
Abstract
Background:
Urinary tract infections (UTIs) are common bacterial diseases. We related diagnosis of UTIs based on International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and in-hospital mortality (IHM) in a cohort of hospitalized elderly subjects.
Methods:
All patients admitted between 2000 and 2013 to the general hospital of Ferrara, in northeast Italy, with ICD-9-CM code of UTIs were included. IHM was the main outcome, and age, sex, type of microorganism, sepsis, and Charlson comorbidity index (CCI) based on ICD-9-CM, were also analyzed.
Results:
The total sample included 2,266 patients (1,670 women, 73.7%) with UTIs and identification of a cultural organism. Mean age was 81.7±7.5 years (range, 65–103). One hundred and sixteen (5.1%, of whom 34.5% were male and 65.5% were female) cases developed sepsis, and 84 (3.7%, of whom 45.2% were male, 54.8% were female) had a fatal outcome. Nonsurvivors had lower prevalence of IVUs due to Escherichia coli (53.6 vs. 71.7%, p<0.001) and higher prevalence of UTIs due to Pseudomonas aeruginosa (19 vs 7.1%, p<0.001). Moreover, non-survivors developed more frequently sepsis (31% vs. 4.1%, p<0.001), and had higher CCI (2.81±2.43 vs. 2.21±2.04, p=0.011). IHM was independently associated, in decreasing order of odds ratios (ORs), with sepsis (OR 10.3; 95% confidence interval [95% CI] 6.113–17.460, p<0.001), P. aeruginosa infection (OR 2.541; 95% CI 1.422–4.543, p=0.002), female gender (OR 2.324; 95% CI 1.480–3.650, p<0.001), CCI (OR 1.103; 95% CI 1.005–1.210, p=0.038), age (OR 1.034; 95% CI 1.002–1.066, p=0.036), and E. coli infection (OR 0.5; 95% CI 0.320–0.780, p=0.002).
Conclusions:
In a large sample of elderly patients hospitalized for UTIs in a single center in northeastern Italy, apart the development of sepsis, IHM was much more dependent on pathogen and female gender than comorbidity index and age.
Introduction
I
The existence of a gender difference in in-hospital mortality (IHM) represents debated topic. Clinical outcomes in patients with hospital-acquired pneumonia admitted to ICUs are not different in the two sexes, 7 and recent data from the Surviving Sepsis Campaign showed that IHM did not differ by gender, although women were less likely to receive antibiotics within 3 hours. 8 Thus, the aim of this retrospective study was to relate diagnosis of UTIs based on International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes and in-hospital mortality (IHM) in a consecutive cohort of patients admitted to a hub university hospital of northeastern Italy, and to evaluate the odds of age, gender, type of cultural organism, and sepsis as life-threatening factors.
Subjects and Methods
Patient selection and eligibility
This study, conducted with the approval of the local institutional committees for human research, included all hospital hospitalizations with a discharge code of UTIs between January 1, 2000, and December 31, 2013, recorded in the database of the Azienda Ospedaliera-Universitaria of Ferrara St. Anna, Ferrara, Region Emilia-Romagna of Italy, and maintained by the Center for Health Statistics. Ferrara is a little town in the northeast of Italy, with a whole population of ∼351,101 inhabitants, 47,8% males and 52,2% females (update January 1, 2014) including its provincial territory, with Azienda Ospedaliera-Universitaria St. Anna (650 beds) as the sole hub hospital and site of the School of Medicine of the University of Ferrara (founded 1391). Since 1999, this hospital is provided with an electronic database and part of a regional network database to track all the discharge hospital sheets (DHSs) of patients admitted to all the regional hospitals. Each DHS lists the name, gender, date of birth, date, and department of hospital admission and discharge, vital status at discharge, length of stay, charge details, main and up to 15 accessory discharge diagnoses, and the most important diagnostic procedures, based on ICD-9-CM. In agreement with national dispositions by law in terms of privacy, the health authorities removed patient names, exact addresses, and other potential identifiers from the database provided for this study. A consecutive identification number for each patient was the only identification data allowed, in order to categorize the admissions by age group. We retrospectively analyzed patients in whom UTIs had been diagnosed, with determination of cultural organism. Thus, all patients in whom an ICD-9-CM code of UTIs were included, independently of site of infection, symptoms and department of admission, and systemic complications, such as sepsis, were also taken into account. The Charlson comorbidity index (CCI) 9 based on ICD-9-CM was also analyzed. The ICD-9-CM codes used to define UTIs were 112.2, 098.xx, 599.0 associated with 0.41.xx. IHM was our main outcome. The total number of hospital discharges maintained in the records in the considered period were 411,588 (47% males, 53% females).
