
Abstract
This literature review focuses on contraception in perimenopausal women. As women age, their fecundity decreases but does not disappear until menopause. After age 40, 75% of pregnancies are unplanned and may result in profound physical and emotional impact. Clinical evaluation must be relied on to diagnose menopause, since hormonal levels fluctuate widely. Until menopause is confirmed, some potential for pregnancy remains; at age 45, women's sterility rate is 55%. Older gravidas experience higher rates of diabetes, hypertension, and death.
Many safe and effective contraceptive options are available to perimenopausal women. In addition to preventing an unplanned and higher-risk pregnancy, perimenopausal contraception may improve abnormal uterine bleeding, hot flashes, and menstrual migraines. Long-acting reversible contraceptives, including the levonorgestrel intrauterine system (LNG-IUS), the etonogestrel subdermal implant (ESI), and the copper intrauterine device (Cu-IUD), provide high efficacy without estrogen. LNG-IUS markedly decreases menorrhagia commonly seen in perimenopause. Both ESI and LNG-IUS provide endometrial protection for women using estrogen for vasomotor symptoms. Women without cardiovascular risk factors can safely use combined hormonal contraception. The CDC's Medical Eligibility Criteria for Contraceptive Use informs choices for women with comorbidities. No medical contraindications exist for levonorgestrel emergency-contraceptive pills, though obesity does decrease efficacy. In contrast, the Cu-IUD provides reliable emergency and ongoing contraception regardless of body mass index (BMI).
Introduction
T
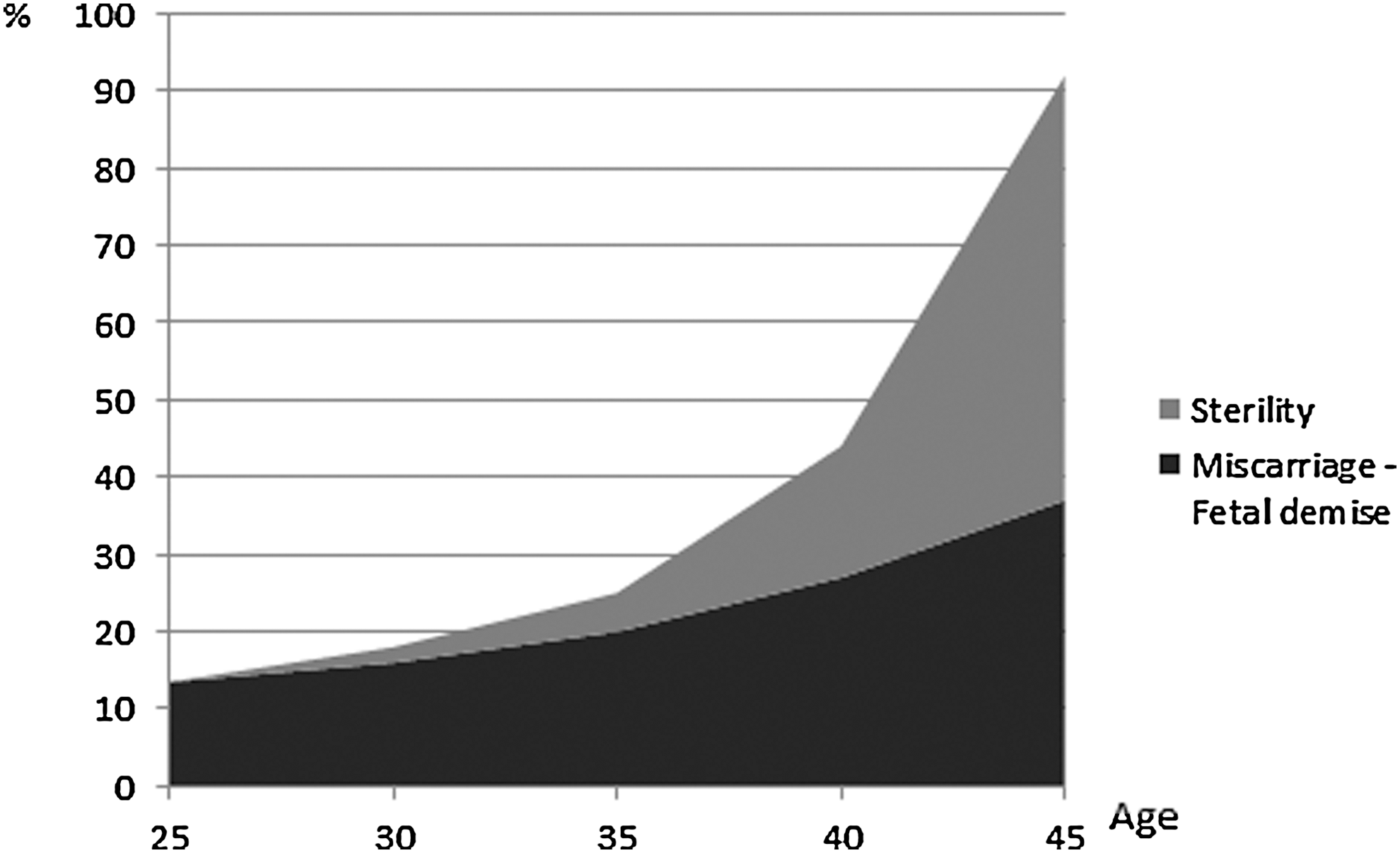
Rates of sterility and miscarriage: fetal demise vs. maternal age.
