
Abstract
Background:
Cardiovascular (CV) disease is the leading cause of death in women. It is known that acute CV events exhibit temporal patterns of onset, that is, seasonal and weekly. We aimed to verify whether such patterns show differences by gender.
Methods:
We analyzed cumulative data from our previous studies dealing with hospital admissions for CV events, such as acute myocardial infarction (AMI), stroke, transient ischemic attack (TIA), aortic diseases (AD), and pulmonary embolism (PE), in the region Emilia-Romagna (RER) of Italy (ICDM9-CM codes, years 1998–2006). Total population and subgroups by gender (percentage of monthly and daily events) were tested for uniformity with the chi-square test, and a chronobiologic method was applied to monthly percentage of data for seasonal rhythmic analysis.
Results:
Season: We considered 130,693 patients (45.1% women): 64,191 AMI, 43,642 TIA, 4,615 AD, 19,425 PE. The monthly and seasonal distribution showed respective peaks in January and in winter, with no differences by gender. Day-of-week: We considered 168,921 patients (45.6% women): 64,191 AMI, 56,453 stroke, 43,642 TIA, 4,615 AD. The weekly distribution showed a peak on Monday, with no differences by gender. A multivariate regression logistic analysis, including in the model either major CV risk factors (hypertension, dyslipidemia, diabetes mellitus) and subgroups by age, did not find any difference in the temporal distribution of events in women and men.
Conclusions:
The seasonal and day-of-week distribution of occurrence of CV events seems to be independent of gender.
Introduction
Cardiovascular (CV)
In the last two decades, it has been widely reported that the occurrence of acute CV events is not randomly distributed over time but exhibits temporal patterns, that is, circadian or seasonal patterns. In particular, morning hours and winter months are characterized by higher frequency of onset of AMI, 6 –8 stroke, 9,10 aortic rupture or dissection, 11,12 and PE. 13 A day-of-week variation, characterized by a Monday peak of onset, was found for AMI and stroke. 14,15 We aimed to investigate whether the seasonal or weekly pattern of presentation of major CV events may exhibit differences by gender.
Subjects and Methods
Recruitment of cases
We analyzed cumulative data of previous studies from our group dealing with temporal variation of hospital admission for CV events, including AMI, stroke, transient ischemic attack (TIA), aortic diseases (AD), and PE, 16 –21 in the region Emilia Romagna (RER) of Italy, according to the regional database maintained by the Center for Health Statistics.
Setting
The Emilia Romagna is a region of Northeastern Italy, with a total surface area of 22,124 km2 and a total population of about 3,985,000 (approximately 7% of the entire Italian population). Commencing in 1998, the RER database began to collect all the discharge hospital sheets (the so-called Scheda di Dimissione Ospedaliera [SDO]) of patients admitted to all hospitals. The SDO contains information about surname and given name of each subject, gender, date of birth, date and department of hospital admission and discharge, first nine different discharge diagnoses, and most important diagnostic procedures, based on the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM). We used time of admission to hospital as the day of onset of each disease because of the particular organization of public healthcare in Italy, which is completely free of charge for both in-hospital and out-hospital care. An Italian citizen can have access to a medical visit at the general practitioner's ambulatory, at home (by their own general practitioner during diurnal hours and by a community ward doctor during night hours and Saturdays and Sundays), or at the ED (24 hours/day). Thus, especially during weekends, it is more likely that patients go directly to the hospital for acute care. In the case of acute CV events, it is extremely unlikely that day of onset and day of hospitalization do not coincide. The total population was divided into subgroups by gender, presence of major CV risk factors (hypertension, dyslipidemia, and diabetes mellitus), and age (<60, 60–69, 70–79, >80 years).
