
Abstract
Background:
Hormone therapy (HT) is associated with increased risk of both venous and arterial thrombosis, which are multifactorial in origin.
Objectives:
Our objectives were twofold: first, we sought to examine associations between endogenous serum sex hormone levels and biomarkers of thrombosis and/or coagulation in postmenopausal hormone nonusers. Second, we separately studied the associations between serum sex hormone levels and biomarkers of thrombosis and/or coagulation in postmenopausal hormone users considering the fact that pattern of circulating hormones is different in women taking exogenous hormones.
Patients/Methods:
We performed a cross-sectional analysis of postmenopausal women enrolled in a large multiethnic community-based cohort study, The Multiethnic Study of Atherosclerosis. We hypothesized that higher levels of estrogen-related sex hormones would be associated with biomarkers of thrombosis, suggesting mechanisms for differences in thrombotic risk from HT. Women (n = 2878) were included if they were postmenopausal and had thrombotic biomarkers (homocysteine, fibrinogen, C-reactive protein [CRP], factor VIII, and
Results and Conclusions:
We found that elevated levels of estradiol and SHBG in HT users were associated with elevated levels of CRP and lower levels of TFPI, both of which may be related to a prothrombotic milieu in HT users. HT nonusers had far more prothrombotic associations between elevated serum sex hormone levels and thrombotic biomarkers when compared with HT users.
Introduction
H
Large-scale observational studies demonstrated significant reduction in cardiovascular risk in postmenopausal women taking HT. 5 However, randomized clinical trials failed to show a benefit either in secondary or primary prevention of coronary events. In fact, there is evidence of an increase in cardiovascular events in the first several years of therapy. 6,7 In particular, HT is associated with an increased risk of venous thromboembolism, stroke, and myocardial infarction. 6,8 The seemingly opposite expected results between the observational studies and randomized clinical trials have led to several secondary and ancillary analyses to further explore potential mechanisms of increased risk of HT. 9,10
Potential mechanisms of prothrombosis include a prothrombotic state, reduced fibrinolysis, and activation of inflammation. 11 –15 To address potential mechanisms of hemostasis imbalance, we examined associations between serum sex hormone levels and thrombotic biomarkers based on whether postmenopausal women were using HT or not in a large multiethnic community-based group of women. We hypothesized that higher estradiol and sex hormone-binding globulin (SHBG) levels and lower testosterone levels in HT users may be associated with biomarkers of thrombosis and this association may identify women at increased thrombotic risk from HT.
Patients/Methods
Study population
The Multiethnic Study of Atherosclerosis (MESA) is a longitudinal cohort study of subclinical cardiovascular disease and its progression in an ethnically diverse population-based sample of 6814 men and women aged 45–84 years. 16 This cohort is free of known cardiovascular disease at baseline. Approximately 38% of the recruited participants are white, 28% African American, 22% Hispanic, and 12% Asian of Chinese descent. In 2000–2002, participants were recruited from six field centers across the United States: Baltimore City/Baltimore County, MD; Chicago, IL; Forsyth County, NC; Los Angeles County, CA; Northern Manhattan/the Bronx, NY; and St. Paul, MN. Details on the examination procedures have been published elsewhere. 16 Each participant provided written informed consent. The study was conducted in accordance with institutional guidelines and with Institutional Review Board approval.
