
Abstract
Background:
Intermittent claudication (IC) and its consequences have customarily been underestimated in women. Our study aimed to determine the differences on functional and quality-of-life issues between women and men in a large group of claudicants.
Methods:
This study was an observational, cross-sectional, nonrandomized, multicenter study of 1,641 claudicants (406 women). Information was collected from patients' medical history, a physical examination, the ankle-brachial index (ABI), the Walking Impairment Questionnaire (WIQ), and the European Quality of Life Questionnaire (EQ-5D).
Results:
On average, women with IC were older than men with IC (70.0 vs. 67.8 years; p<0.001) and tended to have a different socio-occupational status. Women were more likely to be obese and less likely to smoke or have dyslipidemia (p<0.001). Women were notable for their greater prevalence of cardiac insufficiency (p=0.016) and arrhythmias (p<0.001) and a lower prevalence of ischemic cardiopathy and acute myocardial infarction (p<0.001). At the same time, there was a significantly higher level of osteoarticular diseases in women: arthrosis (p<0.001), arthritis (p<0.001), and lumbar pathology (p=0.006). All the symptoms evaluated that were associated with IC were more frequent in women (p<0.05). The mean ABI was similar in claudicant women and men. Conversely, the parameter estimates of the WIQ were significantly lower in women (by 4.3%, and 6.5%, respectively; p=0.003). Likewise, the EQ-5D score was 7% lower in women than in men (from 0.52 to 0.59; p<0.001).
Conclusions:
Women claudicants have higher risk factors and more frequent cardiovascular comorbidity than men do. Women have a lower capacity for exercise and a poorer quality of life than male claudicants, despite having a similar ABI. These poorer outcomes in women can be partially explained by the presence of greater osteoarticular comorbidity.
Introduction
I
Lower frequencies of PAD and IC have customarily been reported in women. The review by Higgins and Higgins, 6 considering research carried out over 5 decades, showed that the prevalence of PAD in women aged between 45 and 93 years of age was 3%–29%. This difference has been explained in terms of women's lower level of physical activity, the presence of atypical symptoms that are not characteristic of IC, women's different perception of their symptoms, and a combination of all these. 7–8 The current estimates of the prevalence of IC by sex are not clearly defined. Thus, although the women with IC accounted for only 30% of all claudicants in the aforementioned Spanish study, 5 the two sexes each accounted for around 50% of all claudicants in a Norwegian study. 9
Nonetheless, it seems clear that women with PAD suffer similar mortality and morbidity consequences as do men. 10 It is also significant that clinical 8,11 and health-related quality of life (HRQL) 12 aspects of women with PAD differ from those of men with the condition and that these differences are also present in the subgroup of women with claudication. This finding has specific diagnostic and therapeutic implications. 13,14 In this context, the objective of our study was to determine whether there are sex-based differences on functional and quality-of-life issues between women and men in a large group of claudicants. These findings will be useful in guiding future regional and national efforts in Spain toward educating the public about cardiovascular conditions.
Materials and Methods
Study population
We designed an observational, cross-sectional, nonrandomized, multicenter study covering the entire Spanish nation. The sample population comprised 2,127 patients with IC. Participating patients had to fulfill all inclusion criteria and none of the exclusion criteria (Fig. 1). All participants signed an informed-consent form. Between May and December 2011, 625 research physicians recruited patients. Each researcher was asked to provide three to four IC-diagnosed patients, who consecutively attended a consultation (60% in hospitals and 40% in health centers of the Spanish National Health System). The IC diagnosis was based on a medical history (including the Edinburgh Claudication Questionnaire), 15 a physical examination, and the ankle-brachial index (ABI). The study was approved by the Scientific and Ethics Committee of the Clinical Hospital, Barcelona, Spain (Protocol: SEA-NUL-2011-01).
