
Abstract
In 2011, the American Heart Association (AHA) issued the pivotal “Effectiveness-based Guidelines for the Prevention of Cardiovascular Disease in Women–2011 Update.” In the interim, multiple guidelines have dramatically altered recommendations for preventive cardiovascular care. This article addresses how I juggle these multiple guidelines in my clinical practice. In brief, my approach to risk stratification is to use the Pooled Cohort Equations, but I also routinely assess the risk factors unique to or predominant in women such as pregnancy complications and systemic autoimmune collagen vascular diseases. I follow the 2013 AHA/American College of Cardiology (ACC) Guidelines on Lifestyle Management to Reduce Cardiovascular Risk, but find value in the detailed aspects of physical activity recommendation in the 2011 Women's Guideline, including those for weight loss or weight loss maintenance. Based solely on epidemiological data, I consider a blood pressure (BP) of 120//80 mmHg ideal in women who remain asymptomatic at that level. I typically titrate BP therapy to 120–130/80–90 mmHg as tolerated. I endorse the current ACC/AHA recommendations for cholesterol management, but for my women patients older than age 75 who previously tolerated a high-intensity statin, I continue that medication or whatever statin they tolerated through age 75. For women older than age 75 with a recent acute atherosclerotic cardiovascular disease (ASCVD) event, a high-risk population, I follow the guideline for younger patients. As ASCVD events are becoming more common before 40 years of age, I screen younger women earlier when risk factors unique to or predominant in women are present. I incorporate sex-specific risk factors for stroke in the risk ascertainment component of women's medical records. With regard to depression, at minimum I perform screening for all women with coronary heart disease with a 2-item Patient Health Questionnaire (PHQ-2). For women with suspected ischemic heart disease, I adhere to the recommendations of the 2014 Consensus Statement of the AHA, “The Role of Noninvasive Testing in the Evaluation of Women with Suspected Ischemic Heart Disease.” An unmet need remains an updated guideline on Prevention of Cardiovascular Disease in Women.
