
Abstract
Women's health is closely linked to a nation's level of development, with the leading causes of death in women in resource-poor nations attributable to preventable causes. Unlike many health problems in rich nations, the cure relies not only on the discovery of new medications or technology but also getting basic services to the people who need them most and addressing underlying injustice. In order to do this, political will and financial resources must be dedicated to developing and evaluating a scaleable approach to strengthen health systems, support community-based programs, and promote widespread campaigns to address gender inequality, including promoting girls' education. The Millennium Development Goals (MDGs) have highlighted the importance of addressing maternal health and promoting gender equality for the overall development strategy of a nation. We must capitalize on the momentum created by this and other international campaigns and continue to advocate for comprehensive strategies to improve global women's health.
Introduction
Women's health in resource-poor settings is tightly linked to poverty, with human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) and maternal conditions constituting the leading causes of death of women aged 15–44. 1 The tragedy is that the causes of death and disability for women in developing countries are preventable and are linked to inadequate access to quality healthcare and the low status of girls and women, highlighting social rather than biological determinants of health.
This article outlines some of the major issues in global women's health, including pregnancy and childbirth, genital fistula, abortion, family planning, HIV and sexually transmitted infections (STIs), cervical cancer, gender-based violence, and female genital mutilation (FGM). By understanding the direct and indirect causes of women's death and disability, we hope to add momentum to the global call to action to improve women's health worldwide.
Pregnancy and Childbirth
According to World Health Organization (WHO) estimates from the year 2000, approximately 530,000 women die each year from pregnancy-related causes, and >10 million suffer long-term disability. 2 A recent publication, however, uses modeling to estimate maternal mortality from 1980 to 2008 and estimates 342,900 deaths in 2008, down from 526,300 in 1980. 3 Although the exact number of maternal deaths is not known, by all accounts the figure is unacceptably high. The leading direct causes of maternal mortality are hemorrhage, sepsis, unsafe abortion, obstructed labor, and hypertensive diseases of pregnancy, and indirect causes include anemia, HIV, and malaria (Fig. 1). 4 The vast majority of these deaths take place in the developing world, where women suffer a high risk of death and disability with each pregnancy and because of high fertility rates, are exposed to many pregnancies in their lifetime. The global disparity in maternal mortality is shocking: 1 of 6 women in the poorest parts of the world will die from a pregnancy-related cause, whereas only 1 in 30,000 women in Northern Europe will suffer this fate. 5 The proportion of deaths in sub-Saharan Africa is estimated to be >50% of all global maternal deaths. 3 The children of women who die are left vulnerable to premature death, adding to the pain and suffering of the families left behind. 4
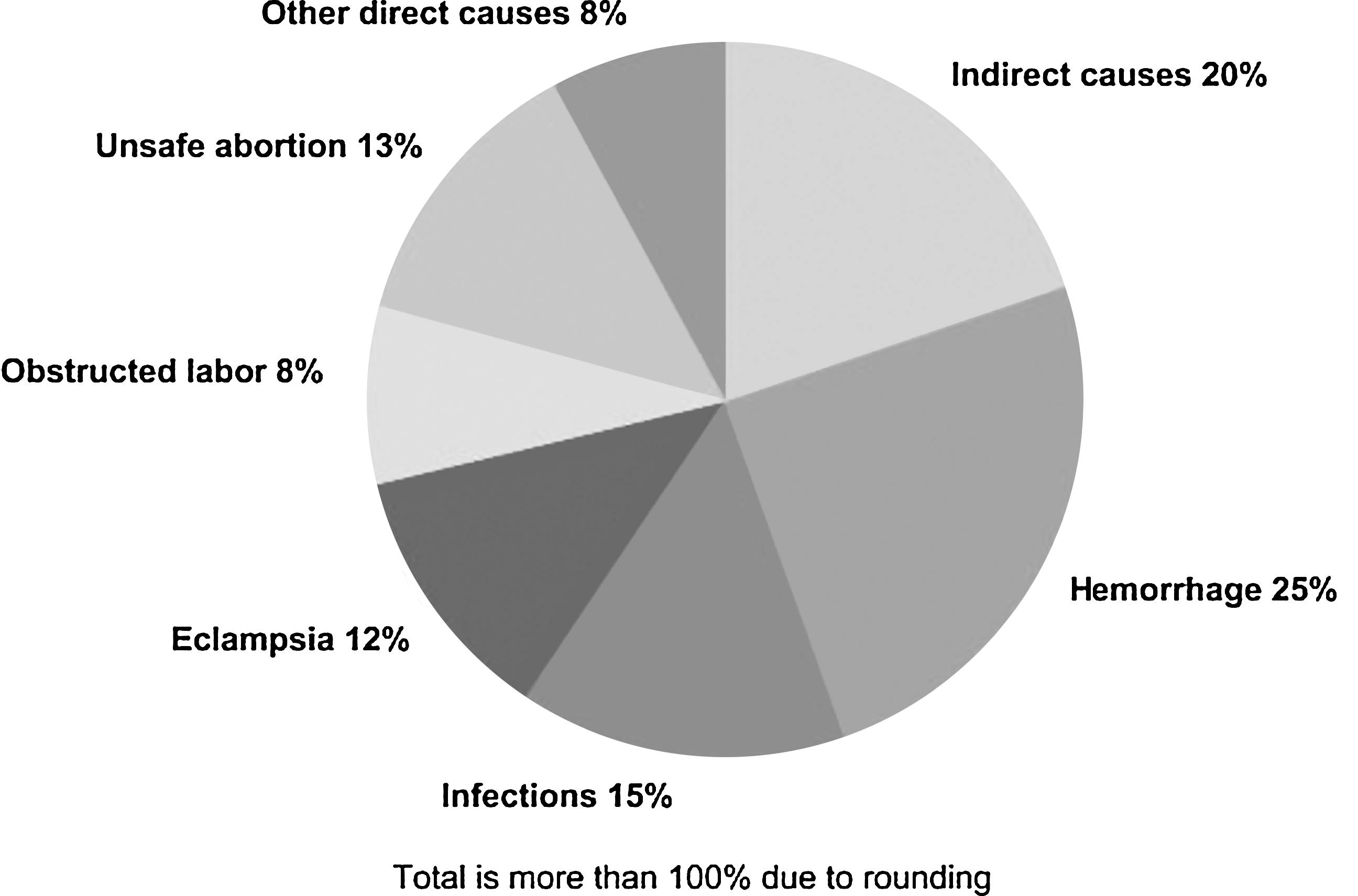
Causes of maternal death. Reprinted with permission, World Health Organization, 2005, page 62. 4
The Millennium Development Goals (MDGs) were adopted in the year 2000 by 189 heads of state as a framework for development. They established eight goals with corresponding targets to reach by the year 2015 and identified key indicators by which progress would be measured. 6 MDG 5, to improve maternal health, highlighted the need for strategies to reduce maternal mortality and reliable statistics by which to measure progress, as reducing maternal mortality by 75% by 2015 was established as the target for this goal. 6 The best way to capture accurate estimates for maternal mortality is widely debated, and the lack of reliable statistics makes it difficult to assess progress toward this goal. By all accounts, however, most nations are nowhere near meeting this target, although there is wide variation between countries in their progress toward this goal. 3,5 Authors of a recent publication that uses modeling to estimate maternal mortality assert that although they found a yearly rate of decline in maternal mortality of 1.8% since 1980, a yearly rate of decline of 5.5% would be necessary to meet MDG 5. 3