We used the MESA baseline cross-sectional data and data from an MESA ancillary study that measured circulating sex hormone levels at baseline to examine the association of exogenous hormone therapy, serum sex hormone levels, and thrombotic factors in women. From the full cohort of 3601 women, we included women who were postmenopausal, had complete data on HT use at baseline, and had thrombotic biomarkers (homocysteine, fibrinogen, C-reactive protein [CRP], factor VIII, and
Baseline data included gender, age, race/ethnicity, smoking, medication use, body–mass index (BMI, kg/m2), and resting blood pressure. Fasting cholesterol and glucose levels were measured at the Collaborative Studies Clinical Laboratory at Fairview University Medical Center (Minneapolis, MN). Total and HDL cholesterol were measured using cholesterol oxidase methods. Low-density lipoprotein cholesterol was calculated using the Friedewald equation when triglyceride <400 mg/dL. Hypertension was defined as receiving antihypertensive medications or a blood pressure ≥140 mmHg systolic or ≥90 mmHg diastolic. Diabetes was defined as receiving hypoglycemic medication or a fasting blood glucose of ≥126 mg/dL. Smoking status was categorized as never, former, or current. HT use was self-reported by participants and confirmed by medication review and categorized as never, former, or current use of estrogens and/or progestins, excluding vaginal creams. Questionnaires for hysterectomy and oophorectomy were used to determine whether a woman had had surgical menopause, these were included as postmenopausal. Information about the indication for HT was not available. Information about oral versus transdermal formulation or the exact hormonal preparation was also not available. For purposes of our analysis, we analyzed women who were either currently on HT or not currently on HT. The inclusion criteria for our analysis were affirmative response on menopause, “don't know” was an exclusion; if menopause was not answered and the age was greater than or equal to 55 years, the participant was also considered postmenopausal. Women with hysterectomy (and either missing data or no oophorectomy) were included as postmenopausal if they were 55 years or older.
Serum sex hormones measured were total testosterone (T), bioavailable testosterone, SHBG, estradiol (E2), and dehydroepiandrosterone (DHEA). Fasting blood samples were drawn between 7:30 a.m. and 10:30 a.m. and within 24 hours of hormone intake. Serum was stored at −70°C, then shipped on dry ice for freezer storage to the University of Vermont Central Blood Analysis Laboratory. Details of serum sex hormone measurement have been published elsewhere.
17
Plasma thrombotic markers included CRP, homocysteine, fibrinogen, factor VIII, vWF, PAI-1, TFPI, and
Higher CRP, homocysteine, fibrinogen, factor VIII, vWF, PAI-1, and
Statistical analysis
We tabulated demographic and cardiovascular risk factor characteristics by category of current use of HT. Differences between groups were tested using t-tests for continuous variables and χ2 tests for categorical variables. Biomarker and sex hormone levels were skewed for both groups; hence, they were logarithmically transformed before they were included in regression analyses. We analyzed the association of logarithmically transformed thrombotic biomarkers as the dependent variable with logarithmically transformed sex hormone levels as the independent variables using linear regression, adjusting for age, race, BMI, current smoking, hypertension, and diabetes. Biomarker and sex hormone variables were entered in the regression models in units of standard deviation so that the magnitudes of the regression coefficients for various models could be compared. Analyses were stratified by current use of hormone replacement therapy. We used the Bonferroni correction for examining 80 p-values to test hypotheses: a p-value of <0.00625 (i.e., 0.05/80) was considered statistically significant.
We performed additional analysis, which is presented in the online Supplementary Data (Supplementary Data are available online at
Results
Characteristics of women by HT use status are shown in Table 1. Women taking HT were younger than women not taking HT. A larger proportion of HT users than nonusers were more likely Caucasian than African American, Chinese American, or Hispanic. Women on HT were less likely to have diabetes than nonusers, had lower systolic and diastolic pressures, and lower BMI. The type of HT use among users was combined estrogen and progestin in 37%, estrogen only in 53%, and unknown in 10% HT users.
Mean ± SD shown unless otherwise indicated.
Median [25th–75th percentile], tested using rank sum test.
BMI, body–mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; HT, hormone therapy; SBP, systolic blood pressure.
Women on HT had lower total testosterone, bioavailable testosterone, and DHEA levels and higher estradiol and SHBG (Supplementary Table S1) consistent with prior studies.