Assessment of Cardiovascular Risk
T
Unfortunately, these classifications represented clinical trial data published before 2011. What should our approach be to subsequently issued evidence-based guidelines?
In 2013, the American College of Cardiology (ACC)/AHA released a guideline for the Assessment of Cardiovascular Risk. 4 The algorithm for this risk assessment is presented in Figure 1. This approach incorporates use of the Pooled Cohort Equations that are gender and race specific and incorporate total cholesterol, high-density lipoprotein (HDL) cholesterol, treatment for hypertension, smoking status, age, systolic blood pressure (BP), and the presence of diabetes. 5 This atherosclerotic cardiovascular disease (ASCVD) Risk Estimator is reproduced in Figure 2. The Pooled Cohort Equations add stroke events to CHD events, that is, they expand the ASCVD composite and include serious nonfatal outcome events as well as mortality. Thus, the addition of the ASCVD Risk Estimator has particular value for women related to this expansion of the composite endpoints.
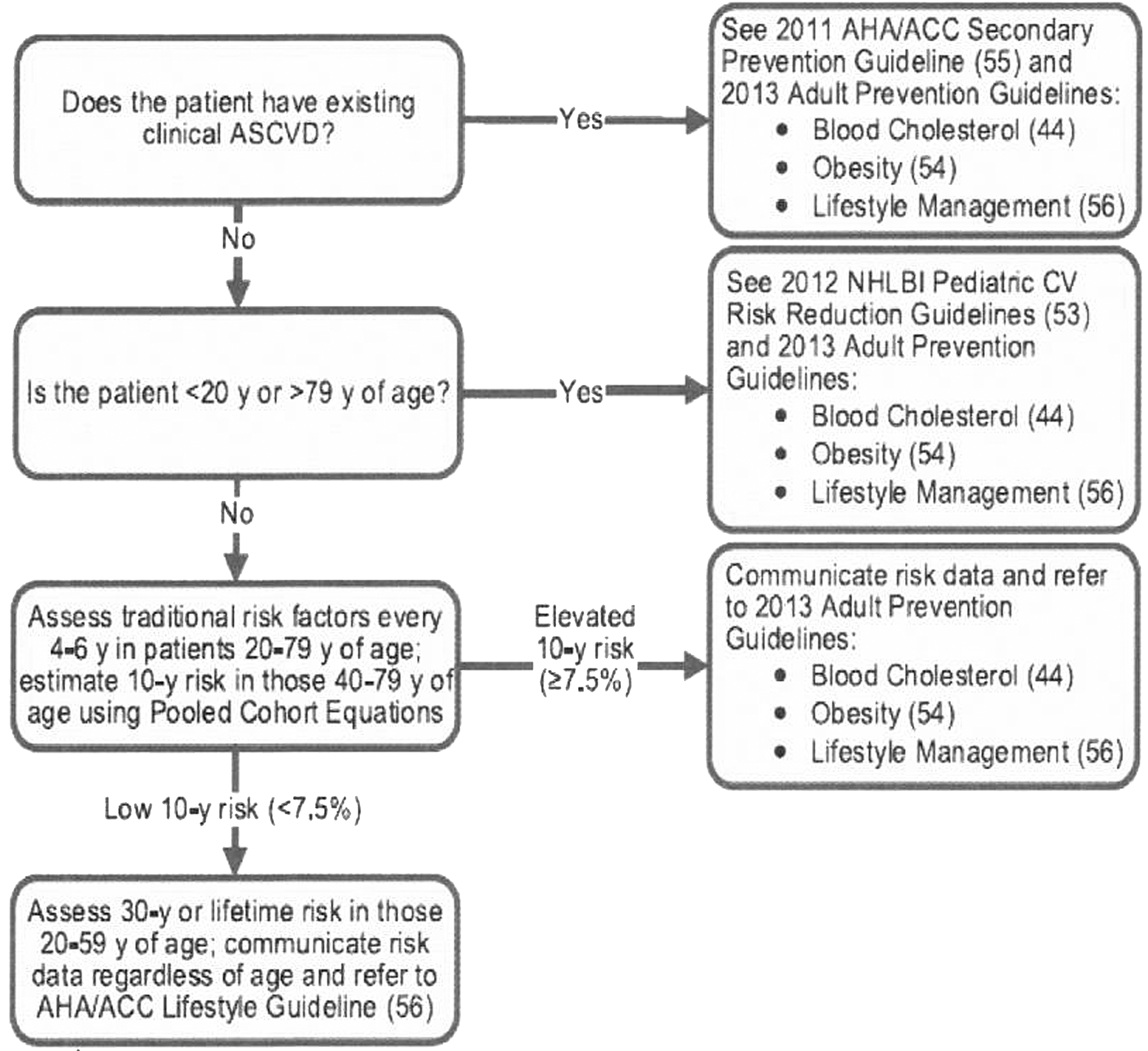
Implementation of Risk Assessment Work Group recommendations. ACC, American College of Cardiology; AHA, American Heart Association; ASCVD, atherosclerotic cardiovascular disease; CV, cardiovascular; NHLBI, National Heart, Lung, and Blood Institute. Source: Goff et al. 4
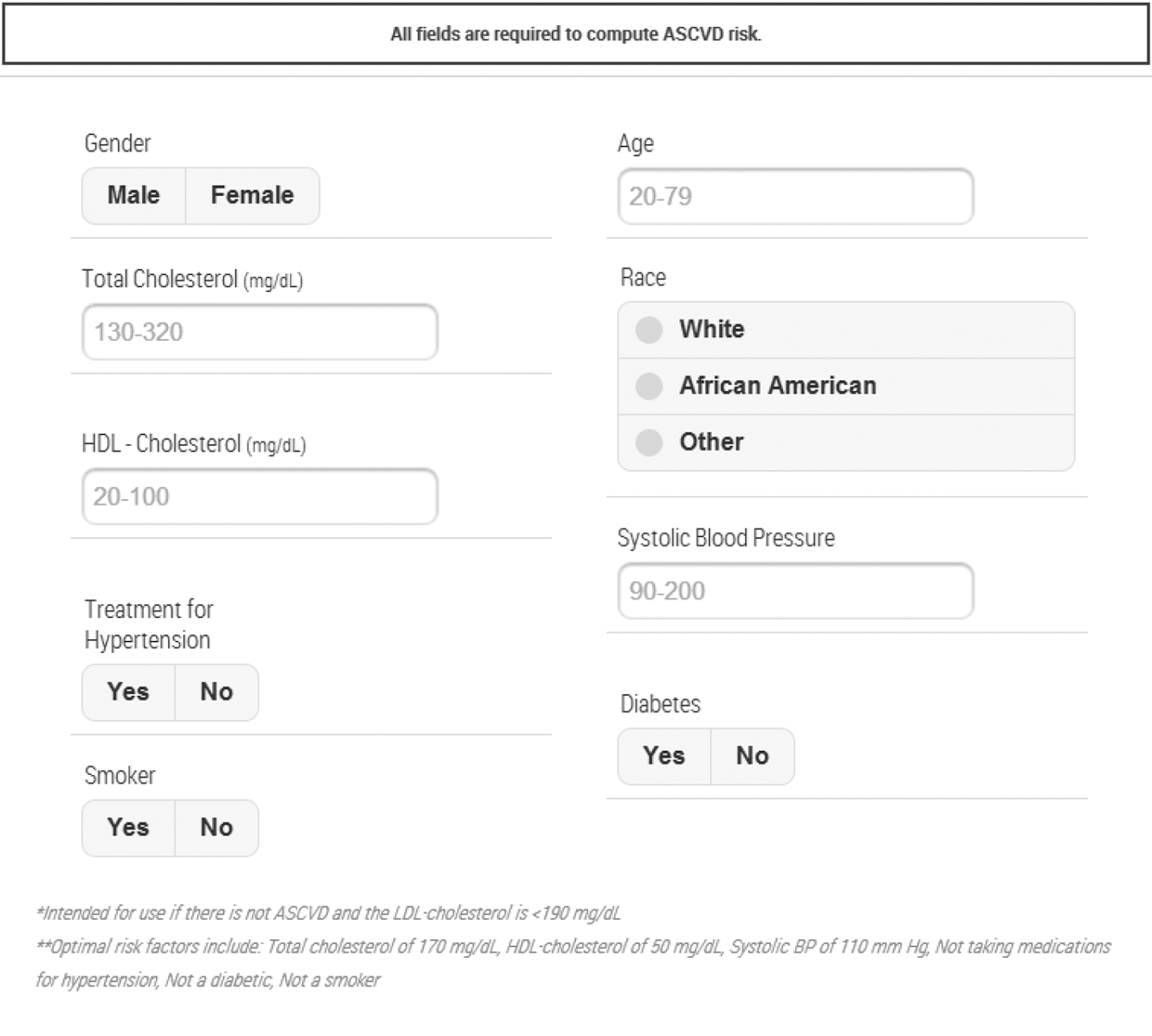
ASCVD Risk Estimator. Source:
My approach to risk stratification is to use the currently preferred Pooled Cohort Equations, which have since been reasonably validated in several cohorts of women, including one from the Women's Health Initiative. The database for the Equations is derived from more recently published national research studies. I also routinely assess and consider the risk factors unique to or predominant in women, for example, pregnancy complications and systemic autoimmune collagen vascular diseases (see below).
