
Abstract
Background:
Results from a number of long-term follow-up studies have suggested that hypertensive disorders in pregnancy are associated with increased risk of cardiovascular disease later in life. More recently, this putative relationship has been substantiated with findings of elevated cardiovascular risk factors, such as lipid profiles and glucose, in women with a history of hypertensive pregnancy disorders. Homocysteine is a sensitive indicator of increased risk but data on homocysteine levels in women with a history of hypertensive pregnancy disorders are inconsistent.
Design:
This cohort study included 279 women with a history of hypertensive pregnancy disorders at term and 85 women with a history of uncomplicated pregnancies who participated in the Hypitat Risk Assessment Study (HyRAS).
Methods:
Blood samples for total homocysteine determination were taken 2.5 years postpartum. Homocysteine levels were determined in plasma using an immunoassay.
Results:
Women with a history of hypertensive pregnancy disorders had significant higher median homocysteine levels (10.66 μmol/L) 2.5 years postpartum compared with women with a history uncomplicated pregnancies (9.82 μmol/L; p=0.002). Women with a history of hypertensive pregnancy disorders had a higher risk of having a homocysteine level in the highest quartile (odds ratio 3.4, 95% confidence interval 1.5–7.6).
Conclusion:
At 2.5 years postpartum, women with a history hypertensive pregnancy disorders had higher homocysteine levels than women who had uncomplicated pregnancies. Although higher homocysteine levels might be a potential link between a history of hypertensive pregnancy disorders and increased cardiovascular disease risk later in life, the clinical implications remain an area for future research.
Introduction
C
This implies that pregnancy may unmask patients with a phenotype of elevated risk factors underlying defects, thus identifying women at increased risk for cardiovascular events at a relatively young age. 6 Screening and tailored interventions might help to change lifestyle and promote healthy ageing of the women at risk. Ideally, interventions should be based on understanding the shared pathophysiology of both hypertensive pregnancy disorders and cardiovascular disease later in life. Currently the pathophysiology of both hypertensive pregnancy disorders and cardiovascular disease and the link between these two disorders is investigated. 7 The most common hypothesis is that in both disorders there is an underlying endothelial dysfunction, manifesting in pregnancy by changes in spiral arteries and later in life in cardiovascular disease as atherosclerosis. 8,9
Studies on cardiovascular risk factors after hypertensive pregnancy disorders mainly focused on classic biomarkers, like lipid profiles, blood pressure, and glucose metabolism. 10,11 Elevated classic biomarkers are described in both women with a history of early and late hypertensive pregnancy disorders compared to women with a history of uncomplicated pregnancies. 12,13
Several biomarkers in women with cardiovascular disease have been associated with atherosclerosis, including biomarkers on inflammation, dyslipidemia, and homocysteine. 14,15 Higher homocysteine levels are associated with coronary heart disease and stroke. 16 Homocysteine is an amino acid that acts as biomarker for oxidative stress and enhanced endothelium inflammation and is suggested to be a more specific and sensitive marker of endothelium dysfunction than classic markers for cardiovascular disease. Increased homocysteine levels are described in association with obstetric complications including preeclampsia, 17 recurrent loss of early pregnancy, 18 and small-for-gestational-age offspring. 19 Homocysteine levels in women with a history of hypertensive pregnancy disorders have been investigated before, as will be noted later, but our large study design with a relative short follow-up time is unique.
In this study we examined whether homocysteine, an early marker for increased cardiovascular risk, is elevated after hypertensive pregnancy disorders.