19,20
Women currently using HT had lower adjusted mean levels of homocysteine, fibrinogen, PAI-1, TFPI, and
Figure 1 shows the association of serum sex hormone levels with thrombotic biomarkers in the women who were HT nonusers expressed as standardized beta with 95% confidence interval after adjustment for age, BMI, race, hypertension, smoking, and diabetes. Higher bioavailable testosterone levels were associated with significantly higher CRP [0.099 (0.059 to 0.1390] and fibrinogen [0.072 (0.028 to 0.116)] levels, but with lower homocysteine levels [−0.072 (−0.166 to −0.028)]. Higher estradiol levels were associated with significantly higher CRP levels [0.069 (0.028 to 0.110)]. Higher DHEA levels were associated with significantly higher CRP [0.096 (0.056 to 0.136)] and fibrinogen levels [0.088 (0.044 to 0.132)]. Finally, higher SHBG levels were associated with significantly lower CRP [−0.215 (−0.257 to −0.173)] and PAI-1 levels [−0.204 (−0.325 to −0.084)] along with higher
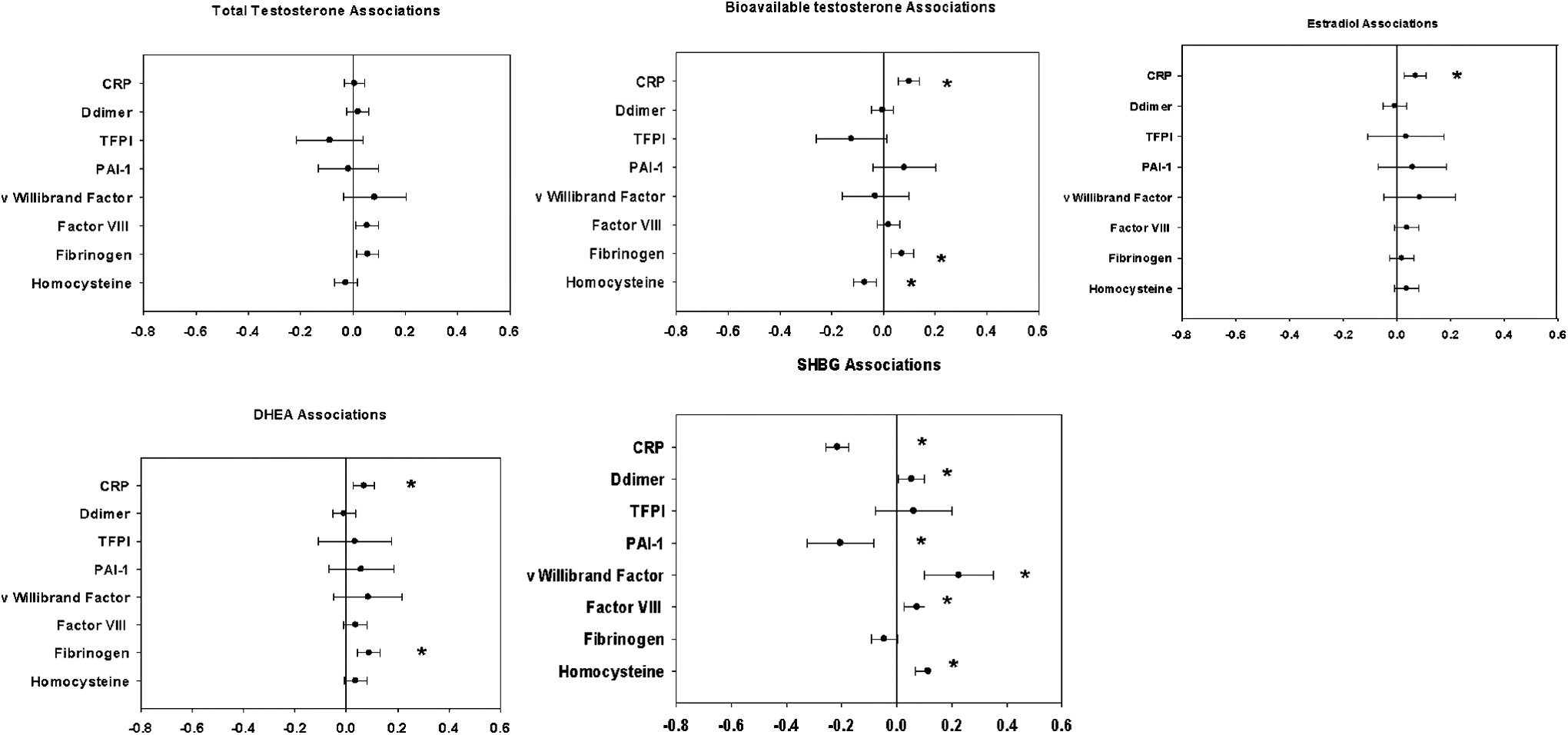
Associations of sex hormone levels with thrombosis biomarkers. Among nonusers of hormone therapy, the plot shows the difference in the biomarker level (represented as the increment of its SD) for each SD higher serum sex hormone level after adjustment for age, BMI, race, hypertension, smoking, and diabetes. BMI, body–mass index; CRP, C-reactive protein; TFPI, tissue factor pathway inhibitor-1; PAI-1, plasminogen activator inhibitor-1; DHEA, dehydroepiandrosterone; SHBG, sex hormone-binding globulin. *p ≤ 0.00625.