Data collection
As the administrative regional database does not provide clinical information, we used IHM as a hard outcome indicator for UTIs, considering fatal cases (death during hospitalization) and nonfatal cases (patient discharged alive). Comorbidity was evaluated by means CCI modified for ICD-9-CM database, 10–11 and diagnoses of diabetes mellitus, heart failure, coronary heart disease, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, AIDS, liver disease, renal disease, dementia, and malignancy were considered as comorbidity components. Age, gender, type of cultured organism, sepsis, and CCI based on ICD-9-CM were analyzed.
Data analysis
The data are expressed as absolute numbers, percentages, and means±standard deviation. A descriptive analysis in patients with UTIs was performed. The analysis of the variables related to the diagnosis code was conducted using the chi-squared or Student's t-test or Mann-Whitney U test, as appropriate. Univariate analysis was carried out to determine the difference between survivors and deceased subjects. Moreover, in order to evaluate the independent parameters associated with IHM, IHM was considered as the dependent variable in a logistic regression analysis, with age, gender, type of cultured organism, sepsis and CCI based on ICD-9-CM being considered as independent ones. Odds ratios (ORs) and their respective 95% confidence intervals (95% CIs) were reported.
SPSS 13.0 for Windows (SPSS Inc., Chicago, IL) was used for statistical analysis.
Results
The total sample consisted of 2,266 patients (73.7% females), with a mean age of 81.7±7.5 years (range 65–103). Males accounted for 26.3% and females 73.7%; mean age was 80±7.3 for males and 82.3±7.5, respectively (p<0.001). Among male subgroup (n=596), prostate disease accounted for 13.1% (63 cases of benign prostatic hyperplasia, and 15 of adenoma, respectively). Sepsis developed in 116 (5.1% of whom 34.5% males, 65.5% females) cases developed sepsis, and fatal outcome occurred in 84 (3.7% of whom 45.2% males, 54.8% females). Causes of death included: infectious complications (n=22), respiratory and cardiovascular complications (n=16 and n=14, respectively), acute renal failure (n=9), neoplasms (n=7), cerebrovascular complications (n=5), and miscellaneous (n=11). Clinical characteristics of the entire population are reported in Table 1, and distribution of types of cultured organisms is shown in Fig. 1. More of 70% of UTIs were due to Escherichia coli. Comparison between survivors and deceased patients is reported in Table 2. Deceased patients had lower prevalence of UTIs due to E. coli (53.6 vs 71.7%, p<0.001) and higher prevalence of UTIs due to Pseudomonas aeruginosa (19 vs 7.1%, p<0.001) infections. Again, they were more likely to have sepsis (31% vs 4.1%, p<0.001) and had higher CCI (2.81±2.43 vs 2.21±2.04, p=0.011).