Methods
Participants
Participants for this cohort study have been selected from the Hypertension and Preeclampsia Intervention Trial at Term (HYPITAT) trial. 20 Between October 2005 and March 2008 the HYPITAT study (trial registration: ISRCTN08132825) was conducted nationwide in The Netherlands. This was a multicenter, parallel, open-label randomized, controlled trial of induction of labor versus expectant management in women with pregnancy induced hypertension or preeclampsia at term. The HYPITAT study included women with gestational hypertension, with a singleton pregnancy and a fetus in cephalic presentation at a gestational age between 36+0 and 41+0 weeks. These patients with a history of hypertensive pregnancy disorder were invited for our follow up study, the Hypitat Risk Assessment Study (HyRAS). 21
Between June 2008 and November 2010, women who participated in this follow-up study were assessed for cardiovascular risk factors at least 2 years after index pregnancy. Results of the cardiovascular risks of these participants with a history of hypertensive pregnancy disorders were compared to the cardiovascular risk of a group of women with uncomplicated pregnancies. The cohort of women with an uncomplicated pregnancy was selected from either friends of HYPITAT participants or women from midwifery practices with a history of only uncomplicated normotensive pregnancies. At time of the postpartum cardiovascular risk assessment, women were excluded when they were pregnant or lactating. A description of the inclusion and exclusion criteria of the study participants and the results of the study are described and published elsewhere (HyRAS study). 20,21
In summary, for the HyRAS follow-up study cardiovascular risk factor assessment was conducted by blood pressure measurement, weight, height, and hip and waist circumference. Furthermore, all participants were asked to complete a questionnaire. This questionnaire included, among other topics, current use of medication including folic acid, obstetric history, and smoking. Venous blood samples were collected after an overnight fast and assayed for glucose, glycated hemoglobin (HbA1c), insulin, total cholesterol, high-density lipoprotein cholesterol, triglycerides, and high-sensitivity C-reactive protein (HsCRP). Insulin resistance was assessed by the homeostasis model assessment. 21 Homocysteine was determined from the venous blood sample.
Laboratory methods
For analysis of homocysteinelevels, ethylenediaminetetraacetic acid venous blood samples were drawn after an overnight fast. After centrifuging the blood samples for 9 minutes at 1440 g at the local center, all samples were sent to the same laboratory (VU Medical Centre Amsterdam, Amsterdam, The Netherlands). They were kept at −60°C until analyses were done. Maximum length of storage before analysis was 2 years. Homocysteine levels were measured using an immunoassay (Architect, Abbott Diagnostics, Abbott Park, IL). The lower limit of quantitation of this assay is 1 μmol/L, the intra-assay coefficient of variation (CV)<3%, and the inter-assay CV<5% for the whole concentration range.
For analysis of the other cardiovascular markers used in the Framingham risk score, venous blood samples were drawn. A detailed description of determination of these markers was previously published elsewhere. 22 After centrifuging the blood samples for 9 minutes at 1440 g at the local center, all samples were sent to the same laboratory (Medical Centre Haaglanden, the Hague, the Netherlands) and analyzed within 24 hours. Plasma was prepared and stored at −70°C in 1.5-mL volumes until used.
Homocysteine levels were measured in a fasting state since the intake of a large, protein-rich meal may increase the plasma homocysteine concentration. A review containing recommendations on homocysteine determination stated extensive clinical applicable guidelines and included a statement on case control series for homocysteine. 23 Advice is that controls should optimally be recruited from the same general population as the cases. For clinical convenience we chose not to determine genetic data and blood determinants on cobalamin and creatinine. Since the questionnaire included a question on folic acid supplementation, we were quite sure of which women were using this kind of supplementation, and therefore, these women were excluded from analysis. In the questionnaire, we further assessed medication use, but we did not specific asked for vitamin supplement usage. Therefore, we chose not to exclude women using vitamin supplements.
Definitions
Participants in this study had a history of hypertensive pregnancy disorder, defined as gestational hypertension or preeclampsia by criteria of the International Society for the Study of Hypertension in Pregnancy, ISSHP. 24 Gestational hypertension was defined as diastolic blood pressure equal to or above 95 mmHg measured on two occasions at least 6 hours apart in a woman who was normotensive at the start of pregnancy until week 20 of gestational age. Preeclampsia was defined as diastolic blood pressure equal to or above 90 mmHg measured on two occasions at least 6 hours apart, combined with proteinuria. Proteinuria was defined as ≥2+protein on dipstick, >300 mg total protein in a 24-hour urine collection and/or protein to creatinine ratio>30 mg/mmol.
Normal range for homocysteine levels contains values between 5 and 15 μmol/L. Hyperhomocysteinemia is defined as homocysteine levels above 15 μmol/L, divided in moderate (≥15 μmol/L), intermediate (>30 micormol/L) and severe (>100μmol/L) hyperhomocysteinemia. 25
Data analysis
Characteristics were described for women with a history of hypertensive pregnancy disorders and women with a history of uncomplicated pregnancies at 2.5 years postpartum. Differences in characteristics were calculated using SPSS software (version 18.0). The one-way analysis of variance test was used when the data was numerical and the chi-squared test when categorical data were analyzed. Categorical data were displayed in number of appearance and percentage of the total. Numerical values were displayed in mean value, 95% confidence interval (CI), and p-value.