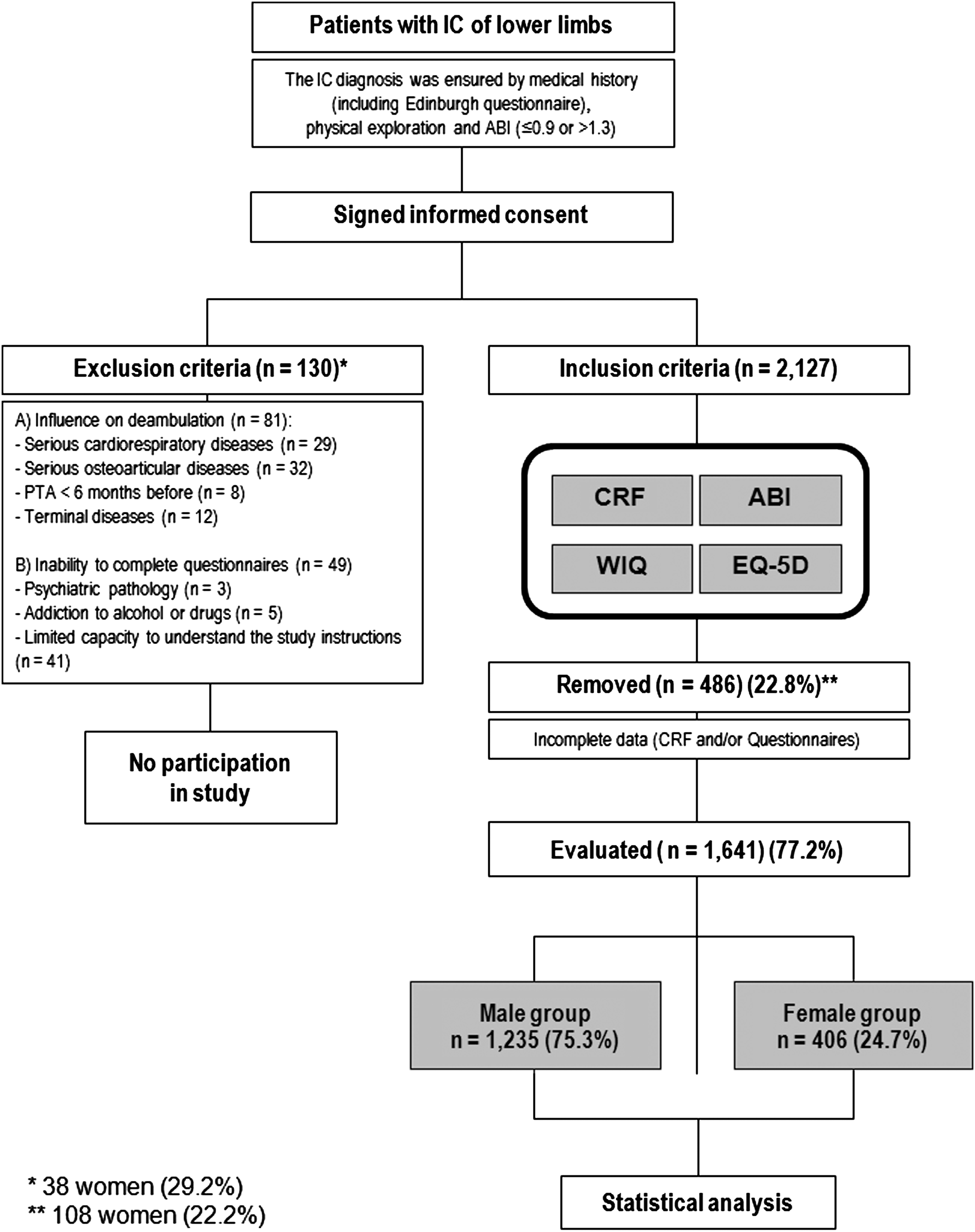
Study design; criteria for inclusion, exclusion, and withdrawal of patients (and number). ABI, ankle-brachial index; CRF, case-report form; EQ-5D, European Quality of Life Questionnaire; IC, intermittent claudication; WIQ, Walking Impairment Questionnaire.
Inclusion criteria were IC of lower limbs (Fontaine grade II) lasting for more than 1 year; either gender, aged between 45 and 85 years; and any race. Exclusion criteria were failure to obtain consent to participate in the study; conditions influencing ambulation in an absolute manner, such as serious cardiorespiratory diseases, chronic obstructive pulmonary disorders, or cardiac insufficiency; those presenting dyspnea with moderate effort, such as climbing one flight of stairs or requiring daily oxygen therapy at home; serious osteoarticular diseases; arthroses of any form such as those requiring assisted deambulation (help from relatives, use of two sticks or similar, including walking frames) or morphine-based pain relief; surgery or percutaneous transluminal angioplasty (PTA) (<6 months before) that can improve the conditions of prior claudication; acute or critical arterial ischemia presenting with permanent pain in the extremities; terminal illnesses (oncological or other) that can affect ambulation due to weakness; and situations that alter the ability to complete questionnaires: psychiatric pathology, addiction to alcohol or drugs, and the patient's inability to answer questionnaires or understand the instructions pertaining to the study.
Measuring instruments
The researcher filled in a case-report form (CRF) that included a standardized questionnaire about demographic, socio-occupational, and clinical data (cardiovascular risk factors, comorbidity, etc.), analyses (basal blood glucose, total cholesterol, and lipid profile), and the ABI. At the same time, patients completed a self-reported questionnaire about their walking performance (Walking Impairment Questionnaire [WIQ]) and one about their quality of life (European Quality of Life Questionnaire [EQ-5D]). The confidentiality of patients' responses to the questionnaires was respected through anonymization.
