
Abstract
Background:
Chronic inflammation and oxidative stress are associated with the development of metabolic syndrome (MetS). Bilirubin is an antioxidant and has a protective effect against cardiovascular disease (CVD). The purpose of this study was to examine the association between total bilirubin levels and the prevalence of MetS in rural Korean women.
Methods:
This cross-sectional study included 5,266 women (>40 years) enrolled in the Korean Genomic Rural Cohort (KGRC). MetS was defined using the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) guidelines. Total bilirubin levels were categorized into quartiles.
Results:
Subjects in the upper quartiles of total bilirubin were younger and had lower waist circumferences, systolic blood pressure, and triglyceride levels and higher high-density lipoprotein cholesterol (HDL-C) concentrations. The overall prevalence of MetS was 39.0%. When the participants were categorized into quartiles by total bilirubin level, the prevalence of MetS according to increasing total bilirubin quartiles was 47.9%, 41.2%, 34.3%, and 32.7%, respectively. By comparison to the lowest quartile of total bilirubin (<0.61 mg/dL), the odds ratio (OR) (95% confidence interval [CI]) for MetS in the highest quartile of total bilirubin (≥0.94 mg/dL) was 0.63 (0.52-0.77) after adjusting for menopausal status, C-reactive protein (CRP) levels, insulin resistance, and other covariates.
Conclusions:
Total bilirubin level appears to be inversely associated with the prevalence of MetS in rural Korean women >40 years of age in the KGRC, even after adjusting for risk factors of MetS, including body mass index (BMI), menopausal status, CRP levels, and homeostasis model assessment of insulin resistance (HOMA-IR).
Introduction
The prevalence of metabolic syndrome (MetS) is increasing worldwide. This global epidemic disorder is a combination of abdominal obesity, dyslipidemia, elevated blood pressure, and glucose intolerance. MetS is strongly associated with the development of type 2 diabetes mellitus and cardiovascular disease (CVD). 1,2 The prevalence of MetS in adult populations is 20%–30%, depending on age, ethnicity, and diagnostic criteria. 2 The prevalence of MetS in Koreans, as defined by the revised National Cholesterol Education Program (NCEP)–Adult Treatment Panel (ATP) III, is 25.7% in men and 31.9% in women. 3 Chronic inflammation, oxidative stress, and insulin resistance are important factors in MetS initiation and progression. 4 –7
Bilirubin is the end product of heme catabolism in mammals and acts as an antioxidant by efficiently scavenging peroxyl radicals and suppressing oxidation. 8 Low serum bilirubin levels are associated with an increased carotid intima-media thickness and impaired vasodilation, 9 and high serum bilirubin levels are associated with a lower prevalence of vascular occlusive diseases, such as peripheral arterial disease and stroke. 10,11 We hypothesized that bilirubin may also function as a protective predictor of MetS development through its antioxidative and radical-scavenging capacity. In the present study, we investigated the association between total bilirubin levels and the prevalence of MetS in rural Korean women.
Materials and Methods
Study populations and data collection
A comprehensive demographic and health survey was completed by 10,114 healthy adults participating in the Korean Genomic Rural Cohort (KGRC), a subcohort of the Korean Genome Epidemiology Study (KOGES), which collected data about relationships among environmental factors, genetic risk factors, and chronic illness in Korean adults from November 2005 to January 2008.
Physical examinations were performed by trained medical staff following standard procedures. Body weight and height were measured to the nearest 0.1 kg and 0.1 cm, respectively, with patients wearing light indoor clothing without shoes. Each participant's waist circumference was measured at the narrowest point between the lower border of the ribcage and the iliac crest. Body mass index (BMI) was calculated as weight/height 2 (kg/m2). Details on daily alcohol consumption were requested and converted into grams consumed per day. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in the right arm using a standard mercury sphygmomanometer (Baumanometer). Menopausal status was surveyed and recorded by questionnaire. After a 12-hour overnight fast, blood samples were collected from each participant's antecubital vein. Biochemical markers, including levels of fasting plasma glucose (FPG), total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (ADVIA 1650, Bayer), and fasting insulin (Insulin RIA Kit, Biosource), were measured. Daily caloric intake was calculated using Can-Pro 2.0, a nutrient intake assessment software program developed by the Korean Nutrition Society.