Data collection and analysis
Monthly/seasonal
Data on monthly and seasonal admissions referred to AMI, TIA, AD, and PE. 16 –19 Hospital admission for each type of acute CV event (percentage of events) was categorized according to 12 1-month intervals and 4 3-month intervals (spring: March 21–June 20; summer: June 21–September 22; autumn: September 23–December 20; winter: December 21–March 20) for circannual and seasonal analysis, respectively.
Day-of-week
Data on day-of-week admission referred to AMI, stroke, TIA, and AD. 16,17,20,21 Hospital admission for each type of acute CV event (percentage of events) was categorized according to the day of the week.
Statistical analysis
The chi-square test and Bonferroni correction for multiple comparisons were used to compare different periods of admission and gender. To investigate the possible existence of a chronobiologic rhythmic variation, monthly percentages of events were analyzed by applying a partial Fourier analysis to the time series data using validated Chronolab software, 22 which can select the harmonic or the combination of harmonics that best explains the variance of the time series data. The percentage of rhythm (PR, i.e., percentage of overall variability of data about the arithmetic mean of the fitted rhythmic function) and the probability value resulting from the F-statistic (hypothesis of zero amplitude) are representative parameters of goodness of fit and statistical significance of each fitted function, respectively. Finally, for evaluation of the risk of time of hospital admission, gender, major CV risk factors, and subgroups of age, a regression logistic analysis and a multivariable logistic regression analysis were used. Significance levels were assumed for p<0.05.
Results
Season
During the considered periods, the RER database contained the records of 130,693 patients (45.1% women) admitted for CV acute events (64,191 AMI, 43,642 TIA, 4,615 AD, 19,425 PE). The monthly distribution (percentage of daily events) showed a peak in January and a trough in July, with no differences between CV single disease and gender (Table 1). The chronobiologic analysis, performed to the monthly percentages of events, yielded a rhythmic seasonal variation (Table 2) characterized by peaks in winter for total cases (January, p=0.044), women (January, p=0.008), and men (January, p=0.102) (Fig. 1). Men, however, also showed a trend toward a biphasic pattern, with peaks in March and October (p=0.072). The seasonal distribution (percentage of monthly events) showed a winter–autumn peak and a summer trough (Fig. 2), with no differences between CV single disease and gender (Table 3).