Certain risk factors, such as young age, older age, high parity, poverty, HIV, malnutrition, anemia, and hypertension and other chronic diseases, have been identified as risk factors for maternal mortality; however, a feature that makes this problem so hard to address is that complications during childbirth cannot be predicted reliably. 7,8 It is estimated that 15% of all births will require some kind of lifesaving intervention, termed emergency obstetric care (EmOC). 7,8 Basic EmOC refers to the ability to provide antibiotics, oxytocics, and anticonvulsants and the ability to perform manual removal of the placenta, removal of retained products after miscarriage or abortion, and assisted vaginal delivery. 9 Comprehensive EmOC, typically delivered in district hospitals, includes all basic functions noted above plus cesarean section and safe blood transfusion. 9 Because it is difficult to predict who will need these lifesaving interventions, timely access to EmOC for all women in labor must be available if maternal mortality is to be significantly reduced. 7,8
Although prenatal care has not proven to directly impact maternal mortality, it has been shown that in developing nations, prenatal care can help women establish a relationship with the healthcare system that makes it more likely they will give birth in a facility, and it can play an important role in delivering key interventions to address some of the indirect causes of maternal mortality. 7,10 For instance, a particular strain of Plasmodium falciparum (one of the parasites that causes malaria) has a tropism for the placenta, making pregnant women, especially those pregnant for the first time, particularly vulnerable to severe malaria because even women who have grown up in endemic regions have limited immunity to this particular strain. Malaria, therefore, plays a devastating role in exacerbating chronic anemia in pregnancy and contributes to making anemia a major indirect cause of maternal mortality. Prenatal care can be a key intervention point for malaria prophylaxis (both with bed nets and intermittent prophylactic treatment) and for diagnosis and treatment for patients who are infected. Additional key interventions that can be offered during prenatal care include identifying and treating other causes of anemia, such as micronutrient deficiency and intestinal parasites; providing tetanus vaccine; making delivery plans; and identifying HIV-positive women and providing them with antiretroviral medications. 3,7 There is also evidence that key postpartum interventions, especially community-based care, can have a positive impact on the health of the newborn. 11
The notion of the three delays has been used as a framework for understanding and addressing the circumstances that lead to maternal death during delivery in developing countries. 8 The three delays include the delay in recognizing a birth complication, which often occurs at the household or village level and is dependent on who attends births in the community and the status of women; the delay in transporting the patient to a higher level of care, which is affected by the infrastructure of the nation as a whole and the healthcare referral system in particular; and the delay in receiving appropriate care once at the referral level, which is impacted by the functional status of the health facility and the quality and quantity of providers. The lack of adequate health education systems and the inability to curb internal and external brain drain have led to a huge shortfall in healthcare providers in developing countries, especially in rural areas. For instance, although Africa has 11% of the world's population and 24% of the global burden of disease, it is home to only 3% of the health workforce. 12