In the view of the skewed distribution, a Mann-Withney U test was used to compare interval to delivery and homocysteine levels in women with a history of hypertensive pregnancy disorders and women with a history of uncomplicated pregnancies. To assess the association of homocysteine levels with the history of hypertensive pregnancy disorders, we calculated odds ratios for women with a history of hypertensive disorders for quartiles of homocysteine. Quartiles were determined by distribution of homocysteine concentrations among women from this study group. We calculated adjusted odds ratios using multivariate logistic regression.
Subsequently we wanted to perform a subgroup analysis on the group normotensive women before pregnancy by excluding women who were possibly suffering from chronic hypertension. A subgroup analysis was therefore performed in women with a booking blood pressure (first measured blood pressure in pregnancy) of <120/70 mmHg.
Results
Of 306 women with a history of hypertensive pregnancy disorders and 99 women with a history of uncomplicated pregnancy, we included 289 women with a history of hypertensive pregnancy disorders and 85 women with a history of uncomplicated pregnancy. In total, 22 women were excluded from analysis: 11 women with a history of hypertensive pregnancy disorders and 11 women with a history of uncomplicated pregnancy, due to insufficient blood samples for determination of homocysteine. Nine women were using folic acid supplementation at the time blood was sampled. These women—6 with a history of hypertensive pregnancy disorders and 3 with a history of uncomplicated pregnancy—were excluded from further analyses. Vitamin supplements including vitamin B6 and B12 could influence homocysteine levels, but since the effects are less significant than the effect of folic acid, we chose not to exclude women who used vitamin supplements.
Characteristics at 2.5 years postpartum
Characteristics of women with a history of hypertensive pregnancy disorders and women with a history of uncomplicated pregnancies 2.5 years postpartum are stated in Table 1. There were no differences in age, smoking rate, ethnicity, and interval between delivery and blood drawn for determination of homocysteine between women with a history of hypertensive pregnancy disorders and women with a history of uncomplicated pregnancies. Women with a history of hypertensive pregnancy disorders were more often nulliparous and had higher body mass index (BMI) and systolic and diastolic blood pressure 2.5 years postpartum.
BMI, body mass index; PE, preeclampsia; PIH, pregnancy-induced hypertension; SD standard deviation.
Homocysteine
Women with a history of hypertensive pregnancy disorder had a significantly higher median homocysteine concentration 2.5 years postpartum compared with women who had a history of uncomplicated pregnancy (respectively 10.7μmol/L; 9.82 μmol/L; p<0.01) (Table 1).
Homocysteine levels were divided into four quartiles based on homocysteine levels of the current study group. This highest quartile consisted of homocysteine level over 12.6 μmol/L. The odds ratio for women with a history of hypertensive pregnancy disorders for homocysteine levels within the highest quartile compared with the lowest quartile was 3.2 (95% CI 1.5–6.5). Adjusted for age, BMI, parity, and smoking, this odds ratio was 3.4 (95% CI 1.5–7.6). A trend of increased odds ratios was seen in the higher quartiles of homocysteine levels for women with a history of hypertensive pregnancy disorders (Fig. 1).