Risk Factors Unique to or Predominant in Women
Preeclampsia, gestational diabetes, pregnancy-induced hypertension
The 2011 Women's Cardiovascular Prevention Guidelines highlighted as a risk factor a history of preeclampsia, gestational diabetes, or pregnancy-induced hypertension. 6 –9
A detailed pregnancy history is an integral component of risk assessment for women, in that pregnancy complications, including preeclampsia, gestational diabetes, pregnancy-induced hypertension, and preterm delivery, all constitute early indicators of increased CVD risk. It has been stated that pregnancy is often the first stress test a woman undergoes. Identification of the cardiovascular and metabolic stresses of pregnancy offers the potential for early prediction of increased CVD risk; this likely reflects shared risk factors for preeclampsia and CVD, rather than responses to the pregnancy complications. Preeclampsia, gestational diabetes, and gestational hypertension confer a threefold to sixfold increased risk for subsequent development of hypertension, and a threefold increase in the subsequent development of ischemic heart disease and stroke. Gestational diabetes increases sevenfold the risk for the development of Type II diabetes mellitus. Although the preeclampsia subsides with delivery of the placenta, there is residual endothelial dysfunction demonstrated at subsequent testing and this has been associated with a subsequent increase in the presence of coronary artery calcium. Women with these pregnancy complications should have CVD risk factor screening with appropriate education, counseling, and preventive interventions.
Systemic autoimmune collagen vascular disease
The 2011 Women's Cardiovascular Prevention Guidelines further identified systemic autoimmune collagen vascular disease (e.g., lupus erythematosus or rheumatoid arthritis) as a major risk factor. These systemic autoimmune disorders are highly prevalent in women and increase the risk of CHD and cerebrovascular accident. 10 –12 CHD is the leading cause of morbidity and mortality in women with systemic lupus erythematosus. There is twofold to threefold increase in myocardial infarction (MI) and CVD mortality associated with rheumatoid arthritis. More recently, psoriasis and psoriatic arthritis have been shown to increase the risk of CVD events, but not CVD mortality. Hence, the presence of a systemic autoimmune collagen vascular disorder warrants increased screening of these women for CVD risk factors and appropriate preventive interventions.
Guidelines for Preventing CVD in Women
The 2011 Women's Guidelines divide the preventive approaches into lifestyle interventions, major risk factor interventions, and preventive drug interventions. These are serially addressed.
Lifestyle interventions
The 2011 Women's Guidelines for physical activity advised women to accumulate at least 150 minutes weekly of moderate exercise, 75 minutes weekly of vigorous exercise, or an equivalent combination of moderate- and vigorous-intensity aerobic physical activity. Aerobic activity was advised to be performed in episodes of at least 10 minutes of duration, preferably spread throughout the week (Class I, Level of evidence A). A similar class and level of evidence recommendation addressed that additional cardiovascular benefits were provided by increasing moderate-intensity aerobic physical activity to 300 minutes weekly, 2½ hours of vigorous-intensity physical activity weekly, or a combination of both, with added advice to engage in muscle-strengthening activities that involved all major muscle groups on ≥2 days of the week.
Two years later, in 2013, the AHA/ACC guideline on Lifestyle Management to Reduce Cardiovascular Risk 13 presented recommendations for adults (without specific gender recommendations) to engage in aerobic physical activity to reduce low-density lipoprotein cholesterol (LDL-C) and non-HDL cholesterol (non-HDL-C): three to four sessions per week, lasting an average of 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. Adults were also advised to engage in aerobic physical activity to lower BP: three to four sessions weekly, lasting an average of 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. The physical activity recommendations were specifically targeted to cholesterol and BP control, with an identical exercise recommendation offered for both. No gender-specific recommendations were listed.
The 2011 Women's Guidelines advised women who needed to lose weight or sustain weight loss to accumulate a minimum of 60–90 minutes of at least moderate-intensity physical activity (e.g., brisk walking) on most and preferably all days of the week; no comparable recommendation was offered in the 2013 Guideline on Lifestyle Management, although there is a separate guideline on overweight/obesity that recommends a comprehensive long-term lifestyle program. 14
My approach: I follow the 2013 AHA/ACC Guidelines on Lifestyle Management to Reduce Cardiovascular Risk, but find value in the detailed aspects of physical activity in the 2011 Women's Guideline, including those for weight loss or weight loss maintenance. My women patients appreciate these specifics either for independent exercise or to guide a structured, supervised exercise program.
Major risk factor interventions
Blood pressure
The 2011 AHA Women's Guidelines indicate that an optimal BP of <120/80 mmHg should be encouraged through lifestyle approaches, including weight control, increased physical activity, alcohol moderation, sodium restriction, and increased consumption of fruits, vegetables, and low-fat dairy products (Class I; Level of evidence B).
The AHA Lifestyle Guideline previously cited 13 identified physical activity as a preventive lifestyle recommendation, but there is major contention regarding BP goals and hypertension management among the professional societies. A 2015 Scientific Statement from the AHA, the ACC, and the American Society of Hypertension 15 recommended the <140/90 mmHg BP target as reasonable for the secondary prevention of cardiovascular events in patients with hypertension and coronary artery disease (CAD) (Class IIa, Level of evidence B) and identified that a lower target BP (<130/80 mmHg) may be appropriate in some individuals with CAD, previous MI, stroke or transient ischemic attack, plus CAD risk equivalents (carotid artery disease, peripheral arterial disease, abdominal aortic aneurysm) (Class IIb, Level of evidence B). These guidelines address only patients with CAD. Other guidelines 16,17 have offered differing recommendations, with most contentious being BP goals in elderly patients.