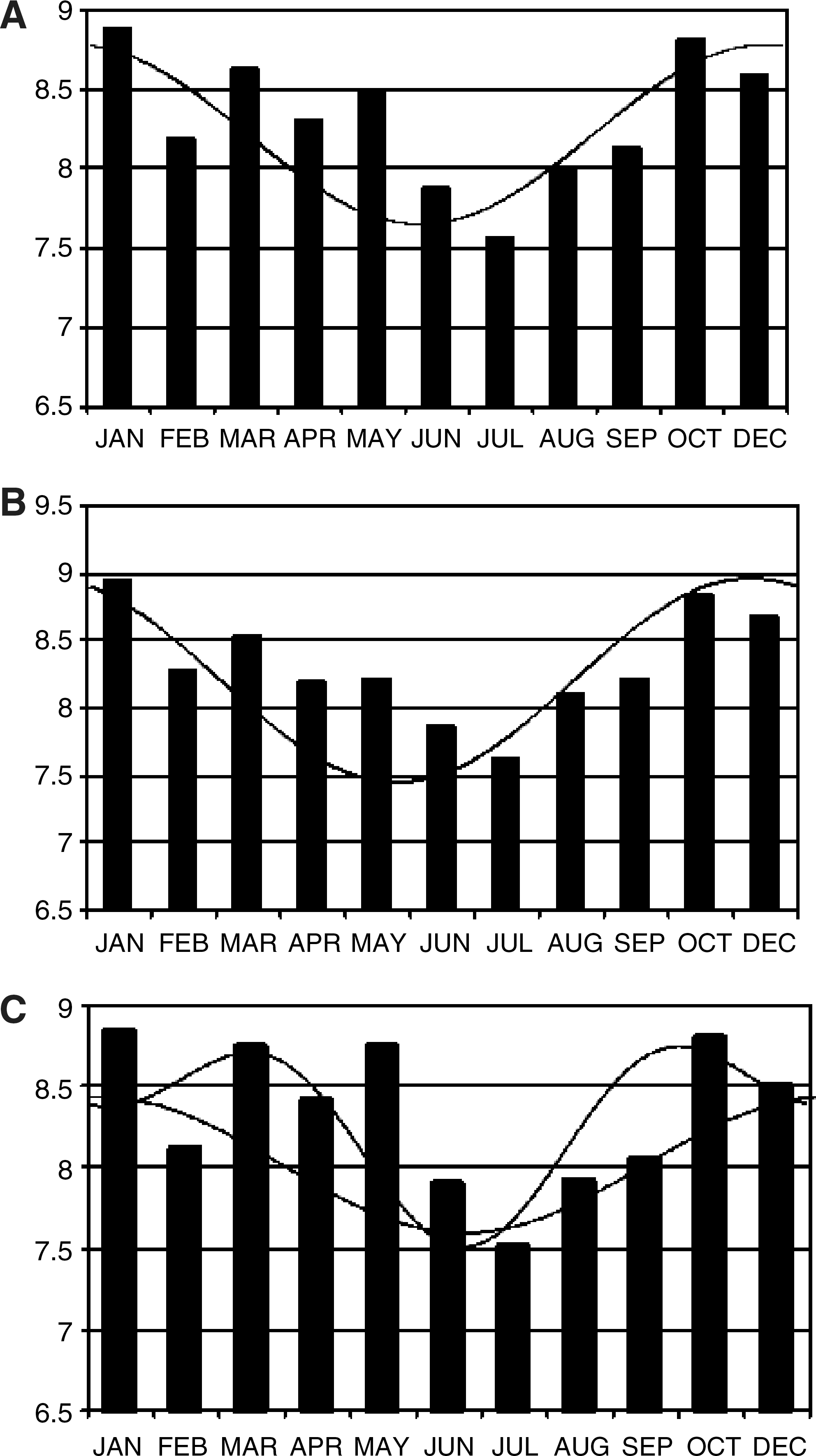
Monthly distribution of hospital admissions (percentage of events) for acute cardiovascular (CV) events. (
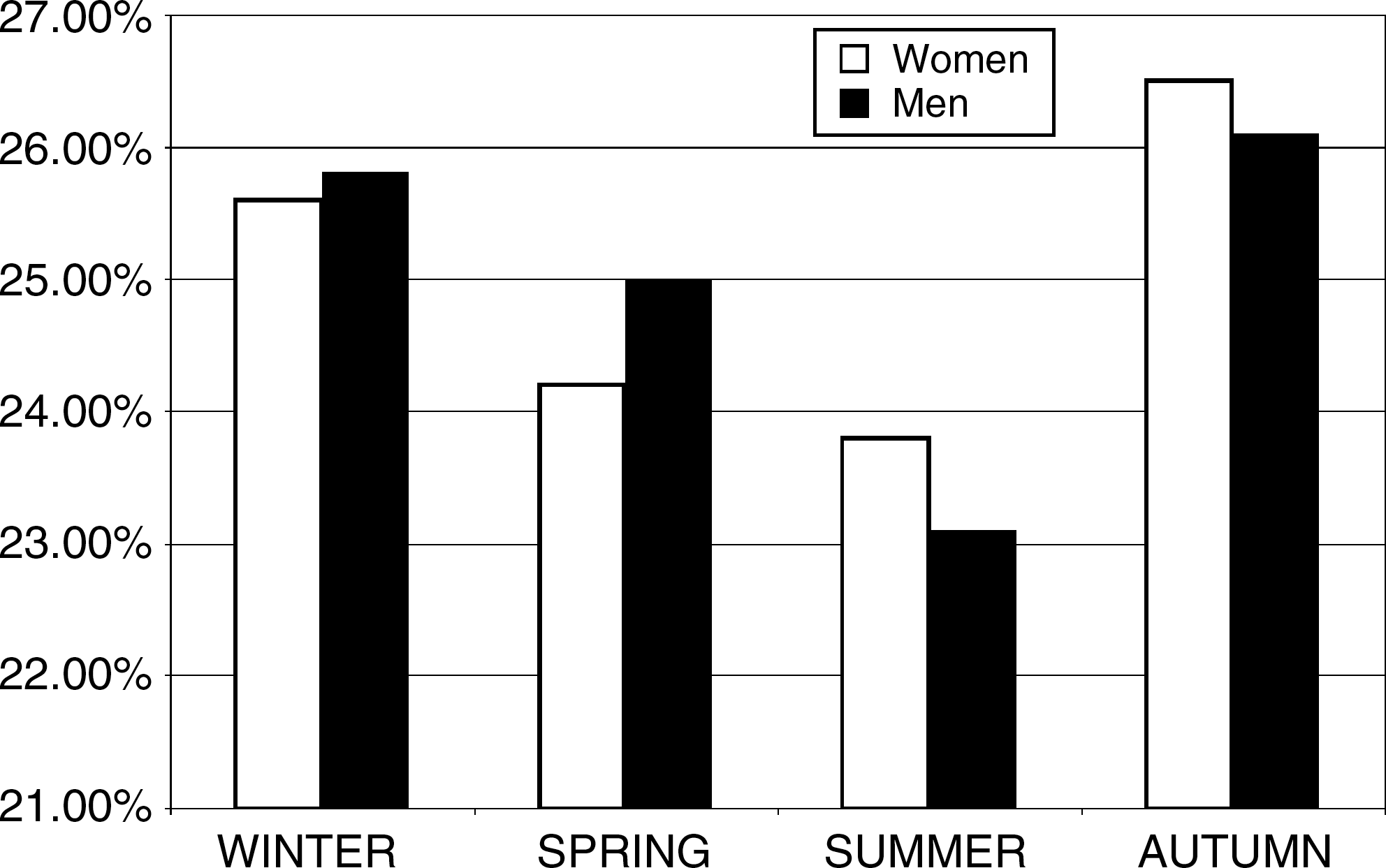
Seasonal distribution of hospital admissions (percentage of events) for acute CV events. White bars, women; black bars, men.
Between women and men: chi-square=0.291, p=NS; bchi-square=0.127, p=NS; cchi-square=0.062, p=NS; dchi-square=0.044, p=NS; echi-square=0.024, p=NS.
TIA, transient ischemic attack.
Peak (acrophase), the absolute maximum value during the observed period; PR, percentage of rhythm.
Between women and men: chi-square=0.078, p=NS; bchi-square=0.066, p=NS; cchi-square=0.025, p=NS; dchi-square=0.011, p=NS; echi-square=0.027, p=NS.
Day of week
During the considered period, the RER database contained the records of 168,921 patients admitted for CV acute events (64,191 AMI, 56,453 stroke, 43,642 TIA, 4,615 AD; 45.6% females). The weekly distribution (percentage of daily events) showed a peak on Monday and a trough on Sunday (Fig. 3), with no differences between CV single disease and gender (Table 4).