Figure 2 shows the association of serum sex hormone levels with thrombotic biomarkers in the women who were HT users expressed as standardized beta with 95% confidence interval after adjustment for age, BMI, race, hypertension, smoking, and diabetes. Higher bioavailable testosterone levels were associated with significantly higher TFPI levels [0.231 (0.073 to 0.390)]. Higher estradiol levels were associated with significantly higher CRP levels [0.179 (0.120 to 0.237)] and lower TFPI levels [−0.263 (−0.414 to −0.111)]. Finally, higher SHBG levels were associated with significantly higher CRP [0.154 (0.092 to 0.216)], but with lower TFPI [−0.461 (−0.620 to −0.302) and PAI-1 [−0.334 (−0.486 to −0.183)]. Data are also presented as the log transformed standard deviations of hormone level and log transformed biomarkers with p-values (Supplementary Table S4). Data are also presented for the type of HT used in the form of estrogen only versus estrogen+progesterone. We saw several more potentially prothrombotic associations between biomarkers and sex hormone levels in the estrogen+progesterone users (N = 8 significant potentially prothrombotic associations) when compared with the estrogen-only users (N = 5 significant potentially prothrombotic associations). A qualitative difference of associations by HT type was observed: SHBG is negatively associated with CRP levels in estrogen and progesterone users, but it is positively associated with CRP in estrogen-only users (Supplementary Tables S3 and S4).
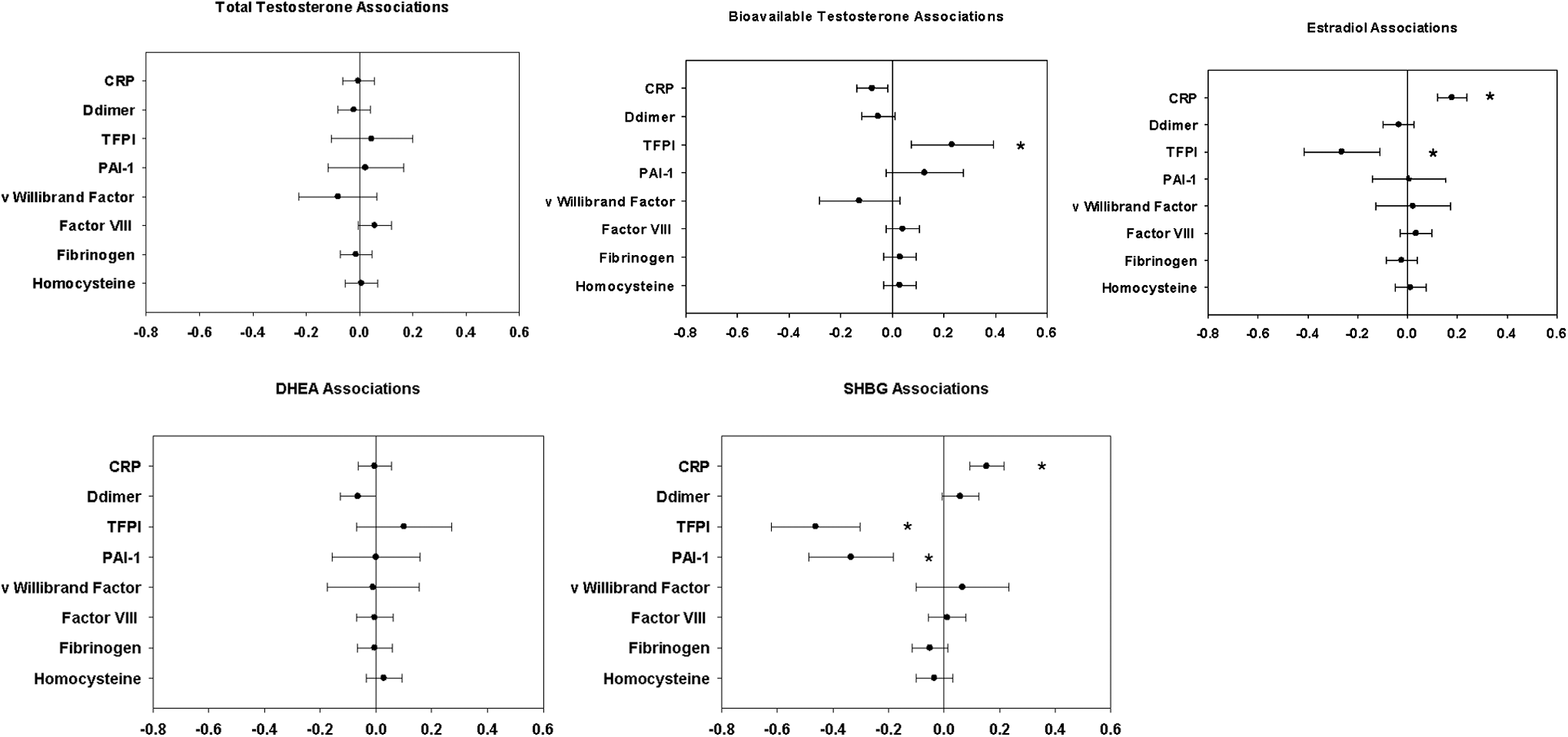
Associations of sex hormone levels with thrombosis biomarkers. Among users of hormone therapy, the plot shows the difference in the biomarker level (represented as the increment of its SD) for each SD higher serum sex hormone level after adjustment for age, BMI, race, hypertension, smoking, and diabetes. *p ≤ 0.00625.
Discussion
The current study is a cross-sectional analysis of postmenopausal women. Given the multiple comparisons of this large cohort, we will first discuss the associations that support a prothrombotic milieu, followed by those associations that do not suggest prothrombosis. Overall, we found more frequent associations between serum sex hormone levels and thrombotic biomarkers in HT nonusers than in HT users. Potential considerations for the increased associations in the nonusers may be a result of the difference in age, incidence of diabetes, systolic and diastolic blood pressures, and incidence of obesity between the two groups, all of which are statistically significant. However, we did find associations that could contribute to a prothrombotic milieu in HT users. In particular, elevated levels of estradiol and SHBG in HT users were associated with elevated levels of CRP and lower levels of TFPI, both of which are considered to be prothrombotic. This combination of lower TFPI and higher CRP is a very plausible explanation for a prothrombotic state as it relates to HT. 21 –23 This directly contrasts the findings we observed in women not on HT in whom higher SHBG levels were associated with lower CRP and had no association with TFPI levels. Of note, oral contraceptive agents that are associated with a high venous thrombosis risk have been found to have lower levels of TFPI in addition to lower levels of protein S. 24 TFPI is a Kunitz-type proteinase inhibitor, which can reversibly inhibit factor Xa (FXa). FXa/TFPI complex prevents activation of Factor IX. FXa/TFPI binds in a second step to the FVII/TF complex, thus leading to inactivation of tissue factor, leading to reduced thrombosis. 