Participants with a known diagnosis or past history of myocardial infarction (MI) or cerebrovascular attack were excluded. Participants with serum ALT/AST ≥80 IU/L were excluded to rule out subjects with possible active hepatobiliary disease, and those with serum total bilirubin ≥2.0 mg/dL also were excluded to rule out subjects with potential Gilbert syndrome. Participants with serum albumin <3.5 g/dL were excluded to eliminate the possibility of hepatic malfunction and malnutrition; however, because viral hepatitis markers were not examined and reported in our cohort population, we were unable to identify and exclude participants who were serologically proven and infected by a hepatitis virus. Of the 10,114 potential participants, 5,266 subjects were included and analyzed in this study.
All participants completed an informed consent form before participation. This study was approved by the Institutional Review Board of Wonju Christian Hospital, Yonsei University College of Medicine, Wonju-city, Korea.
Definitions of metabolic syndrome, HOMA-IR, and menopause
The definition of MetS is controversial. We used the modified Asian criteria for MetS from the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI), 12 which defines MetS as the presence of three or more of the following criteria: waist circumference (for women) ≥80 cm; SBP ≥130 mm Hg, DBP ≥85 mm Hg, or on antihypertensive drug treatment in a subject with a history of hypertension; FPG ≥100 mg/dL or on drug treatment for elevated glucose; TG levels ≥150 mg/dL or on drug treatment for elevated TG; HDL-C levels <50 mg/dL or on drug treatment for reduced HDL-C levels. Note that a lower waist circumference cutoff point has been adopted for Asian populations.
Insulin resistance was determined using the homeostasis model assessment of insulin resistance (HOMA-IR). HOMA-IR was calculated using the following equation:
Menopause was defined as the absence of menstruation for 12 or more consecutive months from last menstruation. 13
Statistical analysis
The characteristics of the study population were analyzed using analysis of variance (ANOVA) tests for continuous variables, chi-square tests for categorical variables, and Kruskal-Wallis tests for nonparametric variables. Total bilirubin levels were divided into quartiles: Q1, <0.61 mg/dL; Q2, 0.61–0.75 mg/dL; Q3, 0.76–0.93 mg/dL; Q4, ≥0.94 mg/dL. Odds ratios (ORs) and 95% confidence intervals (95% CIs) for MetS were calculated using logistic regression analysis after adjusting for confounding variables across total bilirubin quartiles.
All analyses were conducted using SPSS for Windows, version 12.0 (SPSS Inc). All statistical tests were two-sided, and statistical significance was set at p<0.05.
Results
Characteristics of the study population (n=5,266 women, mean age 55.6 years, mean total bilirubin 0.80 mg/dL) are shown in Table 1. Subjects in the upper quartiles of total bilirubin were younger and had lower BMI, waist circumference, SBP, TG, insulin, HOMA-IR, and CRP levels and higher HDL-C levels (Table 2). The percentage of current smokers tended to decrease with increasing total bilirubin quartiles.
All data except menopausal status, smoking status, triglyceride, insulin, homeostatic model assessment of insulin resistance (HOMA-IR), and C-reactive protein (CRP) are presented as mean±standard deviation (SD). Triglyceride, insulin, HOMA-IR, and CRP values are presented as median (interquartile range). Smoking status and menopausal status are presented as percentages.
Menopause was defined as the absence of menstruation for 12 or more consecutive months from the last menstruation.
HDL-C, high-density lipoprotein cholesterol.
All data except menopausal status, smoking status, triglyceride, insulin, HOMA-IR, and CRP are presented as mean±SD. Triglyceride, insulin, HOMA-IR, and CRP values are presented as median (interquartile range). Smoking status and menopausal status are presented as percentages.
p value determined by analysis of variance (ANOVA) test.
p value determined by Kruskal-Wallis test.
p value determined by chi-square test.
Menopause was defined as the absence of menstruation for 12 or more consecutive months from the last menstruation.
Q, quartile.
Figure 1 shows the relationship between total bilirubin quartile and prevalence of MetS and its diagnostic components. The overall prevalence of MetS was 39.0% and was negatively associated with higher total bilirubin quartiles. The percentage of subjects with abdominal obesity, high TG levels, and low HDL-C concentrations varied widely and decreased linearly with increases in total bilirubin. The percentage of subjects with higher blood pressure also tended to decrease with an increase in total bilirubin; however, the values were not significantly different among interquartile groups.