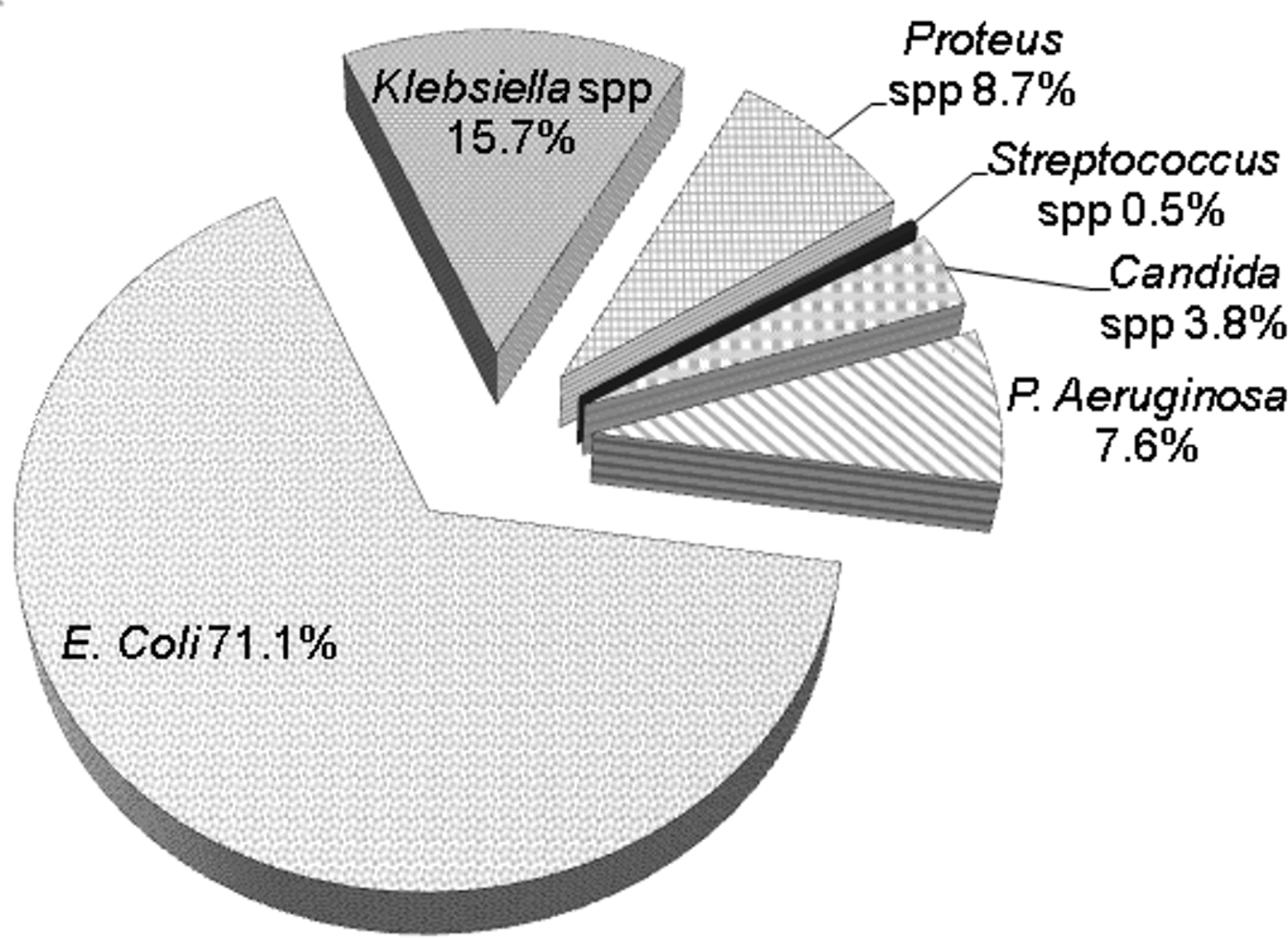
Distribution of the different cultured organisms in the total population of urinary tract infections (n=2,266).
SD, standard deviation; UTIs, urinary tract infections.
Logistic regression analysis showed that IHM was independently associated, in decreasing ORs order, with: sepsis (OR 10.3; 95% CI 6.113–17.460, p<0.001), P. aeruginosa infection (OR 2.541; 95% CI 1.422–4.543, p=0.002), female gender (OR 2.324; 95% CI 1.480–3.650, p<0.001), CCI (OR 1.103; 95% CI 1.005–1.210, p=0.038), age (OR 1.034; 95% CI 1.002–1.066, p=0.036), and E. coli infection (OR 0.5; 95% CI 0.320–0.780, p=0.002). Figure 2 shows the factors independently associated with IHM in the whole population and in subgroups by gender.
