
Abstract
Background:
For nonvalvular atrial fibrillation (NVAF), novel oral anticoagulants (NOACs) have been found noninferior to warfarin for stroke/systemic embolization prevention, and major bleeding events. Recent meta-analysis of NOACs versus warfarin in atrial fibrillation (AF) showed that women on warfarin have greater risk of stroke/embolism than men, and when both are treated with NOACs, differences disappear.
Methods:
NOACs differ in pharmacologic properties, thus they may differ from one another in their effects on women with AF. Using dose-adjusted warfarin as the common comparator, an indirect comparison of rivaroxaban, apixaban, dabigatran 110 and 150 mg, and edoxaban 30 and 60 mg for efficacy (stroke/embolism prevention) and safety (major bleeding events) in women with AF was performed. Data from ROCKET-AF, RE-LY, ENGAGE AF TIMI, and ARISTOTLE were analyzed and compared according to the Bucher method.
Results:
No significant difference was found for any NOAC compared with alternatives in safety or efficacy for women with AF. Examination of odds ratio comparisons alone showed possible favorable efficacy in dabigatran 150 mg, and unfavorable efficacy with favorable safety in edoxaban 30 mg.
Conclusion:
NOACs may slightly differ in their effect in women; the potential differences are very small and likely clinically negligible. Thus, NOACs can be used interchangeably in women according to patient and physician preferences to increase adherence.
Introduction
I
A recent meta-analysis of NOACs versus warfarin demonstrated that women with atrial fibrillation (AF) treated with warfarin have a significantly greater risk of CVA and systemic embolism than their male counterparts. However, when both sexes are treated with NOACs that are deemed superior to warfarin (dabigatran, rivaroxaban, and apixaban), gender difference in stroke and systemic embolism disappears. 8 In the aforementioned meta-analysis, the NOACs were also associated with significantly less major bleeding in women as compared with men. The findings were, in part, attributed to pharmacokinetic and pharmacodynamic advantages of NOACs compared with warfarin, including time to therapeutic range and lack of peaks and valleys in anticoagulation. Given that all of the NOACs differ in at least one of the following properties, including absorption, distribution, metabolism, excretion, and in some cases, mechanism of action, the question remained as to how these agents compared with one another in the female population with NVAF. Prior adjusted indirect comparisons of the NOACs have been performed showing mixed results, 9,10 but these were completed by using the general study populations rather than focusing on a specific subgroup. As such, the aim of this study was to perform an adjusted indirect comparison of rivaroxaban, apixaban, dabigatran 110 and 150 mg BID, and edoxaban 30 and 60 mg QD for the efficacy endpoint of CVA/systemic embolism and the safety endpoint of major, clinically relevant bleeding in women with atrial fibrillation. A secondary aim was to perform the same analysis on the male population with atrial fibrillation to allow for an observation of further potential gender-specific differences in anticoagulant effects.
Methods
The subgroup efficacy endpoint of CVA/systemic embolism in women and major, clinically relevant bleeding in women from the RE-LY, ROCKET-EF, ARISTOTLE, and ENGAGE TIMI AF trials were compared for consistency and comparability by using the Bucher method for adjusted indirect comparison. 11 This method allows an indirect comparison of two variables by using a common comparator. An indirect comparison was performed, because it allows for an evaluation of the relative safety and efficacy of the NOACs with one another, rather than a meta-analysis that would limit their comparison to warfarin as there have been no randomized clinical trials directly comparing NOACs for NVAF.
A formal literature review was not performed. This study was not intended as a systematic review or a meta-analysis, but rather to indirectly compare NOACs for NVAF in men versus women based on high-quality data obtained from rigorous multi-center trials. For this purpose, what we included in the indirect comparison were all major landmark multi-center, phase 3 randomized controlled trials of an NOAC versus warfarin for the purpose of FDA approval of NOACS in NVAF that reported gender-specific outcomes for women and men. Other smaller trials were not included. Gender-specific outcome data were extracted from the final published trials for further analysis. All studies were scored according to Cochrane's risk of bias tool. ARISTOTLE, ROCKET-AF, and ENGAGE AF TIMI had a low risk of bias, as they were double-blinded randomized controlled trials (RCT's) using random number generators. RE-LY scored a high bias risk according to the Cochrane tool, because it was a prospective, open-label trial after the PROBE model. It was included, however, because the PROBE study design has shown no statistically significant difference in endpoint reporting as compared with double-blind RCT's for NOACs. 12
Gender-specific outcome data were extracted from the final published trials for further analysis. A total of 31,508 patients were analyzed. Odds ratios for CVA/systemic embolism and major bleeding were calculated for each NOAC in the aforementioned trials. The odds ratios were compared by using the equation: ORAB = ORAC/ORBC. In this case, A and B represent the two compared NOACs and C represents the common comparator of dose-adjusted warfarin. Confidence intervals were estimated according to Bucher's method as well. First, standard error was calculated according to Altman's practical statistics for medical research. 13 Confidence intervals were obtained by calculating the exponent of the quantity natural log of the odds ratio ±1.96 multiplied by the standard error of the natural log of the odds ratio. These calculations rely on a similarity assumption that ORAC was equally likely to be found if the same trial was performed on the study population from ORBC, meaning that any factors affecting study outcomes are considered similar across the analyzed trails. The aforementioned trials are broadly similar across study designs, with the exception of blinding methodology. 14 The major demographic characteristics again have a high degree of similarity, with the exception of elevated CHADS2 score in the ROCKET-AF trial. Full study characteristics are presented in Table 1. The analysis was applied to indirectly compare rivaroxaban, apixaban, dabigatran 110 and 150 mg BID, and edoxaban 30 and 60 mg QD. Forest plots were generated from the analyzed data by using MedCalc statistics software. Gender-specific data for major bleeding were not provided for dabigatran 110 and 150 mg BID, so they were not included in the safety endpoint analysis.
CVA, cerebrovascular accident; DM, diabetes mellitus; HTN, hypertension; LVEF, left ventricular ejection fraction; NOAC, novel oral anticoagulant; SBP, systolic blood pressure; TIA, transient ischemic attack.