Because husbands or other family member often control the finances and may not make decisions that prioritize the health of women, the low status of girls and women has been implicated in the first delay. Thus, programs to improve the status of women are key to addressing the first delay. Strengthening of health systems can help address the second and third delay, and community-based programs and skilled attendance at childbirth can help address the first delay. The concept of skilled attendance at childbirth has been promoted not only as a key intervention to potentially prevent and identify complications at the home or community level but also to provide all women with quality care during labor and delivery. Skilled attendance refers to trained providers who are capable of conducting safe, normal deliveries, employing appropriate measures for preventing complications and recognizing complications when they arise. 7 These providers are typically nurses, midwives, or physicians. This strategy should be distinguished from past programs aimed at training traditional birth attendants (TBAs), laypeople who have had no formal training, in safe delivery, which has not been shown to reduce maternal mortality. 7 Although current recommendations are for facility delivery wherever possible, the concept of skilled attendance extends to home deliveries, where these providers can offer prevention and early recognition of complications and prearranged transport for referrals, a continuum of care from home to facility. 7,13
Community-based interventions to prevent postpartum hemorrhage (PPH) include training skilled birth attendants in active management of third-stage labor (AMTSL). 14,15 AMTSL employs the use of uterotonics, but at the community level parenteral uterotonics, such as oxytocin, are not readily available. Misoprostol has been evaluated as an alternative to parenteral oxytocics for AMTSL and for treatment of PPH and has been found to be promising for these indications. Partly because misoprostol can be used for inducing abortion, however, its acceptance as an alternative to parenteral uterotonics has been controversial. 16,17 The nonpneumatic antishock garment (NASG) can also be used at the community level and has been shown to be effective for decreasing blood loss and stabilizing women with severe hemorrhage. 18 –20
Because reducing maternal mortality depends on an integrated, multilevel response, MDG 5 is extremely difficult to reach, especially in poor nations with underfunded healthcare systems. The tragedy is that almost all maternal death can be avoided, and with the appropriate approach, political will, and funding, this can be done relatively rapidly. 5 This has been demonstrated by a decline in maternal mortality in such places as Romania, Malaysia, Sri Lanka, Thailand, Egypt, Mongolia, and Matlab, Bangladesh. 3,5 Parts of Ghana and China have also seen declines. 3 In each case, the factors that led to these declines have varied, with abortion laws thought to play the key role in Romania, whereas in Thailand, Malaysia, and Sri Lanka, the decline is thought to be due to a combination of improved training for midwives, investment in infrastructure, and free maternity care. 5 More than 30 years of experience in Matlab, Bangladesh, indicates that improved family planning and abortion services, fertility decline (linked to a rising age of marriage and improved female education), and investment in the healthcare system as a whole are responsible for the >50% reduction in maternal mortality that occurred there from 1976 to 2005. 5,21
In Egypt, the maternal mortality ratio (MMR) halved between 1992–1993 and 2000, decreasing from 174 to 84/100,000 live births. 22 Improvements in delays in recognizing problems and seeking medical care and in the quality of care provided were achieved through interventions at the community, healthcare facility, and healthcare professional levels. 22 The interventions consisted of intensive provider training, revised curricula, publication of medical protocols and service standards, increased skilled attendance at childbirth, upgrading facilities, and successful community outreach and media campaigns. 22 It was also noted that women's general education improved over the time period studied, which may have contributed to the decline as well. 22 This approach, improving provider quality of care through training, use of protocols, and creation of standards, as well as investing in community outreach and health facility strengthening should be replicable in other nations and likely will be facilitated by concomitant investment in, and promotion of, girls' education.