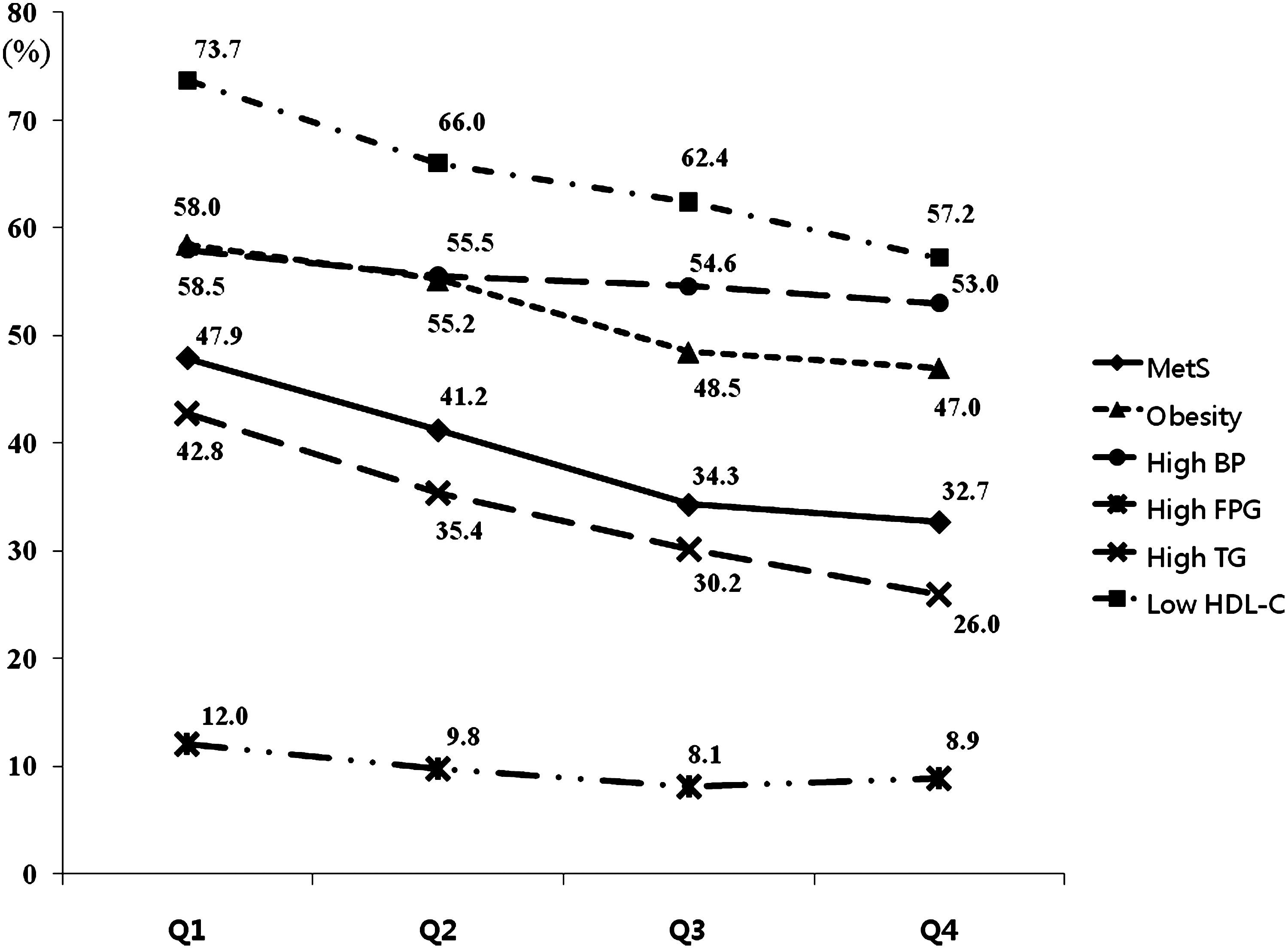
Prevalence of metabolic syndrome (MetS) and its diagnostic components according to total bilirubin quartile. p values for each component according to total bilirubin quartile and trend analysis: MetS, <0.001 and 0.028; abdominal obesity, <0.001 and 0.026; high blood pressure (BP), 0.084 and 0.018; high fasting plasma glucose (FPG), 0.006 and 0.156; high triglycerides (TG), <0.001 and 0.008; low high-density lipoprotein cholesterol (HDL-C), <0.001 and 0.011.