Results
No statistically significant differences were demonstrated for any one NOAC compared with alternatives in terms of safety or efficacy in female or male patients. Comparisons of odds ratios alone in dabigatran 150 mg BID resulted in odds ratios of less than 1 compared with alternative NOACS in both gender groups. Edoxaban 30 mg had odds ratios of less than 1 for major bleeding, but greater than 1 for stroke/systemic embolism in both men and women. Comparative NOAC efficacy for women with associated 95% confidence intervals is displayed in Figures 1
–6, and comparative safety data are depicted in Figures 7
–10. Raw data used to generate the forest plots are presented in the Supplementary Data; Supplementary Data are available online at
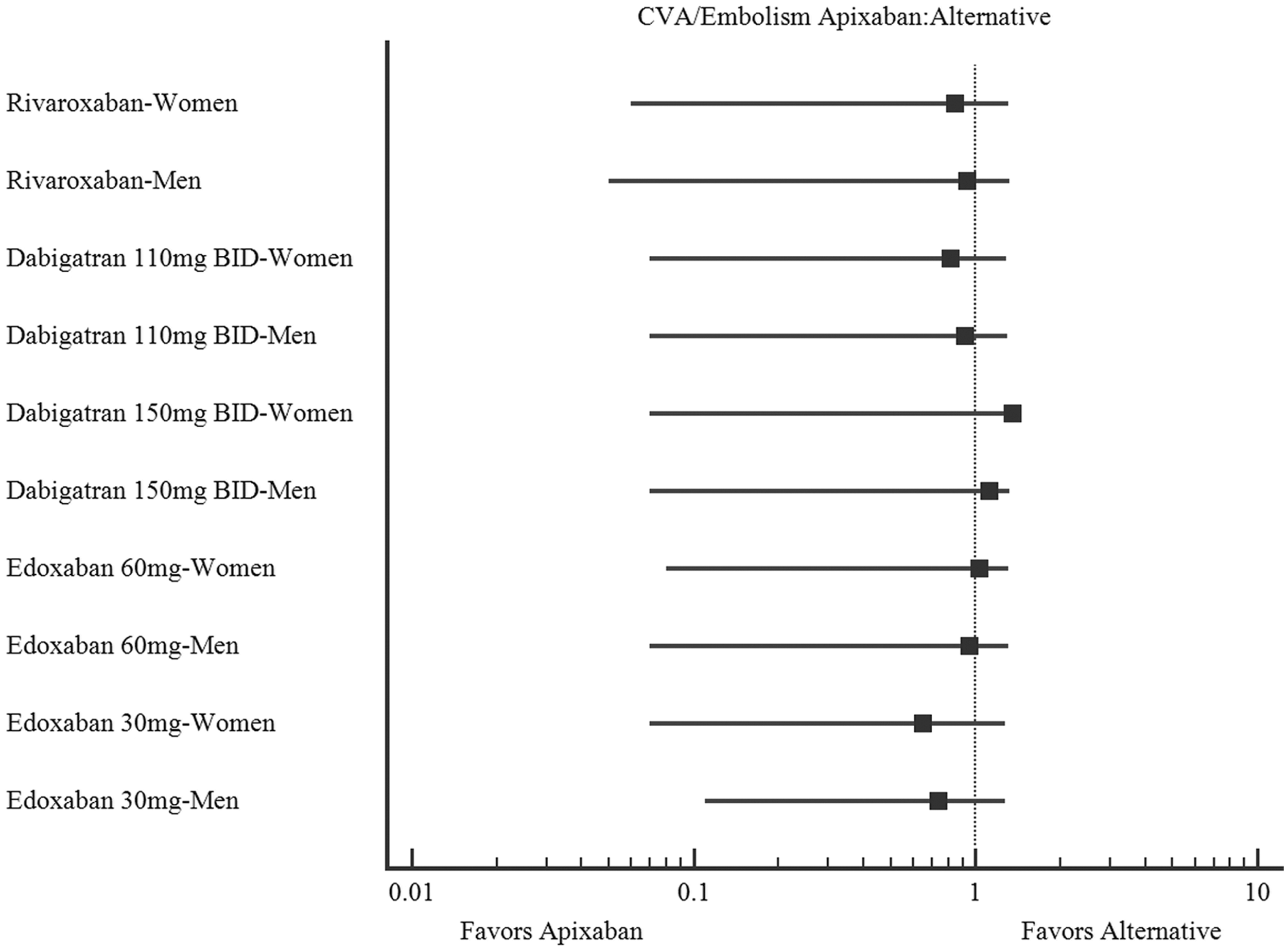
Comparative apixaban efficacy.