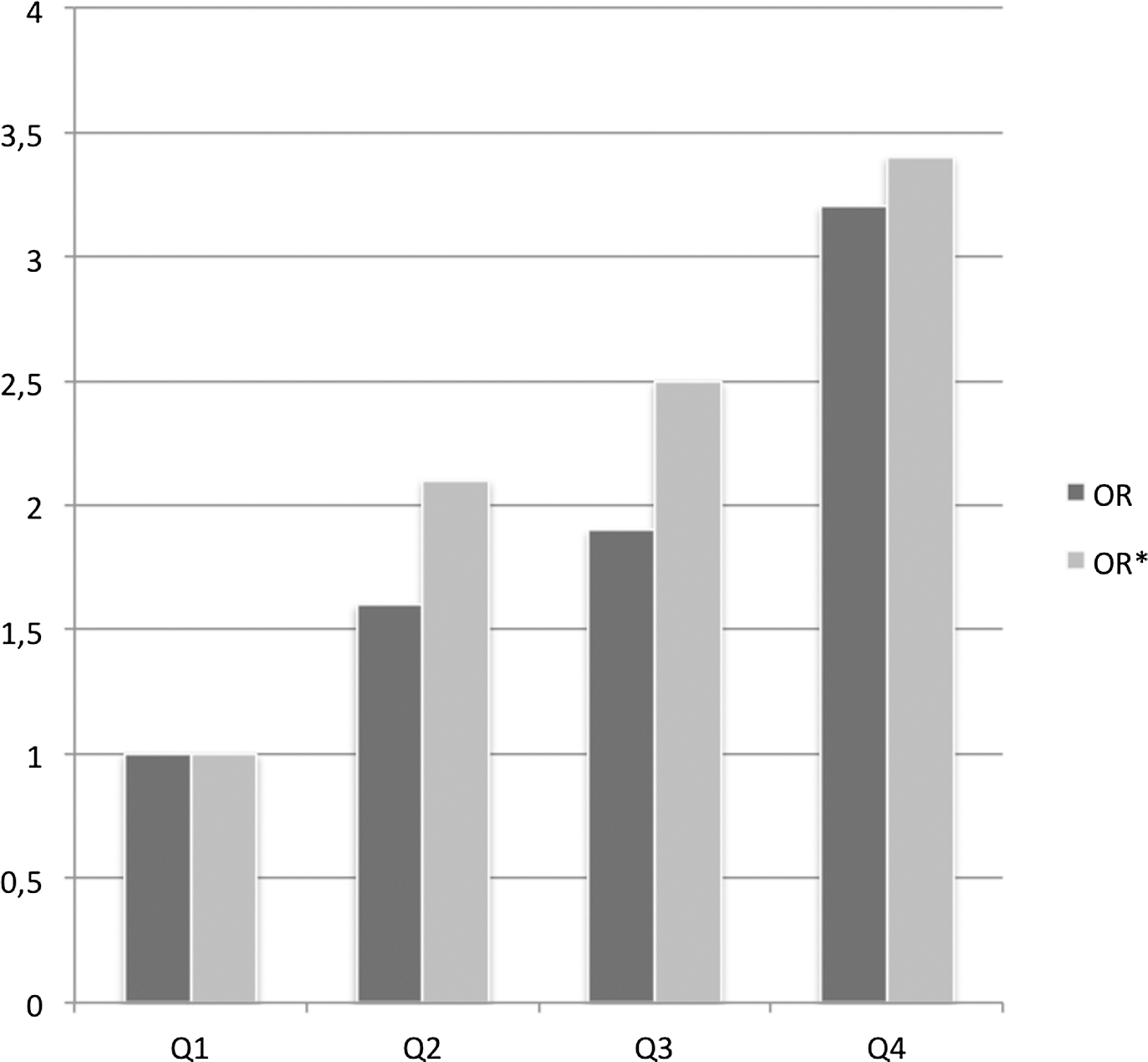
Odds ratio (OR) quartiles for homocysteine concentration 2.5 years postpartum. OR*, odds ratio adjusted for age, BMI, parity, and smoking.
Subgroup analysis
In a subgroup analyses we aimed to analyze only normotensive women. Women with an increased blood pressure before pregnancy might experience chronic hypertension, which is not diagnosed. Therefore, we performed subgroup analyses for women with a blood pressure at the start of the pregnancy <120/70 mmHg (n=81). 25 In this subgroup, the median homocysteine levels did not significantly differ between women with a subsequent hypertensive pregnancy disorder compared with women without subsequent hypertensive pregnancy disorder (respectively 9.44 μmol/L, 9.75 μmol/L; p=0.78). For women in this subgroup analysis, there was no difference of homocysteine levels in higher quartiles for women with a history of hypertensive pregnancy disorders compared with women with a history of uncomplicated pregnancies.
Gestational hypertension and preeclampsia
Of the women with a history of gestational hypertension, the median homocysteine level was 10.8 μmol/L (min 4.53, max 27.0). Of the women with a history of preeclampsia, the mean homocysteine level was 10.2 μmol/L (min 5.71, max 42.9) (Table 1).
A significant difference in homocysteine level was found between women with a history of gestational hypertension and women with a history of normotensive pregnancy (p=0.04).
A significant difference in homocysteine level was also found between women with a history of preeclampsia and women with a history of normotensive pregnancy (p<0.01).
Discussion
The results of this follow-up study among women with and without hypertensive pregnancy disorders show that women with a history of hypertensive pregnancy disorders have significantly higher fasting homocysteine levels 2.5 years postpartum.