A report detailing the decline in maternal mortality in a district in northern Ghana posits that the 40% reduction in the MMR from 637 to 363/100,000 between 1995–1996 and 2002–2004 can likely be attributed to community health outreach programs, increased educational level of girls, increased use of contraception, and increased facility-based delivery. 23 Through the community-based outreach programs, health workers provided reproductive health services, family planning, antenatal care, and coordinated obstetric care with the nearest health facility. 23 A study of maternal mortality in Yunnan, China, found that the MMR decreased from 149 to 63.3/100,000 between 1995 and 2005. 24 Although no clear causal relationship can be demonstrated, hospital delivery seemed to be the strongest predictor of the observed decline, with prenatal care and high-quality home-based care also associated with decreased MMR. 24 Moreover, literacy and income were inversely related to MMR. 24 The authors suggest that interventions that target literacy, economic development, and the health system together are most likely to yield these positive results. They note that because of problems with transportation and poverty, community-based care in the form of quality modern home delivery and an effective referral system is critical in remote areas. 24
In Mongolia, the MMR decreased from 169 to 89.6/100,000 from 2001 to 2007. 25 Although demonstrating a causal relationship between policies and a decrease in maternal mortality is difficult, the authors attributed this decline at the provider level to an approach that included a new course in midwifery, making healthcare providers accountable to health authorities, establishing competencies for healthcare units, and supplemental training for providers. 25 At the health system level, they assert that improved intersectoral collaboration, offering reduced-cost or free services and transportation, and formalized referral systems with more maternity waiting homes contributed to the decline. 25 At the community level, the authors propose that television and radio shows that promoted safe motherhood and raised awareness about these issues among men, along with improved training of healthcare workers in reproductive health, supported this decline. 25 They also noted that abortion legislation had been liberalized in 1989, and access to family planning had improved significantly, which likely contributed to the decline. 25 These reports highlight the assertion that a decline in maternal mortality depends on multilevel, multisectoral interventions.
Maternal mortality is so closely linked to the functional level of a nation's healthcare system that it is sometimes used as a proxy for the measure of a nation's overall health status. 26 Health systems strengthening is thought to be essential for decreasing maternal mortality and includes a substantial investment in health professionals, reliable supply chains for materials and medications, and a functional referral system with strong backup by hospital care. 27 It is noteworthy that the very programs that are essential to strengthen maternal healthcare are also necessary to strengthen the healthcare system as a whole, a feature that can be used to advocate for this approach. Community-based prenatal, postpartum, and even safe delivery care is also promoted as an adjunct to health systems strengthening, as many women still deliver at home and live far from health facilities. A recent controversial article models the potential for community-based programs that include access to misoprostol and antibiotics to reduce maternal death from hemorrhage and sepsis and concludes that up to 33% of deaths from these causes can be averted through these interventions. 28 Others, however, question these conclusions and emphasize that we should not promote community-based care as an alternative, but rather as complementary to comprehensive strengthening of health systems. 27
We must continue to advocate for long-term adequate funding for health systems strengthening coupled with community-based programs. There is growing support for the notion that this approach is likely to be more effective than focusing on any single component alone. 29 It seems the time has come to conduct large-scale research to assess the impact on maternal mortality of a scaleable strategy for health systems strengthening, including community-based care. 29 This approach must encompass strengthening the health system at all levels: the referral hospitals, the district hospitals, the health centers, and community-based programs. It would also include strengthening the supply chain, referral system, transportation, communication systems, provider training, and the use of evidence-based protocols. Moreover, educational campaigns and promotion of girls' education and empowerment are likely to support these efforts.