Eighth Joint National Committee (JNC8) 17 identified strong evidence supporting treating hypertensive patients aged ≥60 years to a BP goal of <150/90 mmHg and those aged 30–59 years to a diastolic BP goal of <90 mmHg. Not evidence-based but based on expert opinion, a BP goal of <140/90 mmHg was recommended as a systolic BP goal for those aged <60 years or a diastolic BP goal for those aged <30. The same goals were recommended for hypertensive adults with diabetes or nondiabetic chronic kidney disease as for the global population <60 years old. A Science Advisory from the AHA/ACC/Centers for Disease Control and Prevention (CDC) 16 recommended a BP goal of <140/90 mmHg for most people, indicating that lower targets may be appropriate for some populations. Lifestyle modifications were advised for all patients.
My approach: Based solely on epidemiological data I consider a BP of 120/80 mmHg ideal in women who remain asymptomatic at that level; epidemiological data indicate an increased risk beyond that BP level, even at older age. In the Women's Health Initiative, adverse outcomes of women with prehypertension were intermediate between those for normotensive women and hypertensive women. I typically titrate BP therapy to 120–130/80–90 mmHg as tolerated.
My approach was very recently validated by premature termination and release of preliminary results from the NIH SPRINT (Systolic Blood Pressure Intervention Trial) study. Using medications to reduce systolic BP to 120 mmHg reduced rates of heart attack, heart failure, and stroke by nearly one-third and death by nearly one-fourth compared to reducing systolic BP to <140 mmHg.
Cholesterol management
The 2011 Women's Prevention Guidelines addressed optimal lipid and lipoprotein levels, including lifestyle and pharmacological interventions. The following levels of lipids and lipoproteins were to be encouraged initially through lifestyle approaches: LDL-C < 100 mg/dL, HDL-C > 50 mg/dL, triglycerides <150 mg/dL, and non-HDL-C (total cholesterol minus HDL) <130 mg/dL (Class I, Level of evidence B). Specific recommendations were presented for pharmacotherapy for LDL lowering; I cite as an example only those for high-risk women. LDL-C-lowering