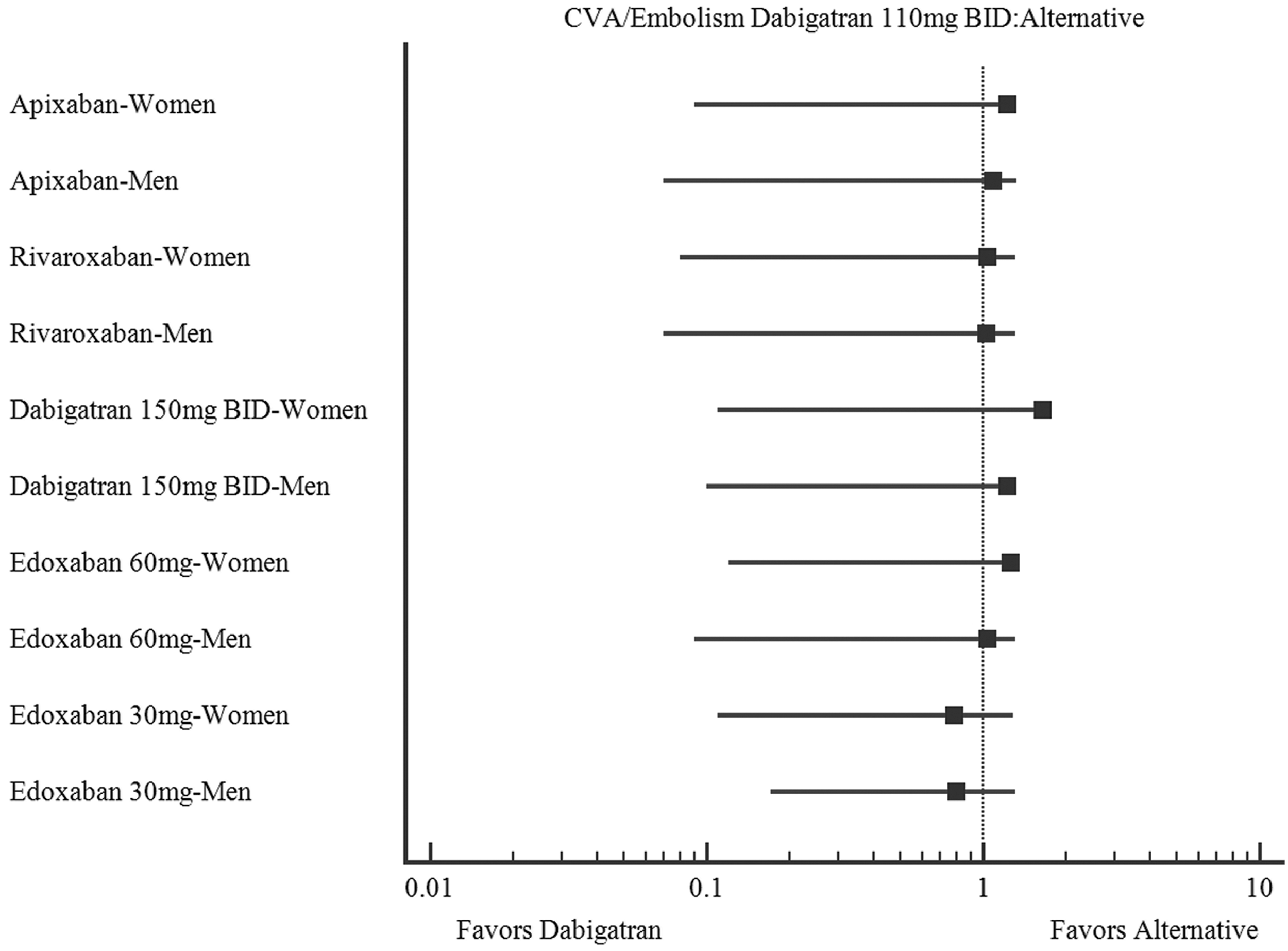
Comparative dabigatran 110 mg efficacy.
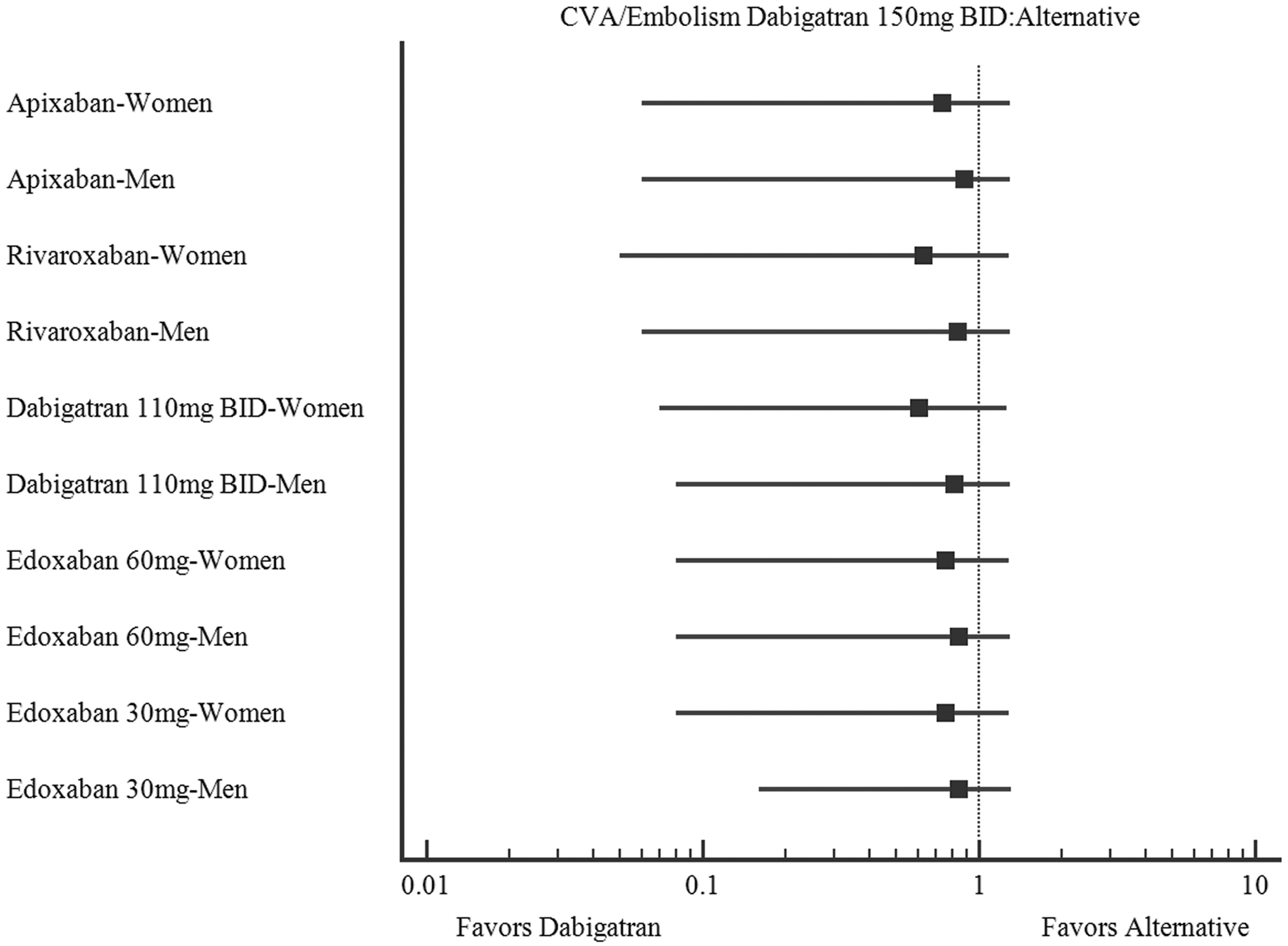
Comparative dabigatran 150 mg efficacy.