Fistula
Genital fistula is one of the most devastating of maternal morbidities. A fistula is a connection between any combination of the bladder, vagina, cervix, uterus, and rectum. Fistulae result from the destruction of pelvic tissue, which most commonly occurs after obstructed labor but can also be the result of sexual trauma, such as rape, or a consequence of surgical complications. The physical effects of fistula are continuous urinary or fecal incontinence or both, vaginal stenosis, pain, and frequent infections. The social effects of fistula include divorce, isolation, and malnutrition, as well as the emotional effects of depression and posttraumatic stress. The WHO estimates that approximately 2–3 million women worldwide are suffering from this condition, with the vast majority of the burden in poorer countries, particularly in Africa. 30 These injuries can typically be avoided with early and appropriate access to emergency obstetric care, which is lacking in many developing countries. It is estimated that the incidence of obstetric fistula in the African continent is 50,000–100,000/year, with the rate of occurrence 1–10/1000 deliveries. 31 The chance of successful surgical repair of obstetric fistula is estimated to be as high as 97%, with a range from 16.7% to 100%, depending on the size, site, extent of fibrosis, and various other factors. 32 There are a number of local and international/multinational groups that provide surgical fistula repair services and support. 33 Even when surgery is successful, postoperative incontinence can remain an issue, and the social and emotional aspects of genital fistula can be challenging to address. Postsurgical care is critical to success, and most surgeons recommend abstinence for 3–6 months and contraceptive counseling with avoidance of pregnancy for 6 months to 1 year, with recommendation for cesarean delivery if available. 30 These postsurgical instructions may be difficult if not impossible to follow in many cases.
Although the overall antecedent cause of obstetric fistula is the lack of EmOC, demographic studies indicate that victims tend to be young, uneducated, and from isolated and rural regions. Most have suffered from prolonged labor lasting >2 days, and >90% had deliveries that ended in stillbirth. 34 The physical complications of fistula are devastating, but the social impact of fistula cannot be underestimated. In some studies from India and Pakistan, 70%–90% of women with fistula had been divorced or abandoned—forced out of their homes because of the constant smell of urine or feces and into isolation and often malnutrition and despair. 35
Young age of marriage and pregnancy is a risk factor for fistula because the growth of the pelvic bones is not complete. 35 In Ethiopia and Nigeria, for example, >25% of fistula patients had become pregnant before the age of 15, and >50% had become pregnant before age 18. 36 Fistula can also be the result of vaginal trauma, and fistulae caused by sexual violence, such as rape, can be seen most often in conflict or postconflict regions. The size of this group of affected women is most likely underestimated. 37 In some regions, FGM can increase labor difficulties, and vaginal cutting, performed ceremonially or to relieve obstructed labor by traditional healers, can lead to fistula. 30 Finally, iatrogenic fistula is now becoming more of a concern, most commonly in poorer countries as a result of cesarean sections and other gynecological surgeries performed by underexperienced personnel. 38
There are many challenges to overcome before we can eliminate genital fistula because at its root are the fundamental issues of poverty, gender inequality, and lack of access to medical care. The United Nations Population Foundation (UNFPA) is currently spearheading the Campaign to End Fistula. 38 Globally, the efforts to eliminate genital fistula include prevention by improving access to quality family planning and maternal healthcare, treatment by increasing personnel trained to repair fistula, support through appropriate counseling and physical therapy to improve women's surgical outcomes and societal reintegration, as well as the fundamental work of improving the status and advancement of women and girls.
Abortion
Forty-two million women undergo abortion procedures each year, and 20 million of these abortions are unsafe. Unsafe abortion kills >68,000 women each year, representing approximately 13% of maternal mortality. 39 Five million more women suffer disability, such as fistula, bowel injury, and infertility, and 220,000 children are left motherless as a result of these unsafe procedures. 40 As these numbers indicate, when left with no other choice, women will risk everything, even their lives, to control their fertility. The vast majority of these deaths take place in countries where abortion is illegal, as abortion performed by skilled providers in appropriate facilities is an extremely safe procedure, with very low mortality and morbidity. 5
Evidence has shown that restricting access to abortion does not decrease the frequency of this procedure; it simply increases maternal mortality and renders hundreds of thousands of children motherless. In Europe, where abortion is readily available, abortion rates are <10/1000 women and abortion-related death is 1/100,000 live births, whereas in countries with restrictive laws, the abortion rate is 20–39/1000 women, and abortion-related mortality is 34/100,000 live births. 41 This evidence theoretically should make abortion-related mortality easy to address from a policy perspective—simply make abortion legal, available, and safe, and maternal mortality will drop without increasing the abortion rate. Case studies have documented this. South Africa changed its abortion law in 1997 and saw a 91% decrease in abortion-related mortality. 42 A reverse trend was seen in Romania, where abortion-related mortality increased dramatically after restrictive legislation went into effect and then dropped precipitously when the restrictions were reversed. 39 Although these cases clearly demonstrate the relationship between restrictive laws and abortion-related mortality, often ideology trumps evidence, leaving women dead and children motherless.