To describe the effects of total bilirubin on each diagnostic component of MetS, we examined our logistic regression analyses according to total bilirubin quartile, after adjusting for multiple confounding factors (Fig. 2). We found that total bilirubin quartile was inversely associated with dyslipidemia, such as high TG or low HDL-C levels (OR [95% CI] for high TG: 0.82 [0.68-0.98], 0.74 [0.61-0.90], and 0.65 [0.53-0.79]; OR [95% CI] for low HDL-C: 0.81 [0.67-0.98], 0.73 [0.60-0.88], and 0.59 [0.49-0.72]). ORs for abdominal obesity in the higher total bilirubin quartiles decreased gradually, but only to a statistically significant degree in the highest total bilirubin quartile (OR [95% CI]: 0.81 (0.65-1.02), 0.80 [0.63-1.01], and 0.74 [0.58-0.93]). High blood pressure and elevated FPG levels were not significantly related to total bilirubin quartile.
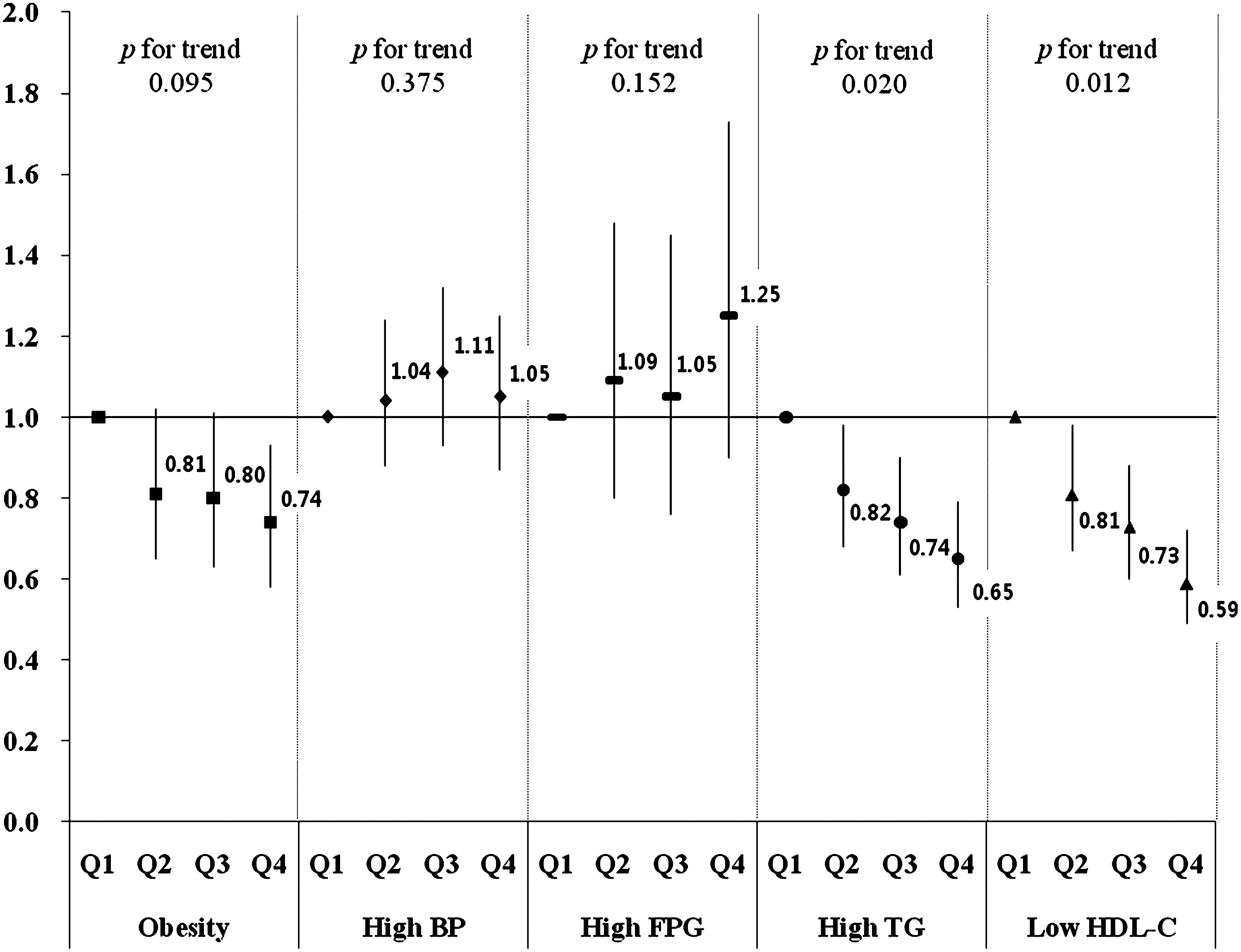
Multivariate logistic regression analysis for diagnostic components of MetS according to total bilirubin quartile Each logistic regression analysis was adjusted for age, energy intake, body mass index (BMI), alcohol consumption, smoking status, menopausal status, C-reactive protein (CRP) level, and homeostatic model assessment of insulin resistance (HOMA-IR), in addition to other diagnostic components of MetS.