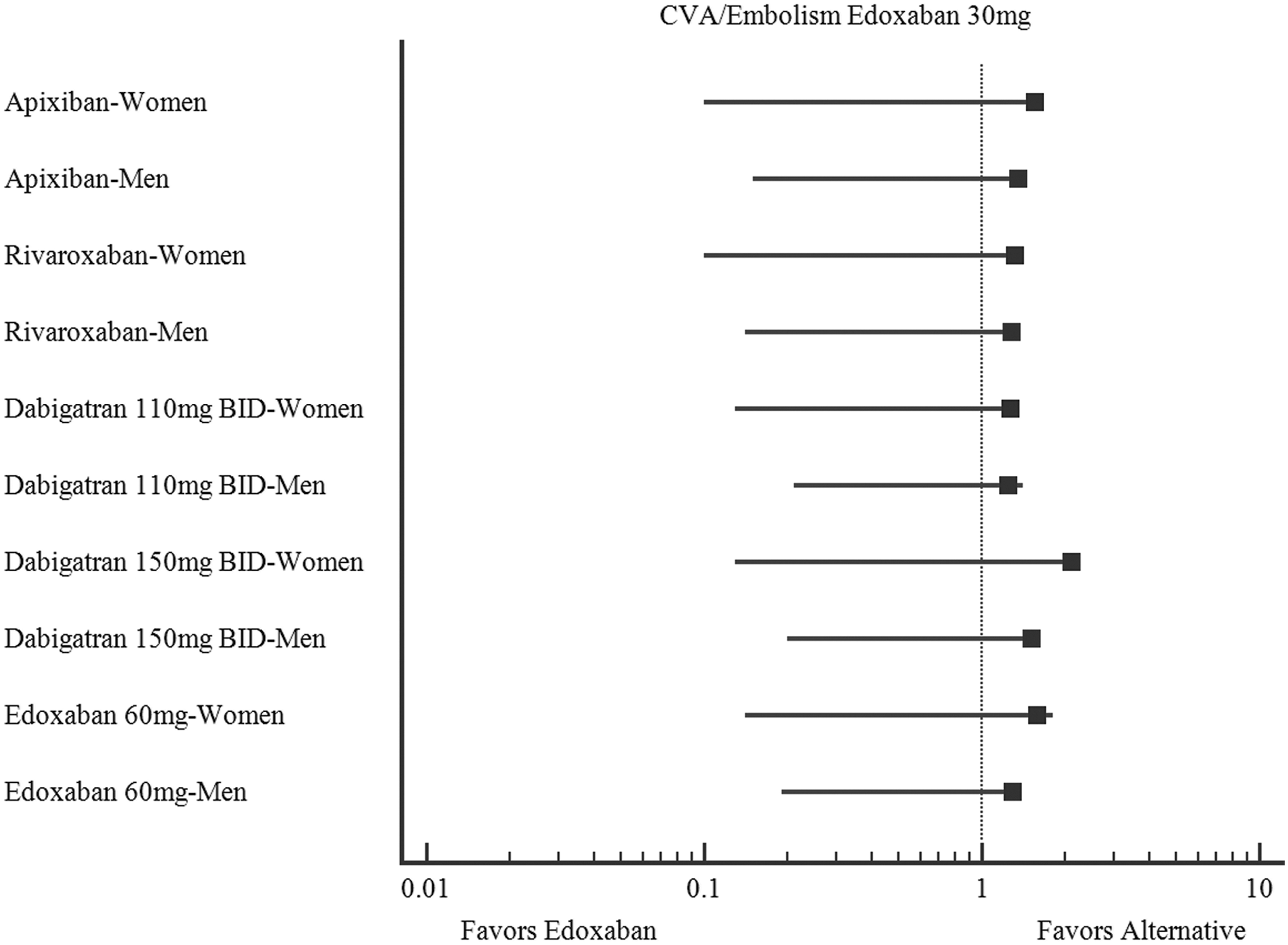
Comparative edoxaban 30 mg efficacy.
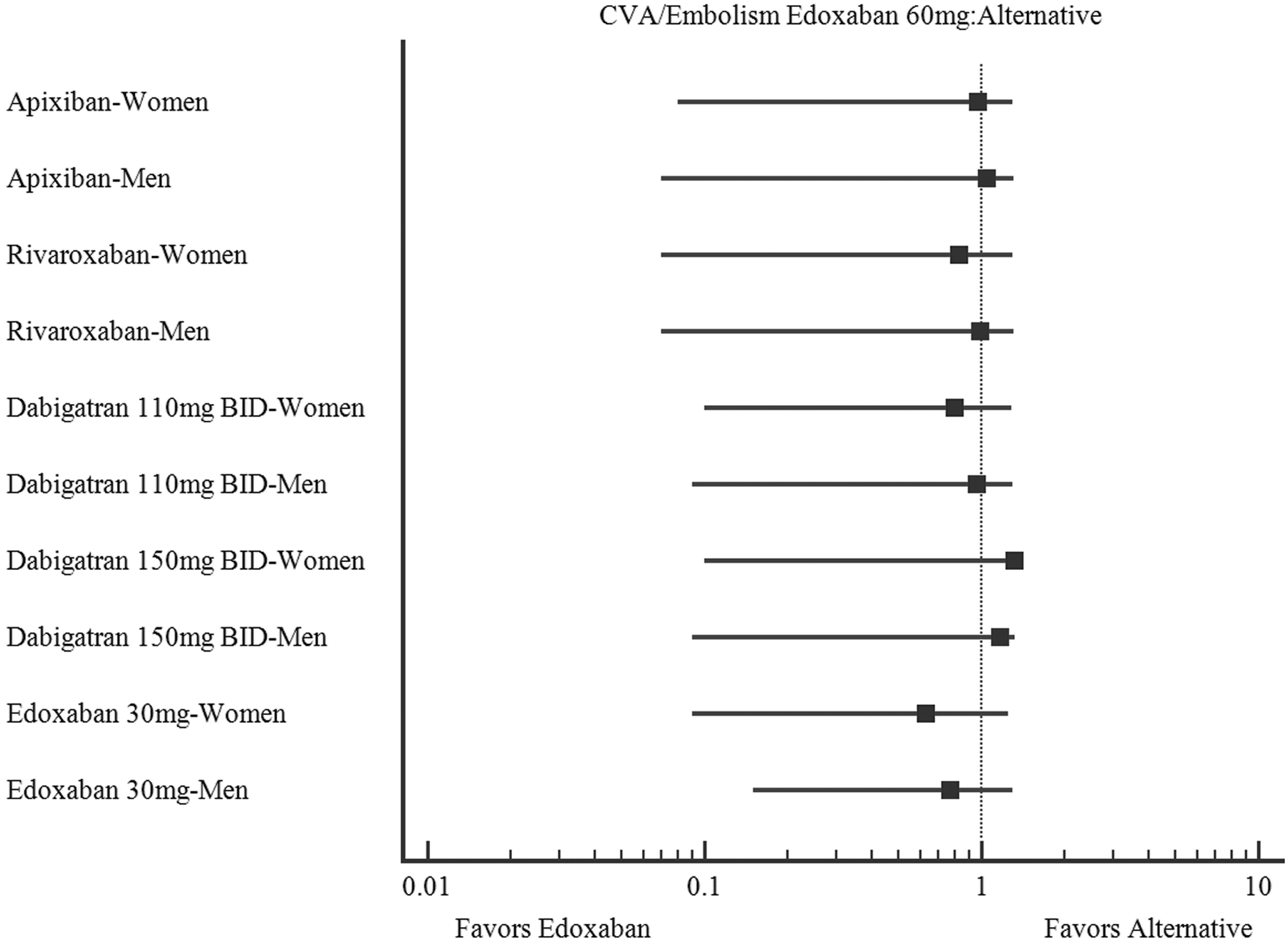
Comparative edoxaban 60 mg efficacy.