ABI
A portable Doppler apparatus (8 MHz probe) was used, a technique recommended by the American Heart Association. 16 The record of each patient took into account only the extremity with claudication or, for cases of bilateral claudication, that with the lower ABI.
WIQ
This instrument documents the physical deficit of patients with IC. 17 It investigates three domains: (1) the distance that patients manage to walk, (2) the speed they achieve, and (3) the number of stairs they manage to climb. Scores for each domain may vary between 0% (complete incapacity) and 100% (complete capacity). The Spanish version of the WIQ was used. 18
EQ-5D
We used the first and second parts of this generic quality-of-life questionnaire. 19 The first part evaluates the state of health of patients across five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Scores are summarized as an overall index between 0 (worst health status) and 1 (best health status). The second part consists of a visual analog scale (VAS), running from worst to best imaginable health status (scored 0 and 100, respectively). We used the Spanish version of the questionnaire. 20
Statistical analysis
Data were collated anonymously and the necessary tabulations done with PASW Statistics version 18 (IBM, New York, NY). Results of continuous variables are presented as the mean and standard deviation (SD); categorical variables are summarized as frequencies and percentages. Continuous variables were examined to determine whether they were normally distributed and thereby the most appropriate test. Qualitative variables were compared with the chi-square or Fisher's Exact Test. In the case of continuous dependent variables, the independent-samples t-test or the Mann-Whitney U test were used to compare values for two groups, and analysis of variance (ANOVA) or the Kruskal-Wallis test were used to compare more than two groups. Statistical significance was concluded for values of p<0.05. A multivariate linear regression was carried out to determine the importance of the 39 independent variables in explaining the results of the WIQ (distance) and the EQ-5D (global score).
Results
Of the 2,127 patients, 486 were excluded from the study owing to incomplete data (CRF and/or questionnaires). Of the 1,641 remaining claudicant patients, 406 (24.7%) were women.
Women were 2.2 years older than men on average (70.0 vs. 67.8 years; p<0.001). The socio-occupational status of women tended to be different from that of men, there being a higher percentage of widows (40.9% vs. 15.0%; p<0.001), those living alone (27.6% vs. 18.9%, p<0.001), those off work (6.9% vs. 4.0%), and retirees (69.7% vs. 65.9%; p=0.008).
With respect to the cardiovascular risk factors, lower proportions of women exhibited dyslipidemia (57.9% vs. 67.5%; p<0.001) or had an active smoking habit (15.0% vs. 42.8%; p<0.001). Obesity (body mass index [BMI]>30) was more frequent among women than men (31.5% vs. 21.5%; p<0.001). Diabetes mellitus and arterial hypertension occurred in similar proportions in women and men. Almost all the women (97%) were postmenopausal.
With respect to cardiovascular antecedents, there was a higher frequency of cardiac insufficiency (12.1% vs. 7.9%; p=0.016) and arrhythmias (13.8% vs. 6.8%; p<0.001) in women compared with men. Conversely, antecedents of ischemic cardiomiopathy (16.5% vs. 26.6%; p<0.001) and acute myocardial infarction (4.2% vs. 12.3%; p<0.001) were less frequent in women. The presence of renal insufficiency and stroke was similar in women and men. Of the osteoarticular diseases, arthrosis (71.7% vs. 45.3%; p<0.001), arthritis (11.3% vs. 4.1%, p<0.001), and lumbar pathology (26.4% vs. 19.8%; p=0.006) were more frequent among women than in men. Other characteristics of the sample are summarized in Table 1.
Women vs. men.
AMI, acute myocardial infarction; BMI, body mass index; CVD, cardiovascular disease; SD, standard deviation.
The associated symptoms of women with intermittent claudication differ from those of men. In addition to the classical symptoms of IC, women had more frequent atypical symptoms than did men (p<0.05). The blood pressure measurements and analytic test results were similar in the two sexes. The mean ABI of the groups was 0.65±0.19 (women) and 0.67±0.19 (men) (p=0.660); the percentage of patients with an ABI<0.50 was similar in women and men. However, all the results from the WIQ and EQ-5D were significantly lower in women. Women's capacities for distance, speed, and stair climbing were even lower (by 4.3%, 4.8%, and 6.5%, respectively) relative to men (p=0.003). Quality of life was 7% lower in women (0.52 vs. 0.59; p<0.001). Table 2 summarizes the determinations implemented. The multivariate analysis reports the independent variables related to the WIQ distance (Table 3) and EQ-5D (Table 4) outcomes.