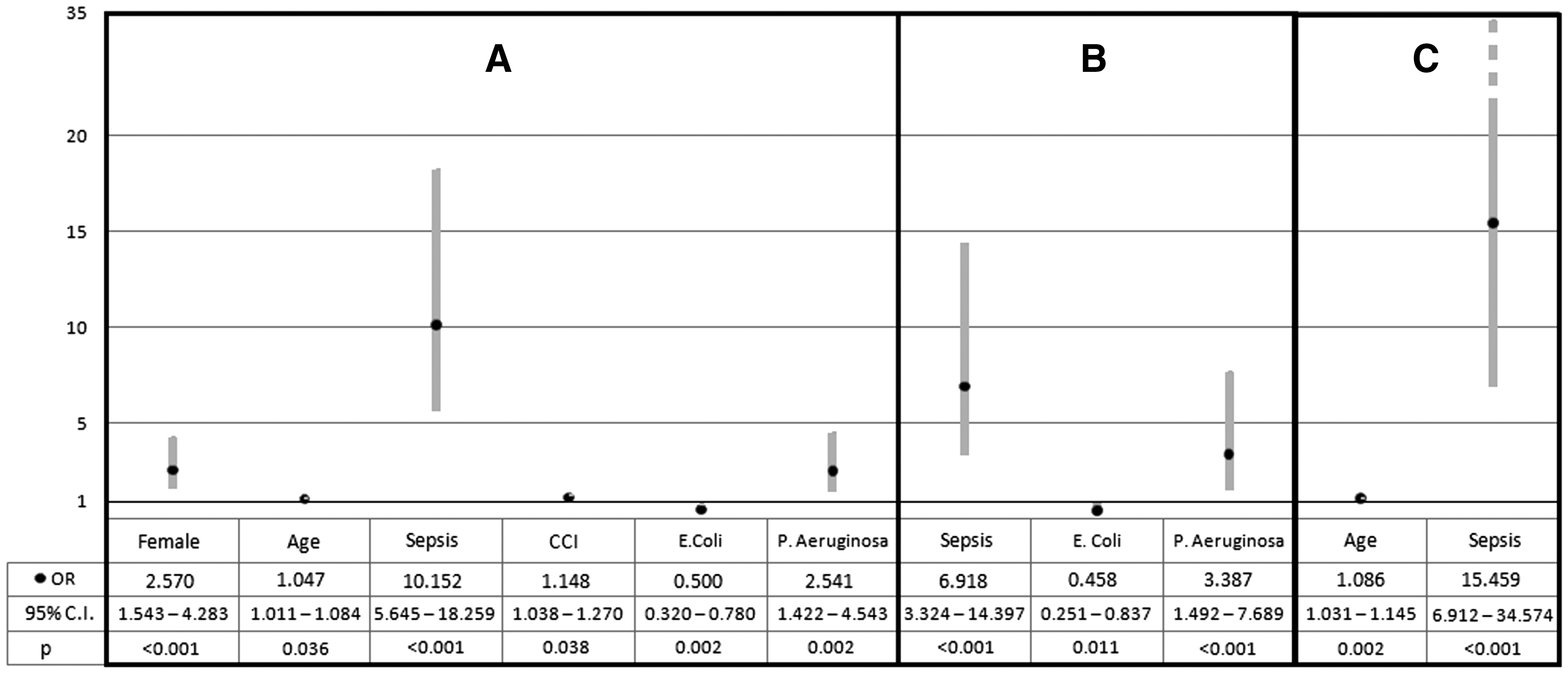
Factors independently associated with in-hospital mortalityin the whole population
Interestingly, when analyzing the population as a whole, female gender exhibited the same high OR as P. aeruginosa, and comorbidity was significantly associated with IHM. When the two subgroups by gender were analyzed separately, comorbidity disappeared from significant factor, whereas age remained significant only for males. The presence of sepsis always exhibited the highest OR (10.052, 95% CI 5.645–18.259, p<0.001), even if ORs were about 2.5-fold higher in males (15.459, 95% CI 6.912–34.574 vs. 3.387, 95% CI 3.324–14.397, respectively; p<0.001).
Discussion
As the population ages and life expectancy improves, infectious diseases represent a growing cause of morbidity, hospital admissions, and even mortality in older patients. 1 The present study, conducted in an area of Northeast Italy on a large series of consecutive admissions and representative of the geriatric population of our region and our country gives further confirmation that gender and comorbidities are risk factors for IHM in subjects with UTIs.