The US Department of Health and Human Services has reported a rise in the fertility rate among women aged 40–44 and those aged 45–49 over the past 2 decades. 3,4 Almost half of all pregnancies in the United States are unintended; that rate is almost 75% in women over age 40. 5 Further, the proportion of induced abortions as compared to live births in women over age 40 is similar to that of women 20–24 years old. 6 Reported sterility rates are 17% by age 40, 55% by age 45, and 92% by age 50. 7 Although the likelihood of pregnancy is lower in women in their 40s, pregnancy occurs and outcomes are often poor. 8 Therefore, effective and safe contraception for women over the age of 44 is recommended if a woman wishes to avoid pregnancy 8 until the diagnosis of menopause can be made with confidence.
Perimenopausal Changes Affecting Fecundity and Fertility
Perimenopause, as defined by the North American Menopause Society, is the interval from the onset of menstrual changes and menopause-associated symptoms through 1 year after the cessation of menses. 9 This transition may last longer than 6 years and requires management of contraception and menstrual irregularity in addition to other symptoms from hormonal fluctuation. During perimenopause, ovulation becomes less prevalent and the menstrual cycle length increases. However 25% of long cycles greater than 50–60 days may be ovulatory; even intermittent ovulation necessitates effective contraception. 10
Aneuploidy from aging oocytes is a major component of declining fecundity beginning in the late 30s, as many aneuploid pregnancies end in miscarriage or stillbirth. 10 Further, factors other than age also shape a woman's overall reproductive potential. Increasing parity is associated with later menopause. 11 Smoking is associated with slightly earlier menopause and lower fertility. 11 Male partner's age, semen quality, and sexual function combined with the couple's coital frequency further alter fecundity. 10
Diagnosis of Menopause
As a result of hormonal fluctuations during perimenopause, hormone measurement alone cannot effectively confirm menopausal status. 12 Although the mean follicle-stimulating hormone (FSH) level can start increasing up to 7 years prior to the cessation of menses, it escalates more rapidly in the last 2 years, but trajectories vary and are impacted by body mass index (BMI) and race/ethnicity. 13 Estradiol (E2) levels are generally normal up to 1 year prior to the cessation of menses and then begin to decline, though this decline may begin years earlier for some women. 13
With this variability, neither FSH nor E2 levels are accurate indicators of menopause. 14 A clinical history is best for assessing menopausal status and most commonly includes changing menstrual patterns, along with symptoms of hot flashes and changes in mood and sleep. 12 Toward the late transition, FSH will be >30 international units per liter (IU/L) and luteinizing hormone >20 IU/L 10 ; however, this is highly variable even with a repeat sampling. 15 An antimüllerian hormone level is also inadequate for diagnosing menopause. 16 Educating patients and healthcare providers regarding the importance of a clinical diagnosis of menopause will ensure appropriate utilization of laboratory tests.