Strengths and limitations
To appreciate these findings, some aspects of the study need to be addressed. A strength of this study is that we included a large study group in a longitudinal, prospective follow-up setting. Although we included a large cohort, the group women with a history of hypertensive pregnancy disorders is bigger than the group women with a history of uncomplicated pregnancy. Homocysteine determination was performed 2.5 years postpartum. We used this time period because hypertension can take up to 2 years to resolve after a pregnancy complicated by hypertensive disorders. 26,27 We found no significant difference in median interval from delivery to venipuncture for determination of homocysteine for cases and controls, but we found a wide time range in our study group. We investigated the homocysteine levels by increasing time interval and found no linear relation between these; no defined increase or decrease of homocysteine levels were found in women with an increasing time interval between delivery and homocysteine determination.
Also, women who used folic acid supplementation at the time of the blood draw were excluded, since we know this influences the measured homocysteine levels. However, folic acid supplementation use was evaluated by a questionnaire and could therefore be incomplete.
Steegers-Theunissen et al. 28 reported that homocysteine were higher in women with a history of hypertensive pregnancy disorders, although this relationship disappears after adjustment for time. In our study, follow-up time did not significantly differ between women with a history of hypertensive pregnancy disorders compared with women with a history of uncomplicated pregnancy. Third, we did not evaluate vitamin status and genetic variants, which may influence homocysteine levels, which could bias results in this study. 28,29
Literature search
To gain insight into the literature on this subject, we performed a literature search. The search was performed in PubMed from inception to February 2015, using the following search terms with their synonyms: gestational hypertension, preeclampsia, eclampsia, homocysteine. One of the studies was a systematic review conducted by our study group in 2013 on nonclassic cardiovascular biomarkers after hypertensive pregnancy disorders. 30 The extensive search conducted for the systematic review included five studies 31 –35 on homocysteine levels after hypertensive pregnancy disorders in a meta-analysis that showed a higher mean homocysteine level in women with a history of hypertensive pregnancy disorders compared with women with a history of uncomplicated pregnancy. Besides the five studies included in the meta-analysis, we found five studies on homocysteine levels after hypertensive pregnancy disorders. 36 –40 The cases in these studies differ significantly: studies included women with preeclampsia, women with preeclampsia and pregnancy-induced hypertension, or both. Further, studies included women with preeclampsia at term or preterm pregnancy or included women with severe preeclampsia. Follow-up time, the time from pregnancy complicated by hypertensive pregnancy disorders till the time of homocysteine determination, was different in all of these studies. One study described homocysteine levels in the first days postpartum, 36 where the study by White et al. described homocysteine levels in women at the age of 60 years. 38 Since studies were so diverse, we felt that the current study on homocysteine levels at 2.5 years postpartum after hypertensive pregnancy disorders could provide new information. We included cases with hypertensive pregnancy disorders at term because these disorders have a high incidence. Further, the follow-up time in our study was 2.5 years; we expected the influence of pregnancy on homocysteine levels to be reduced at this time postpartum. On the other hand, at this time postpartum there is still a wide time frame for possible preventive interventions for cardiovascular disease in case of elevated homocysteine levels displaying a higher cardiovascular risk.
Clinical implications
Since most women undergo their first blood pressure measurement at the booking visit of their first pregnancy, it is difficult to elucidate whether the association of hypertensive disorders in pregnancy and future cardiovascular disease can be partly explained by chronic hypertension before pregnancy. Surprisingly, we found in the subanalyses that homocysteine levels are not significantly higher 2.5 years postpartum in women with a history of hypertensive pregnancy disorders with a booking blood pressure >120/70 mmHg. This might suggest an association of (unknown) chronic hypertension before pregnancy with higher levels of homocysteine both complicated by hypertensive pregnancy disorders and CVD later in life. 41
It is generally accepted that early detection of higher cardiovascular disease risk factors could lead to reduction of cardiovascular disease by preventive measurements like lifestyle changes or use of medications. 42,43 Homocysteine could be of additive value in identifying women with a higher risk because higher homocysteine levels are an early sign of endothelial damage, present before clinical signs of cardiovascular disease are revealed. 44 Up to now there is no convincing evidence that therapy lowering homocysteine levels decreases the risk of cardiovascular disease. 45,46 Since no research was performed in the specific group of women with a history of hypertensive pregnancy disorders, the clinical implications of results in this study remain an area for future research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.