UTIs are a very common medical condition in the general population, particularly in elderly. Data from the U.S. National Center for Health Statistics reported that in 2010 UTIs were responsible for 4.7% of all general practitioner outpatient visits, 1.9% of visits in emergency departments, and 1.7% of hospital discharges diagnoses. 12 In the same year, costs for UTIs management were about $2.3 billion. 13
The incidence of bacteremia increases significantly with age, and a threefold increase in the incidence of bacteremia has been demonstrated in the 80 years and older group compared with the 60–79 years cohort. 14 On one hand, comorbidities surely play a pivotal role; on the other hand, elderly subjects present immunologic factors and physiological alterations, such as urinary and fecal incontinence, and the more frequent use of bladder catheters in repeated hospitalizations, all conditions that promote worse prognosis. 15 In a retrospective study on patients aged ≥65 years with bacteremia acquired outside the hospital setting, UTIs was the most common infection and was diagnosed in 46.7% of subjects. IHM was 22.2% in the whole population and 21.3% in subjects with UTIs 16 . In this study comorbidities were common, and independent predictors of IHM were age ≥85 years, chronic renal disease, bacteremia of unknown origin and cognitive impairment at admission. This study also reported that in elderly admitted in Internal Medicine wards the lack of identification of infection source was associated with a worse prognosis because of inadequate empirical therapy. 16
Virulence of the germs play an important role in the complex relationship between IHM and health care–associated UTIs. Pseudomonas and Candida are frequently isolated in the urine of subjects admitted in a health care setting, while in out-patients Enterococcus and Klebsiella were the bacteria more frequently isolated. 17 In agreement with our findings, UTIs are most frequently due to Gram-negative bacteria (especially E. coli), which also represent the causes of bacteremia development. On the other hand, only a limited percentage of UTIs were related to Candida spp; however, this kind of UTIs are usually due to the use of bladder catheters. 18 Unfortunately, due to study design, in our results we could not analyze how many infections could be classified as nosocomial or catheter-related. A favorable prognosis in UTIs could depend on the appropriate antibiotic treatment at an early stage and this is possible only if urine examination and urine culture are performed soon after the physician evaluation.
It has been reported that in patients with UTIs, IHM from any cause is between 10% and 20% and it appears to be independent from age, but it is related to comorbidities. 19 However, bacteremia and sepsis are more frequent in elderly than in young subjects, 20 and in the presence of sepsis, mortality rate goes up to 26%. 21 A bad prognosis in patients with UTIs is due to sepsis development. Mortality caused by septic shock may be determined by a systemic inflammatory response, independent of the inciting infection, but it may also be influenced by the anatomic source of infection. Although a recent collaborative study showed that obstructive uropathy-associated urinary tract infection was the source of infection with the lowest standardized hospital mortality (26%), 21 the risk of sepsis development is higher if a bladder catheter is inserted. 22 Bladder catheter–related infections represent the second cause of nosocomial infection, after pneumonia. 23 Moreover, it has been observed that infections related to bladder catheters are associated with a higher mortality at 7 days compared with patients with central venous vascular catheter, regardless of comorbidity and age of patients. 24
Interestingly, sepsis seems to exhibit different outcome depending on gender. On one hand, women are infected more frequently than men, and the risk of bacteremia increases after the age of 60 years. 25 However, such difference does not seems to be related only with age. In fact, a study on more than 133,000 adult discharges and 66,000 pediatric discharges in New York, NY, showed that odds of community-associated bloodstream infections, health care–associated bloodstream infections, and surgical site infections were significantly lower for women than for men after controlling for present-on-admission patient characteristics and events during the hospital stay. 26 Moreover, female sex is associated with improved organ function following traumatic injury and hemorrhagic shock, in particular in age groups that are at reproductive age. In fact, among patients admitted to the hospital for trauma and relevant bleeding, higher rates of multiple organ failure and sepsis were observed in males. 27 Experimental studies on animal models showed that, after an endotoxic shock secondary to single injection of lipopolysaccharide (LPS), there were unremarkable differences between male and female rats. However, female rats may recover the inotropic cardiac function earlier than males. 