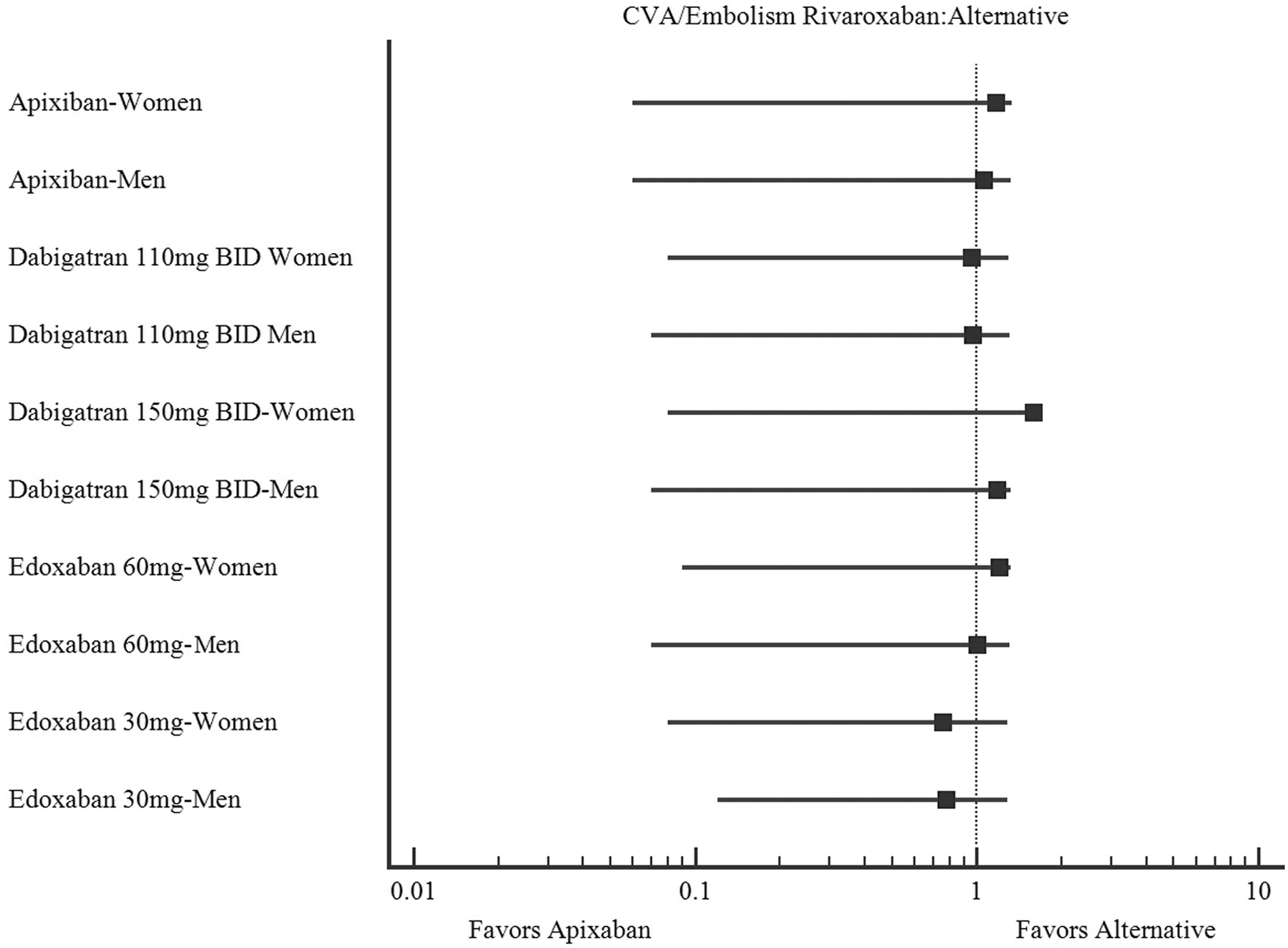
Comparative rivaroxaban efficacy.