In order to decrease maternal morbidity and mortality associated with unsafe abortion in countries where abortion is legal, it is important to continue to advocate for access to safe abortion and train providers in evidence-based techniques. In countries with restrictive laws, creating and supporting postabortion care programs are essential to decrease the public health burden of unsafe abortions and save lives. Training providers in the recognition and timely treatment of complications of abortion and sensitizing them to the importance of treating these patients with compassion and respect and offering comprehensive postabortion family planning are of the utmost importance if abortion-related mortality is to decline.
Family Planning
Access to comprehensive family planning in the developing world could prevent 142,000 maternal deaths and save 1.4 million infants. 43 Family planning can decrease the number of times a woman is exposed to the chance of death in pregnancy overall and prevent particularly high-risk pregnancies—those that happen too young, too close together, too old and those that are not desired and, therefore, lead to unsafe abortion or lack of care-seeking behavior in pregnancy. 7,43 For individuals, access to family planning can help achieve the fundamental human right to choose the number and timing of children, overcome traditional gender roles, help girls stay in school longer, improve maternal health, and allow women to join the labor force. 43 For families, having fewer children allows them to invest more in each child, increases access to education for all children, especially girls, and improves the nutritional status of each child. 43 For societies, improving voluntary family planning programs can decrease poverty, slow population growth, and ease environmental pressure. 43
Family planning programs can be integrated into prenatal and postpartum services, fistula care, and HIV programs. HIV transmission can be decreased through comprehensive family planning programs that include condoms, and family planning can decrease vertical transmission by preventing unwanted pregnancies in HIV-positive women. Family planning programs can also decrease infertility by offering dual protection to women who are at risk for pregnancy and STIs.
From the individual perspective, there can be barriers to accessing family planning services. Family planning providers can be reluctant to provide services to young or unmarried women, and misinformation can lead to unwarranted fears and myths about contraceptive methods or side effects. 1,44 There continues to be a large documented unmet need for family planning, however, with 200 million women worldwide wishing to delay or avoid pregnancy but not using a reliable method of contraception. 43 The demand for family planning is expected to increase 40% by 2050, but funding for family planning is staying stable or decreasing. 43,45 Despite the vast benefits to individuals, families, and communities, as well as the potential to save downstream costs, countries are spending only half of what is required to provide the family planning services that are needed. 43 The world population is expected to increase from 6.8 billion to 9.1 billion by 2050 if fertility rates decline as projected if the demand for family planning is met. 46 If the fertility rate stays stable, as will happen if the unmet need for contraception is not addressed, the population will be 11 billion by 2050. 46 Mobilization of political will and resources is critical to tackle this unmet need and protect women, families, and societies from the downstream costs of undesired pregnancy.
Access for all women and men to high-quality services, including comprehensive counseling, ongoing support to manage side effects, and a wide range of contraceptive methods, along with community-based campaigns to address social and cultural barriers to using contraception, will be successful in meeting the unmet need for family planning. In order to support these programs, funding and political will must be increased, men and communities should be involved, mass media and educational campaigns that highlight the linkages among voluntary family planning, health, rights, and economic development should be undertaken, and access to quality facility and community-based services must be provided.