25 Therefore, a reduction in TFPI can lead to uninhibited factors, IXa, Xa, and VIIa, thereby increasing thrombotic potential. This may serve as a plausible explanation for the increased thrombosis seen in women on HT. On the other hand, it may suggest that lower TFPI or higher CRP with HT reflects estrogenicity as measured by SHBG. Oral contraceptive therapy is associated with lower TFPI, which is associated with an increased risk of venous thrombosis. 26 Certain combined oral contraceptive agents associated with increased venous thrombosis have also been found to lead to elevated SHBG and activated protein C resistance. 27,28 In the Women's Health Initiative trials of postmenopausal hormone therapy, although TFPI was reduced by HT, this reduction was not associated with an increased risk of ischemic stroke. 29 Our further analysis within the HT users alone revealed that estrogen-only users who had elevated levels of SHBG had elevated CRP levels, but among estrogen and progesterone users, those with higher levels of SHBG had lower CRP levels. However, on the whole, we saw several more potentially prothrombotic associations between biomarkers and sex hormone levels in the estrogen+progesterone users when compared with the estrogen-only users. This seems to fit with Women's Health Initiative (WHI) clinical findings of increased cardiac risk with the combined use of estrogen and progesterone. 30 Several studies have also reported an increase in CRP with HT, and CRP is a known risk factor for coronary events. 11,12,23,31,32 Therefore, the connection between thrombosis and HT may also be explained by elevations in CRP. 33 A particular strength of our study is that it is the first of its kind that we are aware of to examine serum sex hormone associations in HT in relation to thrombotic risk markers in a large ethnically diverse cohort. We observed that higher bioavailable testosterone was associated with higher CRP in HT nonusers. We know that increased androgenicity in postmenopausal women is associated with an unfavorable cardiovascular inflammatory risk profile and as such our results support this fact given that we found higher fibrinogen and CRP in non-HT users. 34
We also found evidence of an antithrombotic milieu as well with an association between higher SHBG and lower PAI-1 levels in both HT users and nonusers, which would suggest a favorable vascular risk. These conflicting results, as they relate to differences in SHBG associations with prothrombotic markers in HT users, may suggest that the prothrombotic risk with HT may in fact not be mediated by alterations in these particular biomarkers and perhaps may be due to yet unmeasured biomarkers.