Obstetric Issues in the Older Gravida
As compared with younger women, the obstetric outcomes in older women are often poorer and the rates of miscarriage and stillbirth higher. 17 Pregnancies that do not result in live births may have a significant emotional and physical impact. Maternal comorbidities, including gestational and chronic diabetes, pregnancy-associated hypertension, chronic hypertension, and eclampsia, all increase with age. Age-related differences in rates of diabetes and chronic hypertension are most striking. Per 1,000 live births, women aged 40–54 have diabetes and hypertension rates that are three and four times that of women aged 20–29, respectively. Even more concerning, maternal mortality in women ages 35 and older is 32.3 deaths per 100,000 live births as compared with 7.1–12.1 per 100,000 live births in younger women. 17 Therefore, appropriate contraception may be medically indicated in the setting of comorbidities.
Contraceptive Trends
Long-acting reversible contraception (LARC), including etonogestrel subdermal implant (ESI), levonorgestrel intrauterine system (LNG-IUS), and copper intrauterine device (Cu-IUD), is extremely efficacious in reducing unintended pregnancy. 18,19 The CDC US Medical Eligibility Criteria for Contraceptive Use (MEC) guidelines recommend LARC to women throughout their reproductive lifetime and inform contraceptive choices for perimenopausal women with coexisting medical conditions, using a rating scale of 1=no restriction on use, 2=benefits outweigh risks, 3=risks outweigh benefits, and 4=unacceptable health risk. 20
The American College of Obstetricians and Gynecologists (ACOG) also supports LARC. 21 Growing patient acceptance of LARC in the United States is evidenced by increased LARC use at 8.5% in 2009 as compared with 3.7% in 2007. 22 Further, patients prefer LARC. As part of the Contraceptive CHOICE Project, participants received contraceptive counseling and cost-free access to all methods. Among the initial 2,500 women enrolled, 67% chose LARC. 23 Pregnancy was less common across all age groups in the LARC vs. the non-LARC groups, which used pills, patches, or ring. 24
Contraception in Perimenopausal Women
LARC
Highly efficacious and estrogen-free, LARC is especially advantageous to perimenopausal women, in whom contraindications to estrogen may exist. With contraceptive efficacies similar to sterilization, many women opt for contraception initiated in an office setting rather than the operating room. Recently, the Food and Drug Administration (FDA) packaging for the LNG-IUS 25 and the Cu-IUD 26 has been updated to more closely reflect true medical contraindications to placement. The CDC US MEC notes few absolute contraindications to the placement of intrauterine contraception (IUC), as detailed in Table 1. 20,27 Obese women have no restriction on IUC use and are not at increased risk of method failure. 20
Data from the Centers for Disease Control and Prevention. 20 (Adapted from Marnach ML, Long ME, and Casey PM. Current issues in contraception. Mayo Clin Proc 2013;88:298. Used with permission.)
When indicated, sexually transmitted infection (STI) screening can be performed on the day of IUC placement. 8 Asymptomatic women testing positive at insertion or later and women with pelvic inflammatory disease who respond to antibiotics in the first 48–72 hours do not need to have the IUC removed. 8 However, symptomatic cervicitis, gonorrhea, and chlamydia are temporary contraindications to initiating IUC according to CDC US MEC, though some believe that this recommendation and a 3-month posttreatment deferral of IUC are overly conservative. 28
Abnormal vaginal bleeding requires evaluation prior to IUC placement. This is especially important in perimenopausal women, who carry a higher risk of endometrial cancer. 29 Adequately evaluated vaginal bleeding of benign etiology, nulliparity, prior ectopic pregnancy, HIV disease, pelvic inflammatory disease more than 3 months ago, prior STI, uterine fibroids that do not preclude placement, and nonmonogamous relationships are no longer considered IUC contraindications. 30
IUC indications have expanded beyond contraception alone. The 52 mg LNG-IUS has received FDA approval for treatment of menorrhagia in women needing contraception. Owing to increasing anovulation, perimenopausal women are more likely to suffer from prolonged or heavy vaginal bleeding. 29 After the first year, menstrual blood loss is reduced by 75%–95%, with many women experiencing hypomenorrhea or amenorrhea. 30 IUC insertion may be followed by 3 to 6 months of irregular spotting and bleeding, and appropriate counseling alleviates concern and maximizes patient satisfaction. 25 The LNG-IUS reduces anemia more effectively than combined hormonal contraception (CHC). 31 Anticoagulation and bleeding diathesis do not impair the effectiveness of the LNG-IUS. 32 In the United Kingdom, there has been a notable decrease in hysterectomies for benign disease since the introduction of the LNG-IUS. 32 The LNG-IUS has also been used to treat another condition more common in perimenopausal women: simple endometrial hyperplasia. 32 In addition, the satisfaction and continuation rates are high for this cost-effective LARC. 33