drug therapy was recommended simultaneously with lifestyle approaches in women with CHD to achieve an LDL-C < 100 mg/dL (Class I, Level of evidence A); this was also indicated for women with other atherosclerotic CVD or diabetes mellitus or for women at risk of <20% (Class I, Level of evidence B). An LDL reduction to <70 mg/dL was considered reasonable in very high-risk women with CHD (e.g., those with recent acute coronary syndrome or multiple poorly controlled cardiovascular risk factors) and such women may require an LDL-lowering drug combination (Class IIa, Level of evidence B).
The subsequent 2013 ACC/AHA Guidelines on Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 18 approach is indicated in three algorithms (Figs. 3 –5). A major change in these Guidelines is the focus on LDL-C, the elimination of arbitrary LDL-C treatment targets, a prominent feature of prior Guidelines and the 2011 Women's Guidelines, and the emphasis on statin use. Recommendations for treatment of blood cholesterol were not considered to support the use of fixed LDL-C and/or non-HDL-C treatment targets and no recommendations were provided for agent-specific targets for primary or secondary prevention of ASCVD. Emphasis is rather on individual patient risk assessment to determine who should take statins and to guide the appropriate intensity of statin drugs to reduce ASCVD risk in individuals most likely to benefit. Four high-risk groups of patients were identified (without gender differences) as having the greatest statin benefit in secondary and primary prevention: (1) individuals with clinical ASCVD, (2) individuals with primary elevations of LDL-C ≥190 mg/dL, (3) individuals aged 40–75 years with diabetes and LDL-C 70–189 mg/dL but without clinical ASCVD, and (4) individuals without clinical ASCVD, aged 40–75 years of age with LDL-C 70–189 mg/dL with an estimated 10-year ASCVD risk of 7.5% or higher.
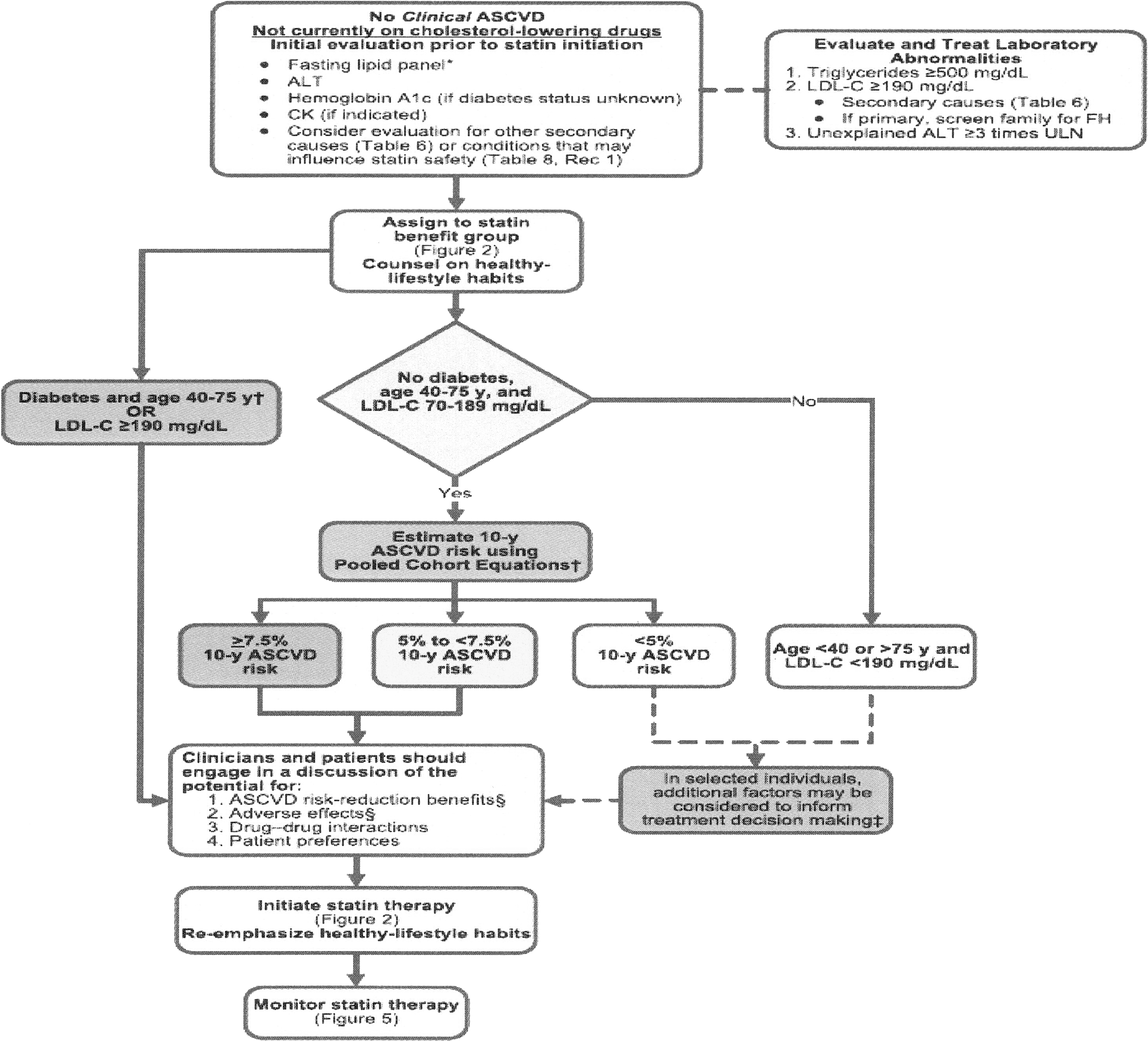
Initiating statin therapy in individuals without ASCVD. Source: Stone et al. 18
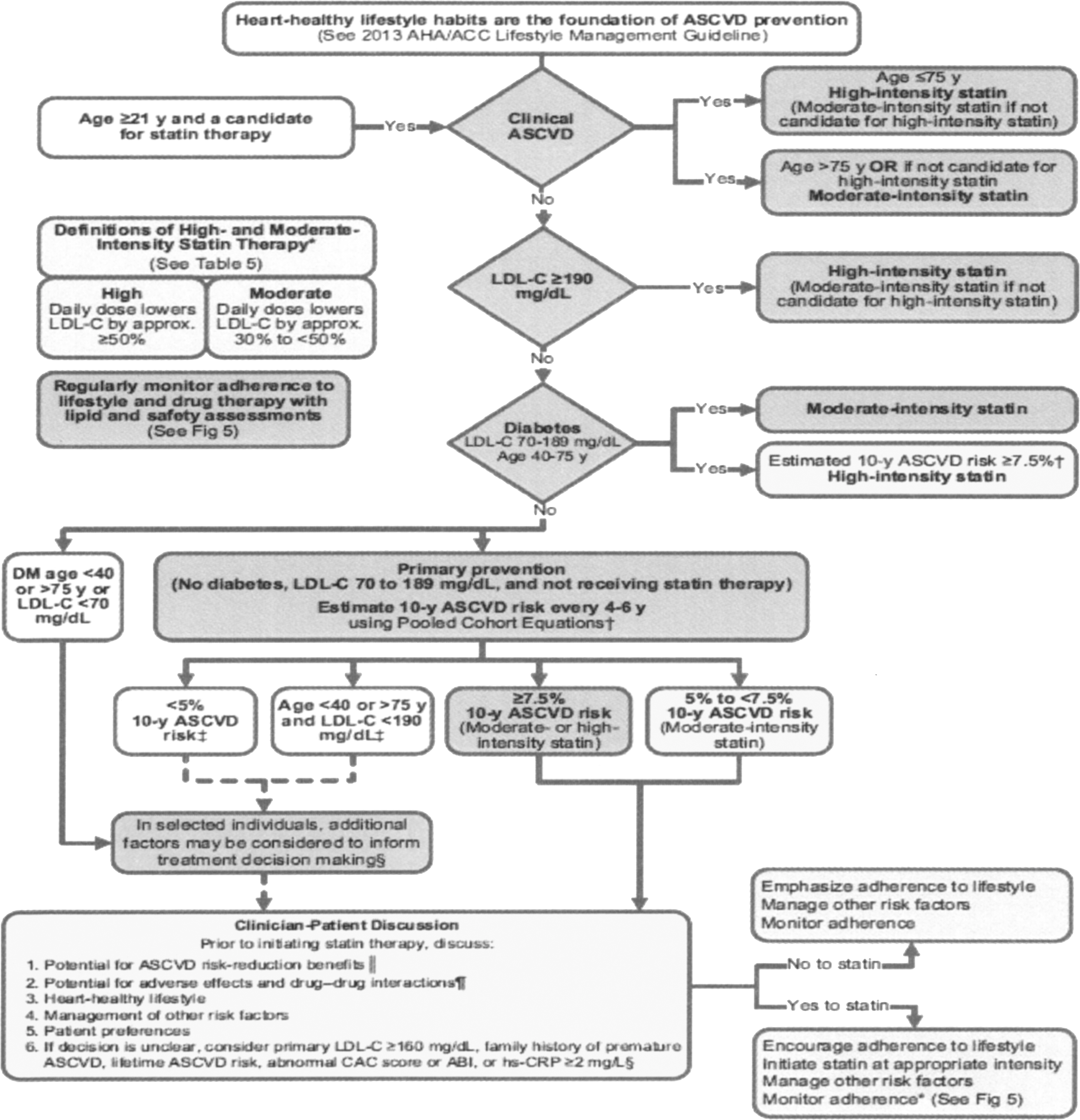
Summary of statin initiation recommendations for the treatment of blood cholesterol to reduce ASCVD risk in adults. Source: Stone et al. 18