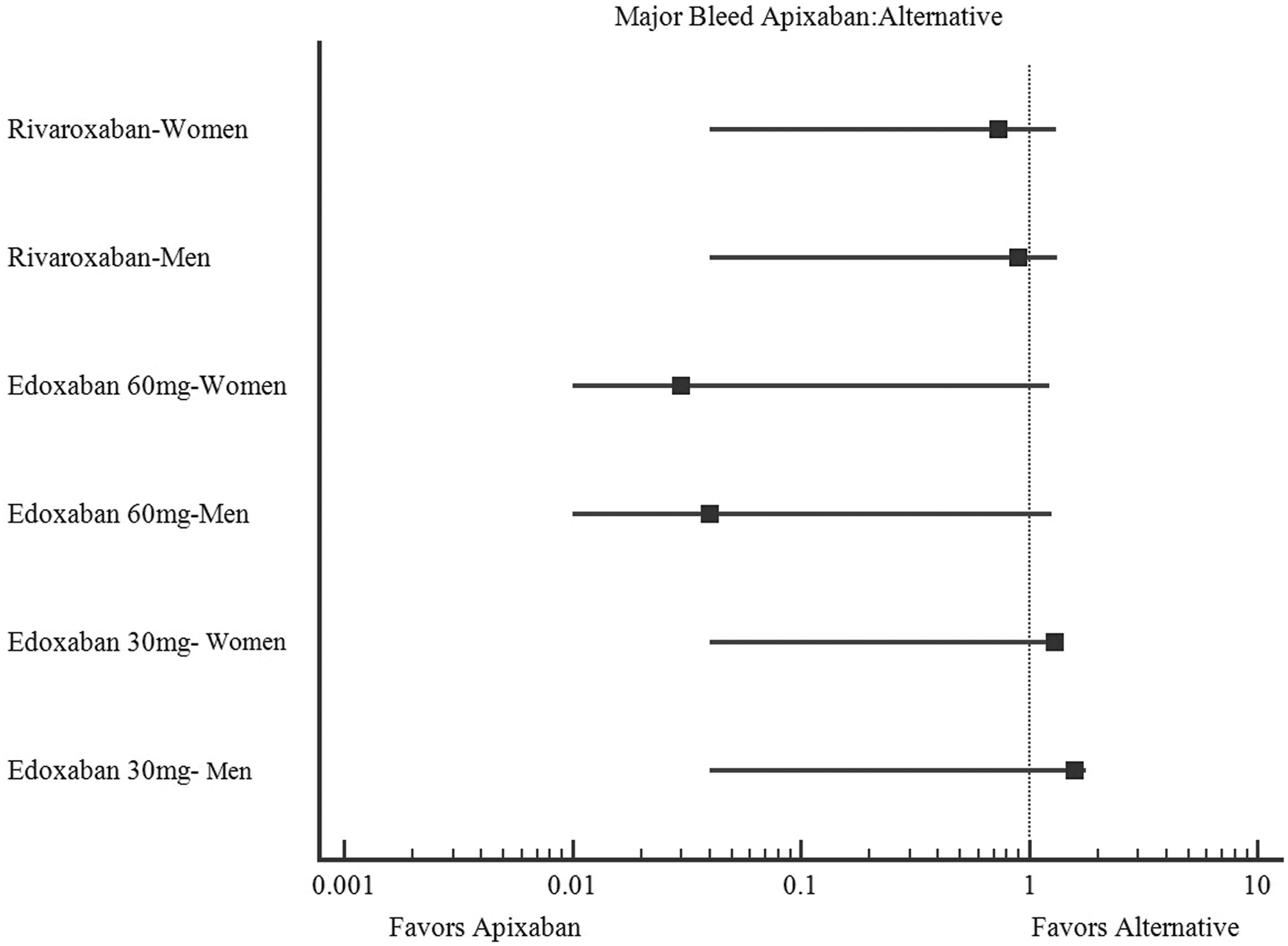
Comparative apixaban safety.
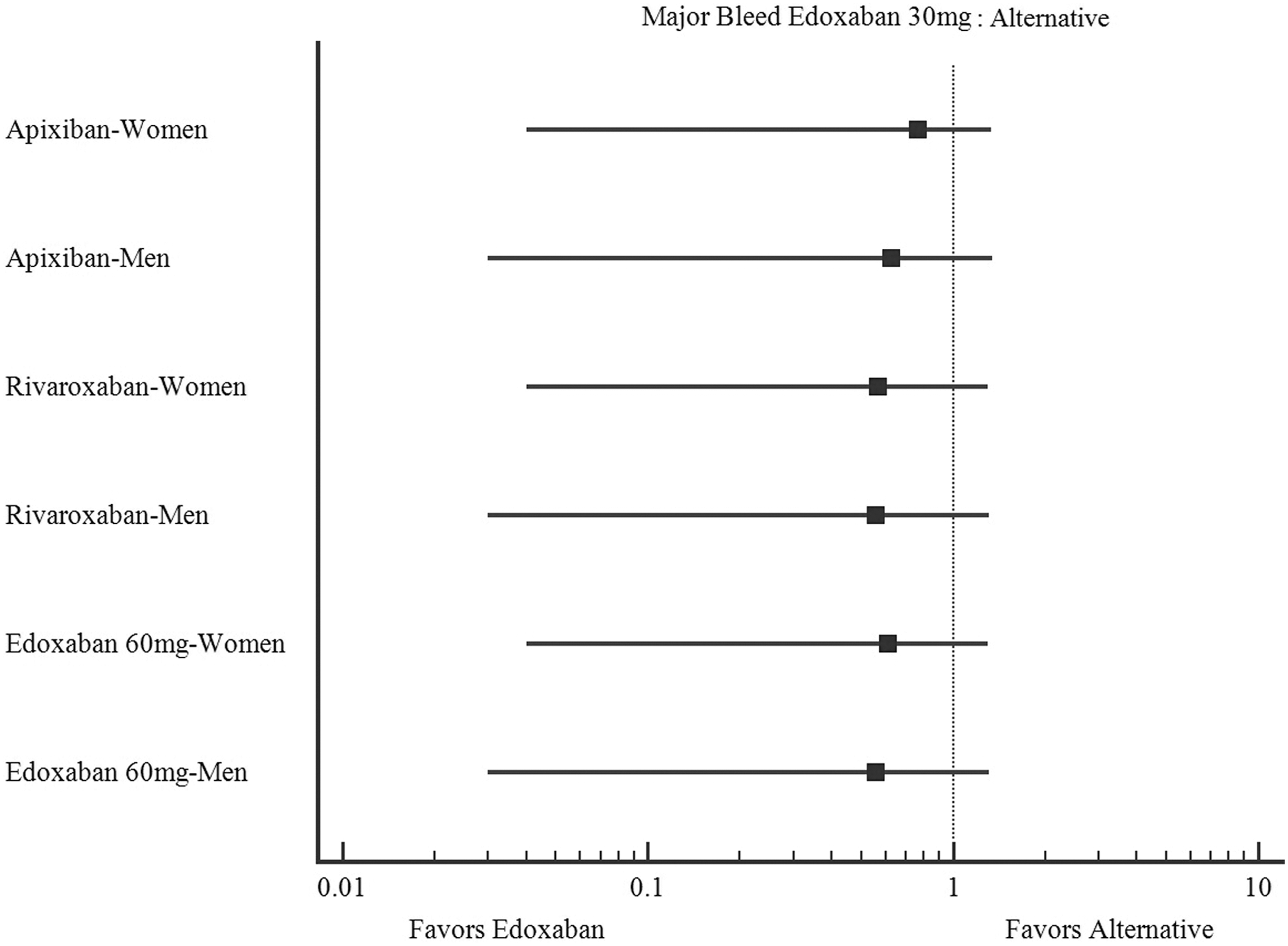
Comparative edoxaban 30 mg safety.