The ESI brought an implantable contraceptive and another LARC option back to the United States. This single-rod implant is easily inserted and removed by a trained provider in an office setting. Post-FDA approval data have demonstrated efficacy in obese women. 34 Unlike other LARC, ESI provides ovarian suppression, potentially improving endometriosis and other conditions affected by cyclic hormonal changes. 35 Additionally, this ovarian suppression does not require estrogen, which is desirable in perimenopausal with certain comorbidities. 20 Although many women find the bleeding pattern with ESI acceptable, around 15% of US women have requested removal for bleeding changes in one US study. 36 Removal rate for bleeding is lower in women with a BMI >30 kg/m2 as compared to those with a lower BMI. 37 Reported management strategies for unacceptable bleeding with ESI include doxycycline, mefenamic acid, and CHC, though lack of clarity persists regarding the relative efficacy of each intervention. 38 –40
Non-LARC hormonal contraception
Developments in CHC have offered women more choices than ever while maintaining contraceptive efficacy. Formulations with estrogen doses as low as 10 mcg are available. Newer progestins have addressed many of the androgenic CHC side effects. Oral CHC remains a popular choice, given its flexibility, convenience, and well-known noncontraceptive benefits. Oral CHC is available in cyclic (21 active pills/7 inactive pills), shortened hormone-free interval (24 active pills/4 inactive pills), extended (84 active pills/7 inactive pills), and continuous (365 active pills) regimens. The latter two decrease or eliminate scheduled menstrual intervals, thus lessening withdrawal vasomotor symptoms and menstrual migraines in perimenopausal women. Vasomotor symptoms occur in more than 60% of perimenopausal women. 41 In CHC users, these symptoms may initially present in the hormone-free interval or placebo week. Estrogen hormone therapy (HT) during the hormone-free interval may be effective in women not using continuous CHC. 41
Extended and continuous CHC regimens are associated with breakthrough bleeding during the initial weeks. This is generally self-limited. 42 CHC can help manage a variety of conditions that continue or worsen as women approach menopause. The shortened hormone-free interval regimens provide cyclicity for those who prefer it yet decrease the risk of symptomatic ovarian cysts. 43 Menses are generally light. Many oral CHC formulations have been successfully used for the treatment of acne. 44 In obese women without other comorbidities, the benefits of CHC typically outweigh the risks, and there is no clear evidence that the efficacy of CHC is altered by obesity. 20 If efficacy is of primary concern, the LARC methods provide at least 10 times greater efficacy with fewer possible safety issues. 20 Although all CHC formulations can be used to treat menorrhagia, which is common in perimenopausal women, the FDC has approved a new estradiol valerate/dienogest quadriphasic oral CHC for treatment of menorrhagia. 45
The contraceptive ring is a CHC alternative that does not require daily attention. It is effective in either a cyclic (in for 3 weeks, out for 1 week) or a continuous (same ring in for 4 weeks, replaced with a new ring right away) fashion. 46,47 The latter option avoids the estrogen-withdrawal symptoms experienced by perimenopausal women, while maintaining contraceptive efficacy. In contrast, concerns about the increased risk of venous thromboembolism (VTE) with the contraceptive patch as compared to that with oral CHC in some but not all studies and the absence of long-term continuous-use safety data make it less appealing for the perimenopausal woman and discourage use in a continuous fashion (using an additional patch each month). 48,49
Perimenopausal women who have a contraindication to the use of estrogen yet prefer an oral contraceptive may choose the progestin-only pill despite its lower contraceptive efficacy as compared with CHC. The progestin-only pill, containing only a progestin and no estrogen, can also provide endometrial protection in women using estrogen HT for the treatment of vasomotor symptoms.
