise can reduce risk factors for heart disease,” and that blood pressure, cholesterol, height, and weight would be measured at enrollment and one year later. All women were notified of their clinical values. The UCG women received usual clinic care for elevated blood pressure and cholesterol, the content of which varied by site. These design elements may have considerably weakened our ability to detect a difference between the two study groups.
Although women in this study had one or more CVD risk factors, for most their risk factor levels were generally not at the level where it is advisable to take medication for lowering blood pressure or cholesterol. For this reason, medication use was not associated with the average reduction in the 10-year CHD risk with statistical significance in our multivariate analysis of the entire study population. Most of the risk reduction was attributable to factors other than medication use, most likely lifestyle counseling.
The strengths of our study include: a single ethnic group with a considerable sample size (869 women with complete assessments); a lifestyle intervention that uses well-tested materials, delivered by bilingual and bicultural CHWs who were trained on relevant topics and devoted their best efforts to providing assessment, counseling, and data collection; and continuous quality assurance of program implementation and data management. Culturally competent CHWs played a key role in achieving the relatively low dropout rate (overall 20%) through encouragement at face-to-face sessions and follow-up phone calls.
Several limitations of the study should be noted. While the homogeneity of the study population (underserved Hispanic women) and the intervention is a combined strength, the study sacrifices generalizability of the findings. Our data collection instruments for key outcome measures (i.e., stage-of-readiness questions, medication use, smoking status, and history of heart disease, hypertension, and diabetes) relied on self-reports.
Finally, the follow-up period of 12 ± 2.5 months was not long enough to draw inferences about sustainability of behavioral changes and further improvement in CVD risk factors, if the changes are maintained. Neither do we know the timing of behavior changes in relation to changes in risk factors. Thus, we are unable not only to ascertain the possible causal links between these changes, but also to find out if there is further improvement in CVD risk factors after the study period.
Conclusion
In this within-site randomized control study, underserved middle-aged Hispanic women with one or more CVD risk factors improved health-related behaviors in eating habits and physical activity approximately one year after attending three face-to-face lifestyle intervention sessions provided by bilingual, culturally competent CHWs. Women with the highest baseline risk levels also significantly reduced their 10-year CHD risk. Future investigation is needed to ascertain if behavioral improvements can be sustained for a period longer than one year and how such improvements can impact long-term CVD risk factor levels.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions made by many individuals involved in the California WISEWOMAN pilot study: the study participants, pilot site project staff at the four sites, CDS staff, and key partners and project officers from CDC's WISEWOMAN team, Charlene Sanders, M.P.H., R.D., Ryan Loo, Ph.D., and Julie Will, Ph.D., M.P.H.
This work was funded by the CDC under Cooperative Agreement Number U58/CCU922827-04, Component 3. Findings and conclusions in this report are those of the authors and do not necessarily represent the views of the CDC, CDPH, or UCSF. This information is distributed solely for the purpose of predissemination peer review under applicable information quality guidelines. It has not been formally disseminated by the CDC, CDPH, or UCSF. It does not represent and should not be construed to represent any agency determination or policy.
Disclosure Statement
The authors have no conflicts of interest to report.