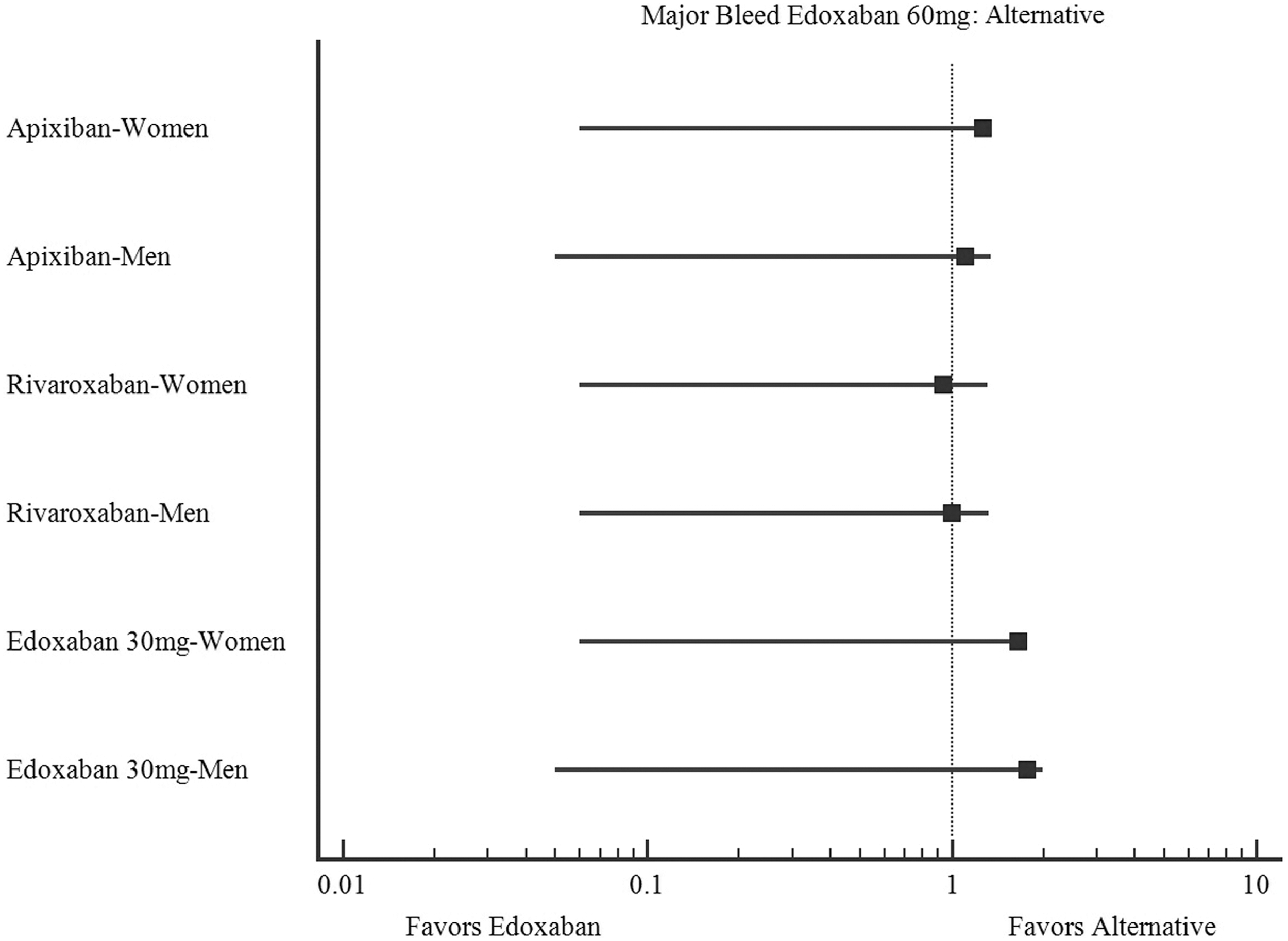
Comparative edoxaban 60 mg safety.