Women vs. men.
Different from the pain owing to intermittent claudication.
Proximal (femoral or popliteal).
ABI, ankle-brachial index; EQ-5D, European Quality of Life Questionnaire: 0 (worst possible) to 1 (best possible); HDL, high-density lipoprotein; LDL, low-density lipoprotein; WIQ, Walking Impairment Questionnaire: 0% (worst possible) to 100% (best possible).
CVD, cardiovascular disease; BMI, body mass index; ABI, ankle-brachial index.
Adjusted r 2 value in the final model indicates that 67% of the variance in the HRQL summary is not explained by these covariates.
CI, confidence interval; HRQL, health-related quality of life; SE, standard error.
Discussion
Our study indicates how cardiovascular risk factors, comorbidity, and symptoms for women with intermittent claudication differ from those for men. At the same time, women have less capacity for exercise and a poorer quality of life than do male claudicants, despite their similar ABIs.
Although our study features a broad sample of claudicant patients, only 25% were women. However, this fact should be considered in the following contexts. (1) A Spanish-population study, using similar diagnostic criteria, contained 30% of claudicant women. 5 (2) Our study design did not allow us to study to the prevalence of IC, because, among women, there are more cases of asymptomatic PAD, or their symptoms of IC are more atypical, as demonstrated in this and other studies. 21,22
Our study investigated the differences between claudicant women and men specifically with intermittent claudication. This aspect has not been thoroughly studied until now: Most of the research into gender differences in this field has addressed PAD in general. Although cardiovascular risk factors are present in both sexes, the tobacco habit, as occurred in our series, is much less established in women of these age groups. 22 The other factors (and their analytic evaluation) arise in a similar way in men and women. 12,23 With respect to the presence of cardiovascular and associated osteoarticular diseases, this and another study 22 showed that women present a lower prevalence of ischemic cardiopathy and a greater prevalence of osteoarticular diseases.
An important difference of our study is that the claudicant women had lower scores for all four WIQ parameters (pain, distance, speed, and stair climbing), suggesting a lower capacity than men for deambulation, as other studies have also shown. 12,22,24 The ABI cannot explain these differences, since it is similar in women and men 22,23 ; at the same time, the correlation between ABI and WIQ is nonexistent 25 or weak 26 –28 for some, but never all, the parameters.
Finally, it is known that HRQL is lower in patients with PAD, specifically those in the IC phase. The few studies about HRQL and claudicant women reveal a worse quality of life with respect to many of the parameters measured in women by the Short Form Health Survey (SF-12) 12 and the World Health Organization Quality of Life (WHOQOL)-100. 29 Our study, which used the EQ-5D, also shows a greater reduction in the quality of life of women with IC compared with men with the condition. However, the HRQL is influenced by many factors (e.g., age, family status, comorbidity) other than those associated with the disease or situation that we may wish to measure (IC, in this case). Specifically, the women in our study present many of these potentially confounding factors, especially the presence of women with greater nondisabling osteoarticular comorbidity (since being nondisabling was an exclusion criterion). The multivariate linear regression reveals this and controls for the other factors mentioned.
Although the differences between the sexes with respect to IC have been explained by microcirculatory aspects, 30,31 we think that the greatest deterioration in the walk and quality of life of the women can be explained, at least partially, by the greater prevalence of osteoarticular comorbidities.
Our study has some limitations. Apart from the aforementioned low proportion (25%) of women in our sample, the study was also limited because it was not possible to carry out a treadmill test to objectively measure the IC. The use of ergometers is time consuming and costly and requires control by specialist professionals. However, this omission may not be too important, since clinical manifestations and the WIQ can be used as an alternative to treadmill testing for objectively assessing functional walking ability. Forty percent of recruited patients came from nonhospital consultations and justifies the use of the WIQ. Also, we do not have the information about possible difference in cardiovascular risk factor medications use between the sexes.
In summary, our study, which is one of the largest comparative case studies of claudicant women and men, highlights gender disparities in IC. The functional and quality-of- life IC consequences for women are the same as or worse than those for men.
Footnotes
Acknowledgments
We are grateful to the Saned Group for assistance with technical and statistical aspects of this study and to the Ferrer Group for funding the project through the SEACV Foundation.
The conception and design of our study were provided by Francisco S. Lozano, José R. March, Eduardo Carrasco, and José M. Lobos. Grupo Saned collected the data and conducted statistical analysis, along with Francisco S. Lozano, who also analyzed and interpreted the results. Francisco S. Lozano and José R. González-Porras wrote the text and created the tables and figure for this article; all the authors approved its final form.
Author Disclosure Statement
No competing financial interests exist.