HIV and STIs
HIV, followed by maternal conditions, has emerged as the leading cause of death for women in the reproductive years, globally and in low-income and middle-income countries (Table 1). 1 In 2007, approximately 15.5 million of the 30.8 million adults living with HIV were women. 1 In some countries, a large segment of the adult population is HIV positive; for instance, in eight Southern African countries, the HIV prevalence among women attending antenatal care clinics was >15%. 1
Table reprinted with permission, World Health Organization, 2009, Chapter 4, page 40. 1
Women acquire the infection primarily through heterosexual sex, and young women, sex workers, injection drug users, and partners of infected males are disproportionately affected. 1 Studies have shown that women are more likely than men to acquire HIV through heterosexual sex with an infected partner because of biological factors, and social factors further exacerbate this vulnerability. 47 Women are less likely to be able to negotiate safe sex practices and less likely to know that condoms can protect against HIV, and stigma and sexual and intimate partner violence (IPV) further decrease a woman's ability to negotiate safer sex practices. 1 Contrary to popular belief, being married further compounds the risk to young girls, as married girls are more likely to have initiated sexual activity compared with their unmarried peers and are exposed to more frequent intercourse with, typically, much older men. 48 Economic instability also puts women at high risk for HIV acquisition, which is sometimes linked with migration and participation in sex work. 1
Women are, however, benefiting from access to antiretrovirals (ARVs), slightly more so than men. 1 Women are also targeted by programs to prevent vertical transmission. In 2008, 45% of pregnant women with HIV received ARVs, compared with 10% in 2004. 1 Unfortunately, these programs often reach women only during pregnancy and do not continue to provide care or ARVs to women after delivery.
Women are vulnerable to STI acquisition for the same reasons that put them at risk for HIV. It is estimated that one in four women in Latin America and sub-Saharan Africa has gonorrhea, Chlamydia infection, syphilis, or trichomoniasis. 1 Because these infections are often asymptomatic and women have limited access to screening and treatment services, these infections can lead to pelvic inflammatory disease (PID), ectopic pregnancies, increased vulnerability to HIV infection, and infertility. 1 In order to curb the spread of HIV and decrease the prevalence of STIs among women in developing countries, access to comprehensive reproductive health services for all women, regardless of age or marital status, is absolutely necessary. Working within communities to improve the status of girls and women, promote girls' education, and curb early marriage is also essential. Continuing to strengthen health systems so that they can provide integrated, comprehensive treatment, including ARVs, to HIV-positive men and women will help decrease the spread of STIs and help those who are infected lead productive, fulfilling lives.
Cervical Cancer
Cervical cancer is caused by high-risk human papillomavirus (HPV), which is an STI. When the infection is detected early through screening programs it rarely leads to cancer, and when it does it is usually at an early, treatable stage. However, in low-income countries, adequate screening and treatment programs are rare, and women often have large invasive lesions that are beyond locally available treatment modalities. There are approximately 500,000 new cases of cervical cancer annually, 250,000 of which will cause death. 49 Approximately 80% of these cases occur in developing countries, where access to screening and treatment is lacking. 1
In Europe and North America, the incidence of cervical cancer decreased precipitously with the introduction of screening and treatment programs, the backbone of which was the cytological examination of cervical cells obtained through routine screening of asymptomatic women. Reflex HPV testing has recently been added to the screening algorithm in some places. Because this approach requires a functional healthcare system, with adequate personnel to perform gynecological examinations and provide treatment, a system for specimen transport and efficient communication of results, and trained pathologists who can review the slides and reliably detect abnormal cells, this approach is not feasible in most developing countries at this time. New approaches, including HPV testing alone and see and treat programs that combine visual inspection with acetic acid (VIA) and immediate treatment of suspicious lesions with cryotherapy, may be promising techniques in resource-poor settings. 50 Implementation of HPV vaccination programs that can take place at the community level are also being studied and adopted by some countries, with the hope of preventing cervical cancer. Like other childhood vaccine programs, if this approach of large-scale prevention is successful, it is likely to significantly curb the morbidity and mortality associated with cervical cancer, although routine screening is still recommended for those who receive the vaccine. Regardless of the approach, a functional healthcare system along with community-based education and recruitment will be necessary for successful programming and, ultimately, prevention of cervical cancer-related death.