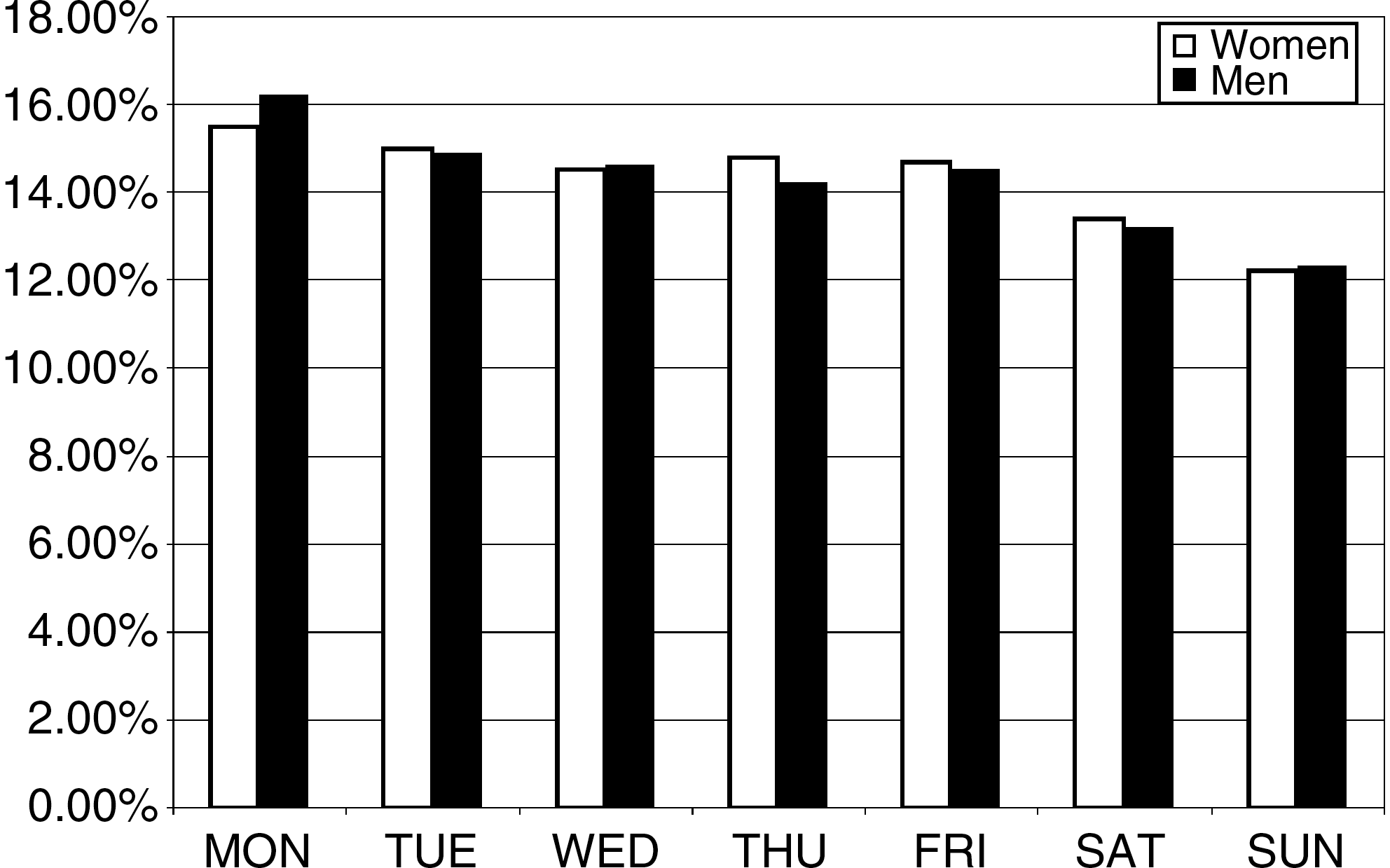
Day-of-week distribution of hospital admissions (percentage of events) for acute CV events. White bars, women; black bars, men.
Between women and men: chi-square=0.218, p=NS; bchi-square=0.109, p=NS; cchi-square=0.053, p=NS; dchi-square=0.032, p=NS; echi-square=0.032, p=NS.
A multivariate regression logistic analysis, including in the model major CV risk factors (hypertension, dyslipidemia, diabetes mellitus) and subgroups by age (<60, 60–69, 70–79, >80 years), did not find any difference in the temporal distribution, either monthly/seasonal or weekly, of events between women and men.