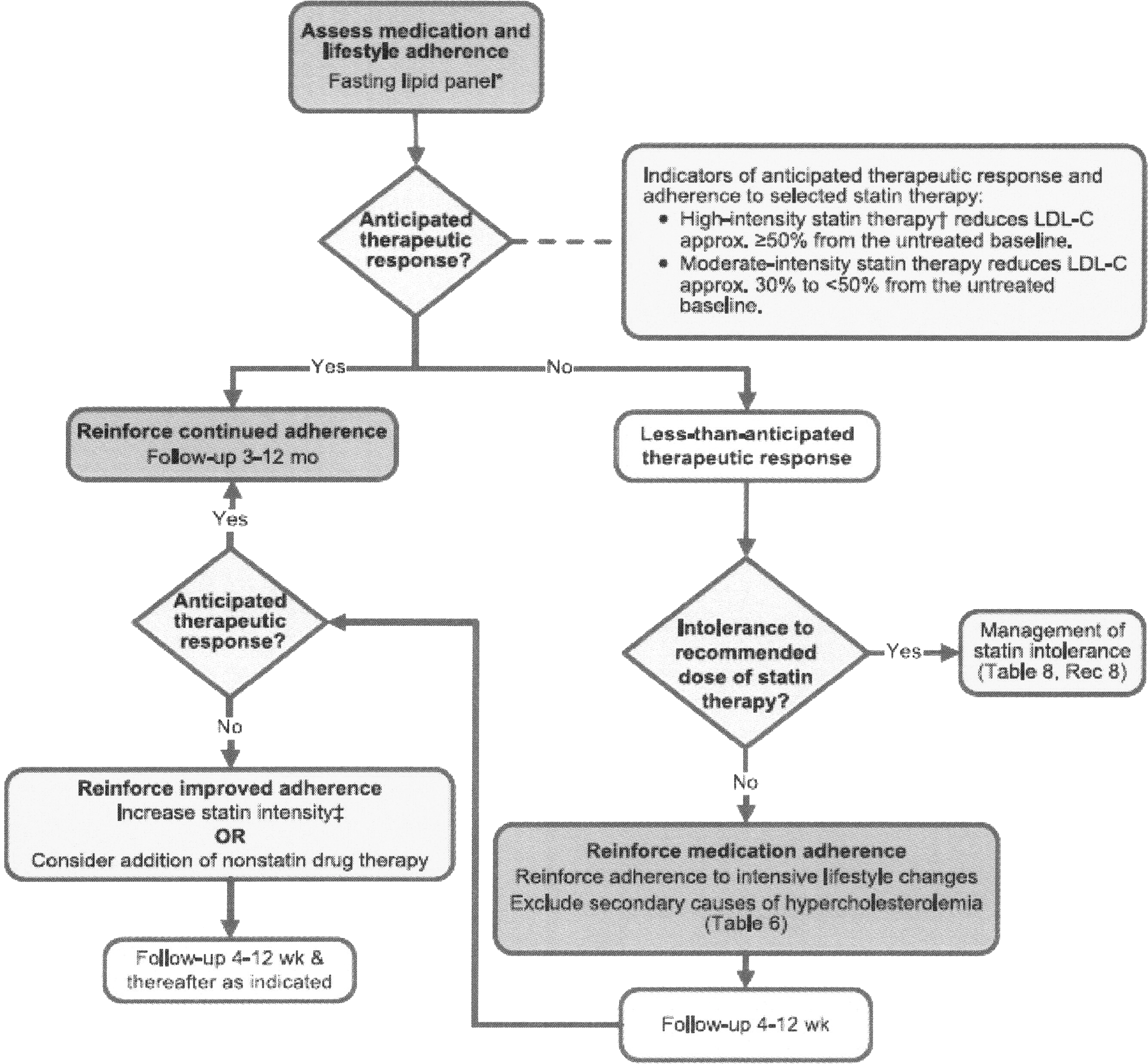
Statin therapy: monitoring therapeutic response and adherence. Source: Stone et al. 18
Statins were unequivocally recommended as the therapy of choice and a streamlined evidence-based algorithm identified these four groups of patients with the greatest statin benefits. For primary prevention patients, the algorithm highlighted individualization of decision-making based on provider–patient discussions. Nonstatin therapies were not considered to provide acceptable ASCVD risk reduction.
Lifestyle modifications were recommended before and associated with cholesterol-lowering therapy, and the Guidelines recommended use of the Pooled Cohort Equations to estimate 10-year ASCVD risk in white and black men and women. 19 Also, new to the Guideline was attention to an LDL ≥190 mg/dL, likely to represent a familial hypercholesterolemia population.
Specific secondary prevention recommendations
High-intensity statins were considered first-line therapy for women and men ≤75 years old with clinical ASCVD. When a high-intensity statin is contraindicated, or individuals have statin-associated adverse effects, a moderate-intensity statin should be used as tolerated. For individuals >75 years old with clinical ASCVD, it was considered reasonable to evaluate the potential for ASCVD reduction benefit as well as adverse drug effects, drug interactions, and to consider patient preferences when initiating or continuing moderate- or high-intensity statin use (Class IIa, Level of evidence B).
Individuals ≥21 years old with LDL-C ≥ 190 mg/dL or triglycerides ≥500 mg/dL should be evaluated for secondary causes of hyperlipidemia. They should be treated with a statin regardless of their estimated 10-year ASCVD risk, using high-intensity statin or maximum tolerated preparation if unable to tolerate high-intensity statin (Class I, Level of evidence B). It was considered reasonable to intensify statin therapy to achieve at least a 50% LDL-C reduction (Class IIa, Level of evidence B). After the maximum intensity statin was achieved, consideration of the addition of a nonstatin drug was to be addressed to further lower LDL-C (Class IIb, Level of evidence C).