Depot medroxyprogesterone acetate (DMPA) injections are another estrogen-free option not requiring frequent attention. However, association with bone loss, though reversible in many cases, makes this option less than ideal for the perimenopausal woman whose rate of bone loss is greatest in the first few years following menopause. 50 The FDA mandated a black-box warning in the DMPA package insert, recommending discussion and consideration of other options after 2 years of use. However, bone mineral density testing for DMPA users is not recommended. 51 DMPA can be used with or without estrogen HT as transitional contraception. Evidence exists for treatment of vasomotor symptoms with DMPA alone in women with contraindications to estrogen. 52 Other progestin-only contraceptives are not known to have deleterious effects on bone density, based on limited data. 53
CHC benefits
In addition to contraception, perimenopausal women may benefit from CHC to regulate menstrual blood loss, timing, and pain. 31 CHC may also reduce pelvic pain associated with endometriosis. 54 CHC for menstrual migraine or other hormonally related headache may benefit perimenopausal women. In these women, extended-cycle (24/4 or 84/7) or continuous CHC is most effective. 55
CHC is associated with reduced bone demineralization in perimenopausal women and increases bone density even at low-dose (20 μg E2) formulations. 56 Interestingly, perimenopausal women with oligomenorrhea who used CHC had the greatest improvement in menopausal fracture risk. 56
Additional CHC benefits include reduced endometrial and ovarian cancer risk. Endometrial cancer risk is reduced by 40% in women using CHC for 12 months or longer, with protection lasting at least 15 years after CHC discontinuation. 57 Ovarian cancer risk is reduced by >50% after 15 years of CHC. Protection persists at least 30 years after CHC discontinuation. 58
CHC risks
The absolute risk of thrombotic stroke (TS) and myocardial infarction (MI) associated with CHC is low in women of reproductive age but increases with age, E2 dose, and the presence of additional cardiovascular risk factors, such as smoking and hypertension. A recent systematic review and meta-analysis showed a twofold increased risk of thrombotic stroke with oral CHC use but an indeterminate effect on the risk of MI. However, it is important to note that the analysis of stroke risk did not differentiate between low- and high-dose E2 (defined as less than vs. greater than 35 μg E2 in this study). Further, the authors note that insufficient studies were available to differentially calculate risks based on age or other cardiovascular risk factors. 59
In a Danish study, the largest to date assessing the risk and incidence of TS and MI in CHC users, the incidence of TS and MI increased by a factor of 20 and 100, respectively, in women aged 45–49 as compared with women aged 15–19, after adjusting for CHC use or nonuse. Notably, no consistent interaction was noted between the relative risk of TS or MI and the use of oral contraceptives in different age groups. With CHC containing 20 μg E2, the risk of TS and MI altered by a factor of 0.9–1.7, while the risk increased by a factor of 1.3–2.3 with CHC containing 30–40 μg E2. 60 To put this in perspective, the incidence of TS in reproductive-age women is about 1 per 10,000 women a year; with CHC use, the risk of TS increases twofold. In contrast, pregnancy and the postpartum state increase risk of TS by three- to eightfold. 59
With the use of a contraceptive patch or ring, the relative risk of thrombotic stroke was 3.15 (95% confidence interval [CI], 0.79–12.6) and 2.49 (95% CI, 1.41–4.41), respectively. 60 There were small differences in thrombotic stroke and MI risk with progestin type. Progestin-only products, including LNG-IUS and ESI, were not associated with an increased risk of TS or MI. Further, they have not been associated with an increase in blood pressure or alteration in clotting parameters. 61
Although older CHC formulations have been associated with a slightly increased risk of breast cancer, lower E2 formulations have not. 62 Furthermore, a recent population-based study revealed no increased risk of breast cancer in women aged 35–64 who were current or former CHC users, regardless of formulation. 63
Although there is no restriction to Cu-IUD use in women with breast cancer, the CDC US MEC recommends caution with LNG-IUS, though no supporting references were given. 20 Limited evidence from a small case-control study of women who continued their LNG-IUS after their breast cancer diagnosis or received it shortly thereafter did not clearly demonstrate an increase in recurrence risk overall in the 79 women (adjusted hazard ratio 1.86; 95% CI 0.86–4.00). An elevated adjusted hazard ratio of 3.39 noted in women continuing their LNG-IUS after diagnosis is of some concern, but the confidence interval was wide (95% CI 1.01–11.35). 64 LNG-IUS may be especially advantageous in perimenopausal women with menorrhagia undergoing chemotherapy, since it is highly effective in reducing menstrual blood flow and has lower systemic hormone levels than other therapy routes. 65 The newly FDA-approved 13.5 mg LNG-IUS has even lower circulating progestin levels and is expected to have lower menstrual blood loss than Cu-IUD but has not yet been studied in the setting of breast cancer. 25,66