We also observed that HT nonusers with higher levels of bioavailable testosterone had lower homocysteine levels; however, HT users did not have lower homocysteine levels. Walsh et al. studied homocysteine and CRP levels in a clinical trial and found that hormone replacement therapy led to decreased homocysteine levels. 35
Higher DHEA was associated with higher fibrinogen and CRP in this study, but only among HT nonusers. Given the lack of similar findings in HT users, it may be interpreted that HT use could be protective in modulating elevations of fibrinogen and CRP associated with DHEA. DHEA is a precursor of androstenedione, testosterone, and estrogen. 36 It is postulated that high levels of androgens potentially increase cardiovascular risk in women through effects on lipids, blood pressure, glucose, and insulin metabolism. 37,38 We are not aware of other studies that reported associations of DHEA with thrombotic and inflammatory markers in the setting of HT use.
Study limitations
This is a cross-sectional study, therefore causality cannot be determined. Given that there were significant differences in characteristics between the groups of women on HT and those not on HT, we could not interpret the direct effects of HT on biomarkers, nor on serum sex hormones. We did not have information on the specific estrogen compound taken by many of these women on HT. In addition, the MESA study only assayed total TFPI and not the biologically active free TFPI, which has been extensively studied. The lack of the ability to compare associations for transdermal versus oral HT is a particular limitation; however, the majority of the participants were on oral HT. Another limitation includes the inability to distinguish which estrogen compounds were used since various estrogen compounds contain multiple variations of estrogen, all of which may have slightly different physiologic effects on thrombotic factors. We have also made multiple comparisons; however, we have used the Bonferroni correction for examining several p-values to test hypotheses and included only those that were highly significant (p < 0.00625). A great strength of the current study is the large number of women studied.
Conclusion
We sought to identify associations between serum sex hormones and thrombotic biomarkers that may give insight into mechanisms by which HT increases the risk of arterial thrombosis. A particular strength of our study is that it is the first of its kind that we are aware of to examine serum sex hormone associations in HT in relation to thrombotic risk markers in a large ethnically diverse cohort.
We found that elevated levels of estradiol and SHBG in HT users were associated with elevated levels of CRP and lower levels of TFPI, both of which may provide insight into a possible mechanism of a prothrombotic milieu of HT. Although HT nonusers had elevated levels of CRP associated with higher levels of estradiol, they did not have lower levels of TFPI associated with higher estradiol levels, which may further strengthen the evidence for TFPI as a potential mechanism of prothrombosis in HT users. Further studies are required to examine the exact mechanism of this prothrombotic state. HT nonusers had far more prothrombotic associations between elevated serum sex hormone levels and thrombotic biomarkers when compared with HT users.
Footnotes
Acknowledgments
This research was supported by contracts, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, and N01-HC-95169, from the National Heart, Lung, and Blood Institute and by grants, UL1-TR-000040 and UL1-TR-001079, from NCRR and NIDDK K23DK093583. The authors thank the other investigators, the staff, and the participants of the MESA study for their valuable contributions. A full list of participating MESA investigators and institutions can be found at
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.