28 In particular, the protection of female hearts against the dysfunction associated with sepsis is (at least in part) attributable to cardiac activation of the protein kinase B/endothelial nitric oxide synthase (Akt/eNOS) survival pathway, decreased activation of nuclear factor κB (NF-κB), and decreased expression of inducible nitric oxide synthase (iNOS), tumor necrosis factor-α (TNF-α), and interleukin-6. 29 Again, it has been reported that male neutrophils show higher responsiveness to stimulation with LPS and interferon-gamma (IFN-γ) than female neutrophils, suggesting that the gender difference in neutrophil responsiveness to LPS and IFN-γ may be partly responsible for that in the outcome of sepsis, in which premenopausal women show a favorable prognosis as compared with men. 30 During sepsis, a complex network of cytokine, immune, and endothelial cell interactions occur and disturbances in the microcirculation cause organ dysfunction or even failure leading to high mortality in those patients. Female gender has been demonstrated to be protective under such conditions, whereas male gender may be deleterious due to a diminished cell-mediated immune response and cardiovascular functions. Male sex hormones (i.e., androgens) have been shown to be suppressive on cell-mediated immune responses. In contrast, female sex hormones exhibit protective effects, which may contribute to the natural advantages of females under septic conditions. 31
The present study has several limitations. This is a single-center, cross-sectional, retrospective study based on ICD-9-CM codes that are known to have poor sensitivity. In fact, diagnosis could be biased by hospital codifying procedures and individual skills. However, the final data are in agreement with what is already known in literature, therefore giving support to our results. Second, evaluating IHM only, information on out-of-hospital mortality is lacking. Third, data based on ICD9-CM codes do not provide information on severity of illness or intensity of care, including aggressive therapies and use of devices. Although we used a validated comorbidity index, it is possible that unmeasured severe and/or mild diseases could had impacted the prognosis. Nevertheless, even with these limitations, this study, based on evident clinical diagnosis and considering a large population, may be considered as representative of the real world of everyday clinical practice. Moreover, we could not differentiate uncomplicated form complicated UTIs, including subjects who underwent catheterization. 5 On the other hand, we can speculate that uncomplicated UTIs should not be hospitalized; therefore, the great majority of subjects included in this study had complicating factors, such as hospital-acquired infections, recent antimicrobial use, resistant uropathogens, indwelling catheter, urological procedures, immunosuppressing conditions, and comorbidities. 5 Moreover, we could not diagnose recurrent UTI; in fact, we could not establish if UTI was caused by reinfection with previously isolated organism. 32
Conclusions
In patients admitted in a hospital of Northeastern area of Italy, a higher IHM was mainly related to female gender, comorbidities (expressed by CCI), and age, even if total mortality was remarkably lower compared with that reported in literature. In particular, logistic regression analysis showed that IHM was independently associated with female gender (OR 2.32). In a recent study on a large cohort of more than 3,900 ICU patients (36.5% females) in the northwestern area of Italy (Region of Piedmont), ICU mortality was similar in men and women in the whole cohort, but female gender was independently associated with a higher risk of ICU death in patients with severe sepsis (OR 2.33). 33 These results, apparently contradictory to the literature findings of a better response of female gender to sepsis, could be explained by the older age of patients enrolled in the Italian studies (66±16 years in Piedmont, northwest Italy, 81.7±7.5 years in Emilia-Romagna, northeast Italy), largely beyond the protective effect observed in the premenopausal age. Moreover, this significantly higher age implies the presence of important comorbidities, and it is known that the CCI has a great importance as a predictive factor for mortality. 1 The possibility to identify predictors of negative outcome in elderly patients with UTIs could help physicians in the clinical decision making process, especially in a period of paucity of resources.
Footnotes
Acknowledgments
The authors thank Dr. Nicola Napoli and Dr. Franco Guerzoni, Centre for Health Statistics, Azienda Ospedaliera-Universitaria of Ferrara, Italy, for their precious support and valuable collaboration. This study has been supported, in part, by a scientific grant from the University of Ferrara (Fondo Ateneo Ricerca).
Author Disclosure Statement
No competing financial interests exist, and there are no potential conflicts of interest by sponsoring agents, products, technology, or methodologies used in this report submitted for publication by any of the authors.