Both the low absolute number of VTE events with CHC and the higher VTE risk in pregnancy and the postpartum period need to be considered. In a cohort of US women, the incidence of VTE per 10,000 was 4.4 nonpregnant/not postpartum, 9.6 in pregnancy, and 51.5 postpartum. 67 A European study reported a VTE incidence of 4.4 per 10,000 in nonpregnant women not using CHC, 8–9.0 per 10,000 CHC users, and 29.1 per 10,000 pregnant women. 65 Of concern is that increased VTE risk begins in the first trimester of pregnancy. 68 These incidence rates of VTE per 10,000 can be compared to rates of 6–15 for the population age 50–59 years and 30–50 for age 70–79 years. 69
Discovery of variation in VTE risk with type of progestin in CHC has increased concerns regarding progestin choice. VTE risk variation among progestins is summarized in Table 2. 70 A black-box warning recommends that healthcare providers discuss VTE risk with drospirenone and offer alternatives, given the reported increased VTE risk associated with this progestin and other third-generation progestins as compared with levonorgestrel. 71 –73 No specific recommendations currently exist relating to etonogestrel-containing contraception. 74,75 Nonetheless, the side-effect profile with less androgenic progestins may impact the prescribing decision.
Adjusted for age, duration of use, year of use, and education.
CI, confidence interval; VTE, venous thromboembolism.
Barrier and fertility-awareness methods
Although much less efficacious than LARC and hormonal contraception, barrier contraception and fertility awareness may be considered adequate by some perimenopausal women. Condom use is recommended to decrease STI risk. Fertility-awareness methods are more difficult to practice in perimenopausal women, owing to fluctuating cycle lengths and unreliable midcycle symptoms. 76 Women choosing these methods should specifically be counseled about the availability, efficacy, and safety of emergency contraception (EC), given the higher pregnancy rates and greater opportunity to identify user and method failure with barrier contraception and fertility-awareness methods.
Emergency contraception
The World Health Organization and the CDC state that there is no medical condition wherein the risks of EC outweigh its benefits. 20 The EC mechanism of action involves the delay or suppression of ovulation; thus, it does not interfere with an established pregnancy but should be administered as soon as feasible after unprotected coitus. Levonorgestrel EC is given as a single oral dose within 72 hours of unprotected coitus and is available without a prescription. Ulipristal EC is given as a single oral dose up to 5 days following unprotected coitus and requires a prescription. Cu-IUD (but not LNG-IUS) may be used up to 5 days following unprotected coitus and had only a 0.09% pregnancy rate in more than 7,000 placements for postcoital contraception. 77 At 12 months postinsertion for EC, 94% of parous and 88% of nulliparous women retained the Cu-IUD for primary contraception. 78 Further, Cu-IUC is the preferred EC for women with a BMI greater than 30 kg/m2, owing to a higher failure rate with LNG-IUS and ulipristal EC. For a similar reason, ulipristal is preferred over LNG-IUS for women with a BMI of 25–30 kg/m2. 79
Sterilization
In the United States, sterilization of one partner is the most widely used contraception. In particular, women over age 40 utilize sterilization at a higher rate (38.1%) than women overall (16.5%). 80 Female tubal sterilization, vasectomy, and LARC have similar efficacy. 81 The complication and mortality rates with female sterilization are higher than those associated with LARC and vasectomy but much lower than those associated with pregnancy. Vasectomy is a low-cost office procedure performed under local anesthesia with few complications and virtually no risk of mortality. 81 No increase in arthrosclerotic disease, sexual dysfunction, testicular and prostatic cancer, or immunologic disease has been reported with vasectomy. 81 Laparoscopic tubal sterilization typically requires general anesthesia and incurs a risk of intra-abdominal injury and thromboembolism. 71 About a third of pregnancies after female sterilization are ectopic. Nonetheless, this rate is lower than the rate in women not using contraception. 81 Hysteroscopic sterilization offers efficacy and cost effectiveness while avoiding general anesthesia and virtually all intra-abdominal injury risk. A nickel allergy is no longer considered a contraindication to hysteroscopic sterilization. 81 Unlike immediately effective laparoscopic sterilization, both vasectomy and hysteroscopic sterilization require weeks to months to become effective; therefore, bridging contraception is necessary. 81 A hysterosalpingogram is required at about 3 months postprocedure to confirm tubal occlusion.