My approach is to favor the current ACC/AHA recommendations but I have concern for my women patients older than age 75, many of whom have ASCVD. If they previously tolerated a high-intensity statin, I continue that medication or whatever statin they have tolerated through age 75. Initiation of statin therapy after age 75 is so infrequent that it does not warrant discussion. For women older than age 75 who have incurred a recent ASCVD event, I follow the guideline for younger patients because these older women (for whom we have no clinical trial data) constitute a high-risk population. I also have great concern for younger women as ASCVD events are becoming more common before 40 years of age and I screen earlier when risk factors unique to or predominant in women are present. 20,21 In discussions about statins with my women patients, I highlight the lack of differing gender recommendations in the 2013 Cholesterol Guideline. Although substantial outcome evidence is present for secondary prevention, primary prevention benefit although present is less powerful owing to limited representation of women in primary prevention trials and their occurrence of outcome events at older age. Discussion of risk of transitioning to diabetes mellitus is appropriate, although this risk is substantially outweighed by the potential beneficial effects of statins. There is no definitive evidence that statins lead to cognitive decline.
Class III Interventions: Not Useful/Effective and May Be Harmful for CVD Prevention in Women
My approach: There should be no change but continued attention to avoiding the Class III interventions cited in the 2011 Women's Cardiovascular Prevention Guidelines. 1 Elimination of ineffective preventive interventions focuses attention on those with documented efficacy.
Menopausal hormone therapy
Hormone therapy and selective estrogen receptor modulators should not be used for the primary or secondary prevention of CVD. This has been re-emphasized by recommendations from the US Preventive Services Task Force. 22
Antioxidant supplements
Antioxidant vitamin supplements (e.g., vitamin E, C, and beta carotene) should not be used for the primary or secondary prevention of CVD. 23,24
Folic acid
Folic acid, with or without vitamin B6 and B12 supplementation, should not be used for the primary or secondary prevention of CVD. 25
Aspirin for MI in women ≤65 years of age
Routine use of aspirin in healthy women <65 years of age is not recommended to prevent MI. 26
What Else Is New and Relevant?
Risk guidelines for the prevention of stroke in women
A 2014 Statement for Healthcare Professionals from the AHA/American Stroke Association identified guidelines for the prevention of stroke in women. 27 Stroke risk factors were categorized as those that are sex specific, stronger, or more prevalent in women, or similar between women and men (Table 1).
Source: Bushnell et al. 27
Sex-specific risk factors include pregnancy, preeclampsia, gestational diabetes, oral contraceptive use, postmenopausal hormone use, and changes in hormonal status. Risk factors that are stronger or more prevalent in women include migraine with aura, atrial fibrillation, diabetes mellitus, hypertension, depression, and psychosocial stress. Risk factors with a similar prevalence in women and men and an unknown difference in impact include physical inactivity, age, prior CVD, obesity, diet, smoking, and the metabolic syndrome.
My approach: Since stroke is more common in women than men, these guidelines are a useful addition to our diagnostic and therapeutic armamentarium. Sex-specific risk factors for stroke in women should be incorporated in the risk ascertainment component of the electronic medical record.
Depression
A Scientific Statement from the AHA 28 identifies “Depression as a Risk Factor for Poor Prognosis Among Patients with Acute Coronary Syndrome: Systematic Review and Recommendations.” Despite the heterogeneity of the published studies included in this review, the preponderance of evidence supports the recommendation that the AHA should elevate depression to the status of a risk factor for adverse medical outcomes in patients with acute coronary syndrome.
Depression occurs frequently in women living with CVD. Research data demonstrate a link between CAD and depression, with an increased prevalence of depression in younger women with CVD. Depression is an independent risk factor for CVD and is associated with worse outcomes, particularly for women. Despite the recommendation to screen for depression in women with ASCVD in the 2011 Women's Prevention Guidelines, depression is rarely screened for in women with any form of CVD, despite its adverse impact on outcomes. 29
My approach: At a minimum, screening should be performed for all women with CHD with a 2-item CHD Patient Health Questionnaire (PHQ-2), 30 and ideally particularly in hospitalized women, with the PHW-9 Questionnaire (Developed by Drs. Robert L. Spitzer, James B.W. Williams, Kurt Kroenke and colleagues, with an educational grant from Pfizer, Inc. No permission required).
The role of noninvasive testing in women with suspected ischemic heart disease
In 2014, a Consensus Statement from the AHA addressed the “Role of Noninvasive Testing in the Evaluation of Women with Suspected Ischemic Heart Disease.” 31 Although not strictly related to preventive interventions, suspected ischemic heart disease is often the initial diagnostic entry of women into the clinical care system, in that angina is more often the initial presentation of CVD in women than in men.
The underlying considerations regarding the initial diagnostic procedure relate to the fact that extensive comorbidity, multiple risk factors, and functional disability increase the ischemic heart disease risk category. In general, low-risk women are not generally candidates for further diagnostic testing and should be assessed for non-stable ischemic heart disease as etiological for their symptoms. For low- or intermediate-risk women, the exercise ECG is the preferred study for functionally capable women with an interpretable resting electrocardiogram. For intermediate- to high-risk women, stress imaging or coronary computed tomographic angiography (CCTA) can assess ischemic burden and guide anti-ischemic therapy and clinical decision-making. For high-risk stable women, stress imaging is important, but concern should always be present to reduce ionizing radiation. The diagnostic algorithm is presented in Figure 6.