Discussion
Gender does not seem to influence the seasonal or weekly preference in the occurrence of CV events, with winter–autumn and Monday confirmed to be higher risk periods. As for the seasonality of CV diseases, this is not surprising, as several factors, for example, variations in blood pressure (BP), lipids, endothelial function, markers of inflammation, and endogenous factors, may play a role, 23 but with no significant differences among men and women. Arterial BP rises in winter in both sexes, with increases greater in older than in younger subjects. 24 Winter peaks in plasma total cholesterol and low-density lipoprotein cholesterol (LDL-C), have been reported as well, 25 and this pattern is independent of gender, body mass index (BMI), overall diet, or physical activity. 26 Seasonal variations in endothelial function and markers of inflammation have been found, with no differences between men and women. In the large population (n=1,973, 53% women) of the Framingham Offspring Cohort, brachial flow-mediated vasodilatation (FMD) was lowest in the winter, 27 and fibrinogen exhibited significant winter peaks, with changes ranging from 30 mg/dL to 70 mg/dL in different studies. 28 –30 The seasonal variation in risk factors, however, contributes less to the female gender, as the estimated increase in score risk is 6.8% in men and 3.6% in women. 31 For endogenous rhythms, which are difficult to investigate because of the potentially masking effects imposed by environmental and life habits but are potentially capable of playing a role in the seasonal variation of CV diseases, no significant seasonal differences have been reported between women and men as they have for endocrine and metabolic functions correlated with CV functions. 32
Day-of-week and CV risk
Day-of-week distribution of CV events shows a higher frequency peak on Monday irrespective of gender. As for day-of-week occurrence of myocardial infarction, Willich et al. 33 reported a significant increase in relative risk of disease onset on Monday in the working versus nonworking population. A couple of years later, Spielberg et al. 34 did not confirm differences for working and nonworking subjects, that all showed a Monday peak. As for gender, one study in Japan reported a Monday peak in workingmen but not in women, who exhibited a peak on Saturday. 35 Thus, a weekend stressful burden for women was hypothesized by the authors. A Monday peak, irrespective of age and gender, also has been reported for cardiac arrest. 36 A meta-analysis investigated the excess risk associated with the Monday peak in CV mortality and found an increased pooled odds ratio (OR) of 1.19, with no significant differences between subgroups by gender and age. 37 Stress from commencing the weekly working activity, higher BP levels, and unfavorable biochemical status have been proposed as potential triggering factors. 38,39 In the present ICD-9 code-based study, we did not have any information about working activity, and this represents a limitation. As we did not find differences in subgroups by age (and age may be correlated with working activity), however, it can be presumed that the Monday preference is independent of working activity. Regarding risk factors, in a previous study from our group, the higher Monday frequency of stroke was independent of the presence of arterial hypertension, diabetes mellitus, and dyslipidemia, 40 and the present results provide further confirmation for total CV events also.
Conclusions
At least for the time of acute onset, there are no differences among men and women, and to the best of our knowledge, this the first study to investigate such a hypothesis. This is not surprising, as no significant temporal variations by gender have been reported for classic CV risk factors. However, the study of biologic clocks and human rhythms is a novel, greatly expanding field of research. Recent original research opened the possibility that a molecular mechanism intrinsic to the cardiomyocyte, such as the circadian clock, and its alterations may contribute to the temporal variation of CV disease. 41 At present, we do not know of gender differences in the circadian molecular mechanisms in humans. Further studies are needed to explore the intriguing possible relationship among biologic rhythms, CV disease, and gender.
Footnotes
Acknowledgments
We thank Dr Franco Guerzoni and Dr Nicola Napoli, Health Statistics Unit, Azienda Ospedaliera-Universitaria, Ferrara, Italy, for their valuable support. This work was supported in part by an institutional research grant from the University of Ferrara (Fondo Ateneo Ricerca).
Disclosure Statement
There are no commercial associations or competing financial interests or competing interests, actual or potential, for any of the authors.