Postpartum and laparoscopic sterilizations are associated with a lower risk of pelvic inflammatory disease and ovarian cancer. Laparoscopic sterilization has not been associated with sexual dysfunction, dysmenorrhea, or menorrhagia. There are no data regarding these benefits after hysteroscopic sterilization. Sterilization regret is lower in women over age 30. 81
When Both Contraception and HT Are Needed
If a woman is not yet menopausal, contraception is required with HT. LNG-IUS provides years of contraception and endometrial protection when administered with estrogen HT. 82 LNG-IUS is particularly suited for use in perimenopausal women who experience heavy menses. 83 The intrauterine progestin delivery has the added advantage of protecting against endometrial hyperplasia while avoiding potential side effects associated with an oral progestin. 82 The progestin-only pill also provides endometrial protection with estrogen HT. Although CHCs are relatively contraindicated for women experiencing migraine with aura, postmenopausal HT is not contraindicated in these patients. 84 For management of vasomotor instability, a transdermal preparation of estrogen is suggested, utilizing the lowest effective dose for the shortest duration needed to control symptoms. 82,84
Progestin doses adequate for HT endometrial protection are not adequate for ovulation suppression. 85 The ideal time to transition from contraception is following 12 consecutive months of amenorrhea when fecundity is extremely low. 10 When menopausal amenorrhea is obscured by hormonal use and ongoing contraception is desired, hormonal contraception can be continued until age 56, when the likelihood of spontaneous menopause is 95%. 86 Discontinuation of contraception at age 45 will prevent most live births, but pregnancy can still occur. 10 Although these pregnancies almost always result in fetal loss, 2 they still expose women to complications, such as hemorrhage and VTE. 10 Continuing hormonal contraception rather than observing for amenorrhea during a hormone-free interval also prevents estrogen-withdrawal symptoms.
Conclusion
In the perimenopausal years, women need contraception to avoid unintended pregnancy. Menopause is diagnosed by clinical history or can be safely assumed at age 56, when its likelihood is 95%. 86 Inconveniently, laboratory testing does not reliably confirm menopause. Perimenopausal women may also have coexisting issues, including migraines, menorrhagia, and vasomotor symptoms, and may therefore benefit from treatment with progestin, estrogen, or both. The absolute risk of VTE and cardiovascular complications with CHC is low in appropriately selected patients and is much lower than that associated with pregnancy or the postpartum period. CHC is associated with noncontraceptive benefits, including reduced risk of endometrial and ovarian cancers. Low-dose formulations are not associated with an increased risk of breast cancer. LARC is emerging as a highly efficacious, safe, and convenient contraceptive class and should be considered as first-line contraception across the reproductive lifespan. Both LNG-IUS and CHC are efficacious in managing the menorrhagia that commonly plagues perimenopausal women. Progestin-only LARC may be used as contraception and also endometrial protection in conjunction with estrogen HT. EC is an option for all women, but hormonal EC is less effective in women with an elevated BMI. Therefore, Cu-IUD should be considered for EC and potentially long-term contraception in these women. The CDC US MEC serves as an excellent resource to inform contraceptive choices in women with coexisting medical conditions.
Footnotes
Acknowledgment
The authors thank Gladys Hebl for assistance in preparing this manuscript.
Author Disclosure Statement
Margaret E. Long and Petra M. Casey, certified IMPLANON® and NEXPLANON® trainers not receiving payment for training services, receive research support from Merck. No support was received from any other entity for this project. No competing financial interests exist for Stephanie S. Faubion, Kathy L. MacLaughlin, or Sandhya Pruthi.