Logistic regression analyses were performed to investigate the association between total bilirubin quartile and MetS prevalence (Table 3). Compared to subjects in the lowest total bilirubin quartile (<0.61mg/dL), the ORs (95% CI) for MetS in the highest total bilirubin quartile (≥0.94 mg/dL) were 0.53 (0.45-0.62) and 0.58 (0.49-0.68), when not adjusted and when adjusted for age, respectively. We also conducted multivariate logistic regression analyses after adjusting for age, energy intake, BMI, alcohol consumption, smoking status, menopausal status, CRP level, and HOMA-IR. The OR (95% CI) for MetS in the highest total bilirubin quartile was 0.63 (0.52-0.77) in Model 3. ORs for each analysis model decreased linearly in our trend analysis.
Model 1 was not adjusted.
Model 2 was adjusted for age.
Model 3 was adjusted for age, energy intake, body mass index (BMI), alcohol consumption, smoking status (current, former, never smoker), menopausal status, CRP level, and HOMA-IR.
Discussion
The major finding in this study was that higher total bilirubin levels appear to be negatively associated with MetS prevalence in rural Korean women >40 years of age.
Although the pathogenesis of MetS is not fully understood, several factors, including insulin resistance, chronic inflammation, and oxidative stress, appear to be associated with the development of MetS. 4 –7,14 Abdominal obesity is strongly associated with insulin resistance and expression of inflammatory cytokines. 15,16 Oxidative stress, including the production of reactive oxygen species (ROS) and reactive nitrogen species (RNS), plays a key role in the development of insulin resistance and MetS through chronic activation of stress-sensitive signaling pathways. 17,18 In mice, increased ROS correlates with an augmented expression of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and decreased expression of antioxidant enzymes. 7 In rats, activated NADPH oxidase in adipocyte membranes, when exposed to insulin, has resulted in increased H2O2 compared with control adipocytes. 19 Many stimuli, including hyperglycemia, elevated free fatty acid levels, and inflammatory cytokines, increase ROS/RNS production and oxidative stress. Consequently multiple stress-sensitive serine/threonine kinase signaling cascades, such as Iκβ kinase B (IKKβ), are activated, causing phosphorylation of serine or threonine residue on the insulin receptors and insulin receptor substrate (IRS), instead of tyrosine residue. 14 Abnormal phosphorylation of insulin receptors and IRS is associated with insulin resistance and chronic inflammation and subsequently cause MetS. Furthermore, oxidative stress strengthens and contributes to elevated blood pressure and initiation of CVD. 20
Bilirubin, the end product of heme catabolism, is generated by sequential enzymatic degradation of heme, such as heme oxygenase (HO) and biliverdin reductase. Increased bilirubin levels are associated with a lower prevalence of vascular atherosclerotic diseases, such as peripheral arterial disease and coronary arterial calcification. 10,21 Bilirubin also suppresses the oxidation of lipids and lipoproteins and thus prevents plaque formation and subsequent vascular occlusive diseases, including stroke and ischemic heart disease. 11,22 These protective effects result from the antiatherosclerotic functions of bilirubin that inhibit endothelial cell expression of vascular cell adhesion molecule-1 (VCAM-1), monocyte transmigration, the formation of oxidized LDL-C, vascular proliferation of smooth muscle, and endothelial inflammation. 23 –26 The mechanism that bilirubin is produced by stimulatory signals is through inflammation or oxidative stress that stimulates HO-1, the rate-limiting enzyme in heme catabolism. This process increases heme catabolism in order to minimize potential vascular damage by inflammatory or oxidative insults. 27 Biliverdin, mediated by HO-1, is converted into bilirubin by biliverdin reductase. When bilirubin acts as an antioxidant, it is itself oxidized to biliverdin and then regenerated by biliverdin reductase. 28 Bilirubin plays an important role as a potent antioxidant capable of protecting cells against oxidative stress via the bilirubin-biliverdin interconversion cycle.