Gender-Based Violence and Female Genital Mutilation
The low status of girls and women in many places threatens their autonomy, dignity, and security and contributes to the perpetuation of gender-based violence (GBV). The term gender-based violence encompasses a wide range of human rights abuses, such as rape, trafficking, sexual abuse and harassment, domestic violence, sexual abuse of children, and some harmful traditional practices. Girls are often taken out of school earlier than their male siblings in impoverished families, and this lack of access to educational opportunities is linked to the perpetuation of GBV. WHO conducted a multicountry study on violence and found that between 15% and 71% of women reported physical or sexual violence by a husband or partner, and 24%–40% of women reported that their first sexual experience was not consensual. 51 Physical abuse during pregnancy was also reported by 4%–12% of respondents. 51 Violence during pregnancy is associated with double the risk of miscarriage and quadruple the risk of delivering a low birth weight baby. 52
Around the world, there is growing concern about trafficking of women and girls for forced sex and labor, yet international law and response are still inadequate to curb this widespread and devastating phenomenon. Women also bear the brunt of displacement and insecurity during times of conflict, with women representing the majority of displaced people and suffering increased vulnerability during these uupheavals. 1 Rape has been widespread in recent ethnic conflicts, used to humiliate and intimidate civilians and, in some cases, as a form of ethnic cleansing. 52 Harmful traditional practices, such as forced marriages and child marriages, violate women's and girls' human rights, yet they are common practices in some countries in Asia, the Middle East, and sub-Saharan Africa. 1
In addition to the clear violation of human rights and the personal effects on self-esteem, GBV can also have health and economic consequences. Violence against women is associated with the acquisition of STIs, HIV, unintended pregnancies, and induced abortions, as well as adverse pregnancy outcomes. 1 The first-contact medical examination for victims of rape should include a thorough history and full body examination, treatment of injuries, testing and postexposure prophylaxis against STIs including HIV, pregnancy testing and emergency contraception, and collecting of forensic evidence. Given that many women first seek care for sexual violence through police facilities, it is important that police receive appropriate training and counseling in the examination of survivors and their rapid referral for medical care. The downstream effects of GBV include decreased participation of girls and women in educational and income-generating activities and serious health consequences. 52 In addition to the personal and familial havoc caused by GBV, social and economic development is stunted when the rights of girls and women are violated. 52
Child sexual abuse is prevalent and associated with high-risk behavior later in life, such as early sex, unprotected sex, multiple partners, and substance abuse, all of which carry their own health consequences. Moreover, abuse as a child or adult increases the risk of mental health problems, including depression, post-traumatic stress disorder (PTSD), somatization disorders, and eating and sleep disorders. 1 Mental health services are notably lacking in most of the world, sometimes leaving people who suffer from these problems severely disabled.
FGM is another harmful traditional practice that is closely linked to the status of girls and women and has social, cultural, and religious underpinnings. 53 FGM is now internationally recognized as a violation of human rights, although 100–140 million girls and women are estimated to undergo this procedure. 53 The practice is most common in the western, eastern, and northeastern regions of Africa, in some countries in Asia and the Middle East, and among certain immigrant communities in North America and Europe. Procedures are most often performed on girls between infancy and 15 years of age. 53 FGM ranges from clitoridectomy to infibulation, narrowing of the vaginal opening through the creation of a covering seal formed by cutting and repositioning the inner or outer labia, with or without removal of the clitoris. 54 Immediate complications of the procedure include bleeding, infection, poor healing, urinary retention, and injury to nearby genital tissue. Long-term consequences can include recurrent urinary tract infections, increased risk of complications of childbirth, need for repeat surgeries, and infertility. 54
The MDGs highlight the importance of gender equality in achieving social and economic development. MDG 3, to promote gender equality and empower women, provides a strong basis for promoting gender equity and reducing GBV as a development strategy. 55 In order to address GBV, it is important to continue to gather information about where and under what circumstances these conditions prevail. Moreover, female empowerment is of the utmost importance, not only to combat harmful practices but also to proactively promote the rights of women and girls and to move toward women playing a more prominent political role in their families, communities, and on the national and international levels. Widespread advocacy efforts to raise awareness about the benefits of female empowerment and the devastating effects of GBV and to help individuals, communities, and societies implement strategies to combat this trend are also necessary; advocacy must include male community leaders and members. These approaches may include promoting education for all children, particularly girls; sustainable economic development programs for women; substance abuse and mental health treatment programs; conflict resolution strategies; local and international policy to curb human trafficking; and campaigns to end harmful practices, such as child marriage and FGM.
Conclusions
There are many pressing issues in global women's health that require advocacy, financing, sensitization campaigns, community-based programs, and overall investment in health systems strengthening. These problems must be addressed through a multilevel and multisectoral approach to provide quality services, coupled with programs that tackle the root causes of these problems, namely, gender inequality and poverty. Now is the time for large-scale implementation and evaluation of these comprehensive, integrated strategies.
Footnotes
Disclosure Statement
No competing financial interests exist.