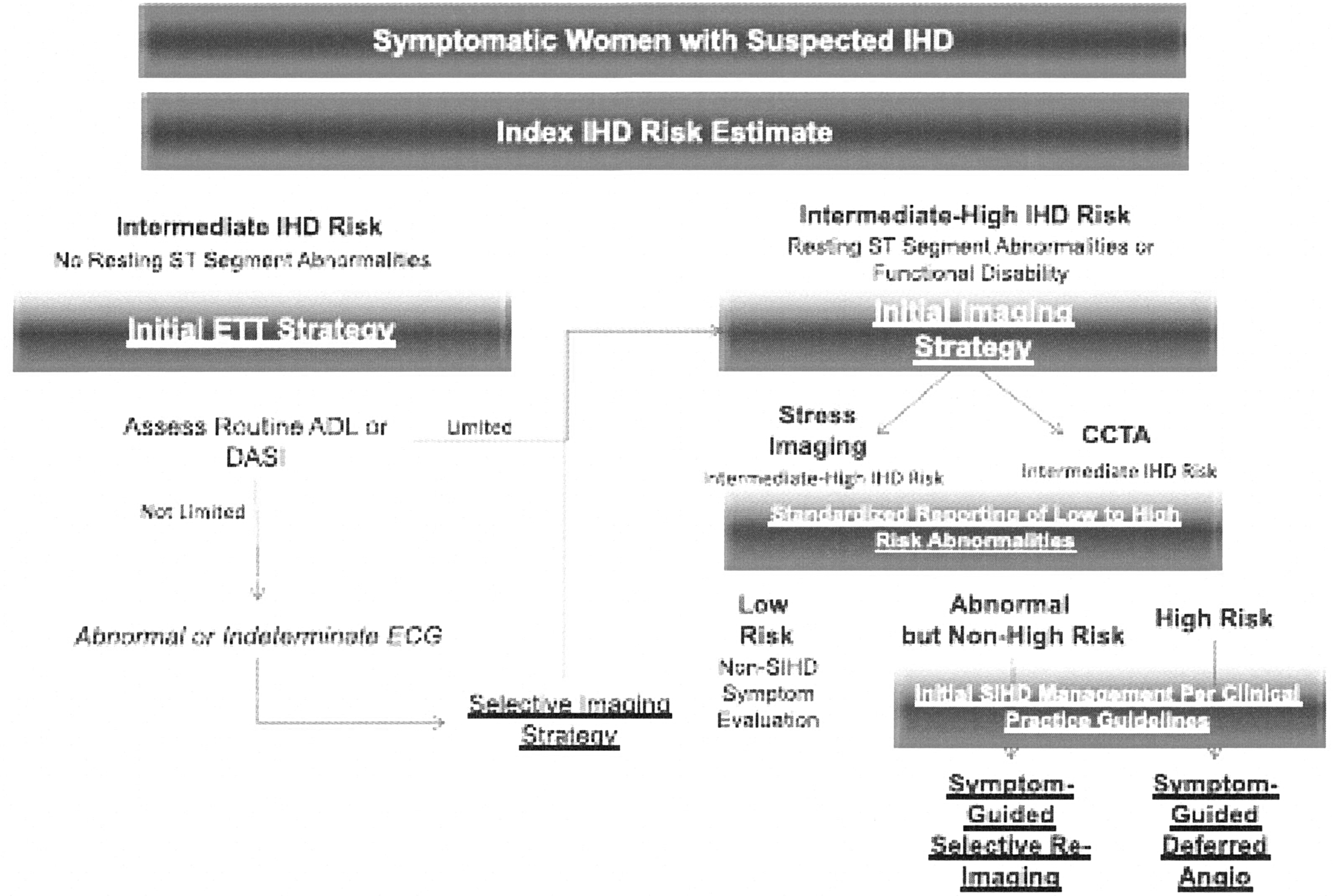
Diagnostic evaluation algorithm for women presenting with suspected ischemic heart disease (IHD) symptoms and intermediate IHD risk and intermediate IHD risk. ADL, activities of daily living; Angio, angiography; CCTA, coronary computed tomography angiography; DASI, Duke Activity Status Index; ETT, exercise treadmill testing; SIHD, stable ischemic heart disease. Source: Mieres et al. 31
To summarize, most low-risk symptomatic women are not candidates for diagnostic testing. The exercise ECG is the initial strategy for low–intermediate ischemic heart disease risk women. Symptomatic women with functional disability, an abnormal resting electrocardiogram, or an indeterminate exercise test result should have echocardiography, myocardial perfusion imaging, or cardiac magnetic resonance imaging (CMR) as reasonable options, with preference for echocardiography or CMR for premenopausal women because of radiation exposure. CCTA is reasonable for women at intermediate ischemic heart disease risk and provides unique information about the burden of obstructive CAD. Risk stratification is based on the extent and severity of inducible abnormalities.
My approach: As a coauthor of this document, I follow the recommendations. Many women present to the office with results of coronary calcium or carotid IMT testing either done independently or ordered by another clinician. Current evidence-based recommendations do not support such screening but accumulating evidence for coronary calcium may change future guidelines. Coronary calcium can be equated with atherosclerosis and conventional coronary risk intervention should be instituted.
Summary: Juggling Multiple Guidelines: What Is the Prudent Approach?
First is to use the 2011 Women's Prevention Guidelines where applicable, as noted earlier. The outdated recommendations should be replaced by more contemporary guidelines regarding cardiovascular risk assessment, lifestyle management, treatment of blood cholesterol, and noninvasive testing for suspected ischemic heart disease.
New information is highly relevant to clinical practice, particularly guidelines on the prevention of stroke and the issue of depression as a risk factor for women. The treatment of hypertension is a work in progress, with new recommendations expected shortly. Importantly, stay vigilant for new guidelines.
An unmet need is an updated guideline on Prevention of Cardiovascular Disease in Women.
Footnotes
Author Disclosure Statement
No competing financial interests exist.