Several animal studies have shown the underlying mechanisms of bilirubin in the components of MetS. HO-1 expression and subsequent bilirubin production suppress NADPH oxidase activity and reduce oxidative stress. 29 HO-1 induction improved insulin sensitivity and glucose tolerance and decreased adiposity, although it decreases proinflammatory cytokines in animal study. 30 Hyperbilirubinemic rats attenuated the pressor and pro-oxidant effects of angiotensin II through its antioxidant properties. 31 Furthermore, several animal and experimental studies have demonstrated that bilirubin inhibits tumor cell growth and induces apoptosis by changing cellular signaling or mitochondrial function, in addition to its antioxidative effects. 32 –34 Human data also reveal that high serum bilirubin levels are inversely correlated with colorectal cancer and nongastrointestinal cancers and decrease cancer mortality. 35,36
We performed the same analyses on 3,488 male subjects >40 years in the KGRC. We found no inverse association between total bilirubin and MetS in male subjects. These differing results between the sexes may be caused by differing lifestyles, such as cigarette smoking and alcohol consumption habits. The men in the KGRC consumed much greater amounts of cigarettes and alcohol than the women (percentage of current smoker: 36.6% in men and 1.7% in women; mean daily alcohol intake: 30.5 g/day in men and 2.6 g/day in women). Cigarette smoking is an independent risk factor for high blood pressure, glucose intolerance, and dyslipidemia, 37 –39 and cigarette smoke, which itself acts as an oxidant, induces free radical production, such as ROS, in blood. 40,41 Although dose-response relationships between alcohol consumption and cardiovascular risk factors are inconsistent, alcohol consumption may be involved in the generation of ROS and RNS. 42 We infer that the overwhelming oxidative stresses introduced by cigarette smoking and alcohol consumption may have caused a reduced antioxidative effect of total bilirubin to prevent MetS in the male subjects.
This study involved a large study population composed of healthy, middle-age to advanced-age women in the KGRC and did not include hospital-visiting subjects. Age is negatively related to serum bilirubin levels and plays a role in the confounding factors or covariates for MetS. 43 Because the subjects participating in this study were relatively homogeneous in age (≥40 years), we infer that the confounding effects of age on MetS may have been reduced considerably. As shown in Table 2, the median values of CRP and HOMA-IR differ by total bilirubin quartile, and they require adjustment as confounding variables capable of affecting the prevalence of MetS. Insulin resistance largely contributes to the pathophysiology of MetS through alteration of lipid and glucose metabolism. 44 CRP, an inflammatory indicator and an important risk factor for MetS, was also adjusted for in logistic regression analysis. 4 In addition, menopausal status was adjusted to control the effects of female hormones on MetS in logistic regression analysis, as they are closely associated with MetS and insulin resistance. 45 Although several studies have investigated the association between bilirubin and MetS, few have adjusted for menopausal status, CRP level, and insulin resistance to control for MetS risk factors. 46
There are some limitations to be considered when interpreting the findings of the present work. First, it is difficult to determine a causal relationship between total bilirubin level and the prevalence of MetS. Based on the results of a Chinese study that found that serum bilirubin prospectively predicts and prevents long-term cardiovascular events, 47 we suggest that elevated total bilirubin levels may prevent the development of MetS. Second, most KGRC participants reside in rural areas and are relatively older (≥40 years); therefore, we cannot generalize the findings to a younger, general population. Third, we did not discriminate direct and indirect bilirubin effects from the effects of total bilirubin, and we did not explain the reason that total bilirubin was not significantly associated with high blood pressure and high FPG levels (Fig. 2), although previous experimental data have demonstrated these relationships. 30,31
In conclusion, serum total bilirubin levels were inversely associated with the prevalence of MetS in this cross-sectional study of rural Korean women. This association remained significant even after adjusting for risk factors of MetS, including BMI, menopausal status, CRP level, and HOMA-IR. These data suggest that serum total bilirubin should be monitored in order to assess metabolic and cardiovascular risks and may be elevated using HO-1 inducers to help prevent the development of MetS.
Footnotes
Acknowledgments
We thank all members in the Cohort study in Wonju Christian Hospital for helpful discussion and comments. This study was supported in part by a grant from the Korean Centers for Disease Control and Prevention (Reseach Serial Number: 2005-E71013-00, 2006-E71002-00, and 2007-E71013-00).
Disclosure Statement
The authors have no conflicts of interest to report.