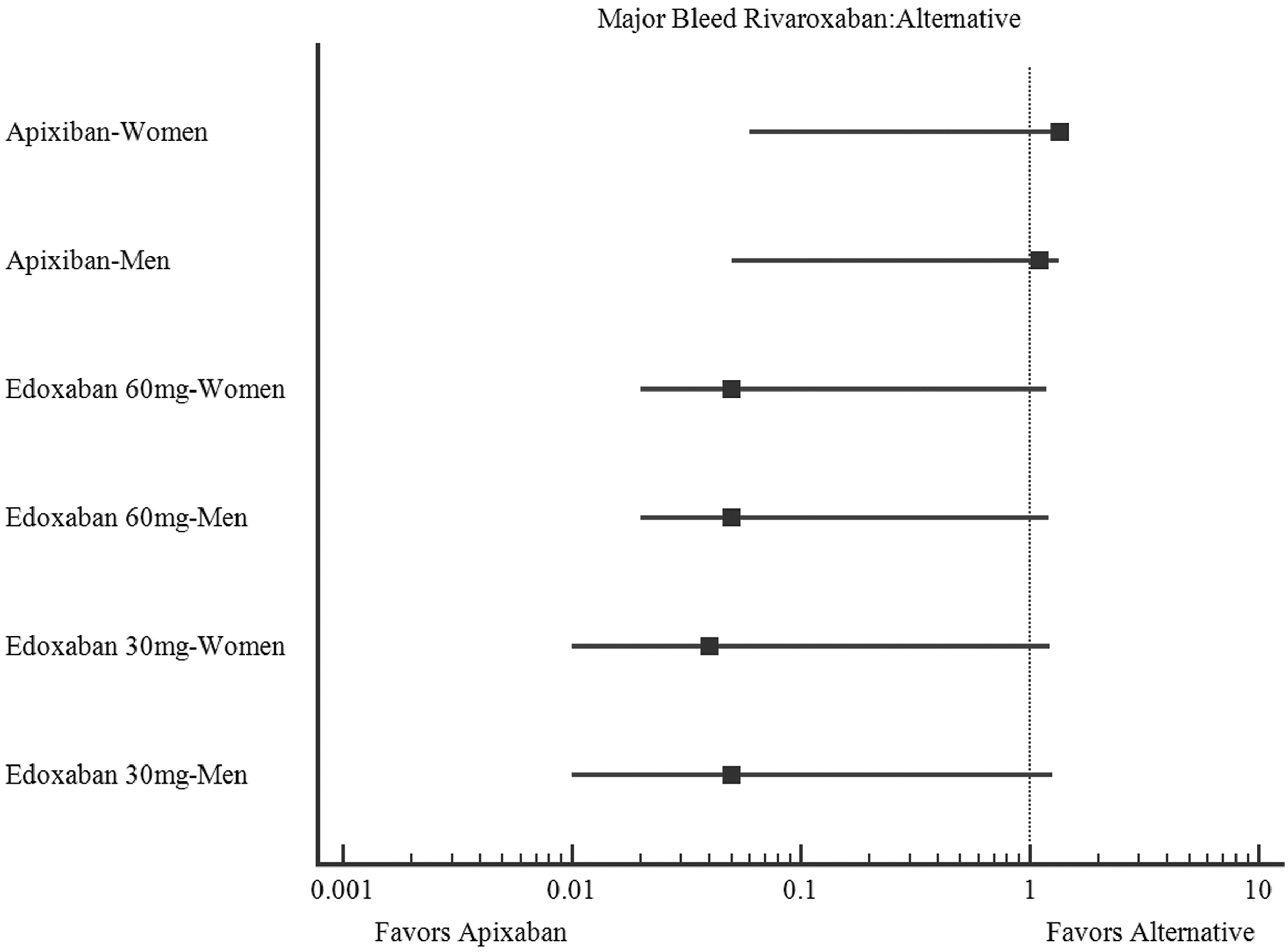
Comparative rivaroxaban safety.
Discussion
Prior meta-analyses on NOAC gender differences have been performed with mixed results based on the indication examined. The inspiration for this indirect comparison was a published meta-analysis on gender differences in NVAF treated with NOACs or warfarin, which showed that both sexes had a decreased stroke risk with NOACs as compared with warfarin, and no significant difference in bleeding risk. When the data were examined in gender subgroups, women treated with any NOAC demonstrated a lower risk of both stroke and bleeding than their male counterparts. 8 A meta-analysis of gender differences in NOACs and warfarin in patients with venous thromboembolism showed no significant difference in recurrent venous thromboembolism between genders. Women demonstrated a statistically significant increase in major bleeding events when treated with any NOAC compared with men. 9 These meta-analyses allowed for comparisons of NOACs as a group to warfarin, but could not draw any conclusion about the effect of the NOACs compared with one another. As such, the objective was to statistically compare NOACs with one another, specifically in men and women with NVAF to evaluate whether the differences reported in the prior meta-analyses could be attributed to any individual NOAC. According to our adjusted indirect comparison of efficacy and safety of NOACS in men and women for CVA/systemic embolism and major bleed risk, there were no statistically significant differences demonstrated for any one NOAC when compared with the other with respect to safety or efficacy in either gender. Although the data analysis indicated no statistically significant differences, observation of odds ratios alone demonstrates several areas for potential further investigation through direct head-to-head comparisons of NOACs.
The odds ratios for dabigatran 150 mg BID in both men's and women's CVA/systemic embolism are all less than 1, indicating a potential favorable efficacy profile. Unfortunately, no major bleeding data for gender subgroups were available from the RE-LY trial, so no comment, observational or statistical, can be made on its sex-specific safety profile. Edoxaban 30 mg, meanwhile, had odds ratios greater than 1 for efficacy outcomes, but less than 1 for safety outcomes in both men and women, showing a mixed picture of possible decreased efficacy but improved safety profile to alternative NOACs. In side-by-side observations of the remaining Forest plots, there do not appear to be differences in safety or efficacy for any single agent for women as compared with men.
One reason that warfarin continues to be used instead of NOACs despite their safety and efficacy profiles is the availability of reversal agents. Very recently, a reversal agent was approved for dabigatran and a reversal agent for the direct factor Xa inhibitors is undergoing evaluation at the time of writing. The existence of reversal agents for NOACs makes them increasingly a safe choice.
The observed trends in odds ratios mentioned earlier provide a point of investigation for direct comparisons of NOACS in women. Such a comparison would require a very large patient population to find statistically significant differences in NOAC efficacy and safety in women. The potential observed effects are very small and likely clinically negligible. As such, our analysis indicates that the NOACs examined may be used interchangeably in women with atrial fibrillation due to highly similar safety and efficacy profiles. These findings mean that ease of dosing, affordability, side-effect profile, kidney function, and individual patient preference should guide NOAC choice. Considering those factors will lead to drug choices to which women with atrial fibrillation will remain adherent, so that they are safely and effectively anti-coagulated.
Limitations
Limitations of this comparison include slight differences in compared patient populations, but as previously discussed and presented in Table 1, and discussed in the methods section, the trials used in the indirect comparison have a high degree of similarity. This is a known issue of indirect comparisons. 14 Selection of only large trials with as many common endpoint and population characteristics as possible was performed to minimize this effect. All the included studies used stroke or systemic embolism for primary efficacy endpoints and major bleeding as defined by International Society for Thrombosis and Hemostasis criteria as their primary safety endpoint, allowing for a reliable data comparison. 15,16
Conclusion
No statistically significant differences in NOAC efficacy and safety could be detected in the female or male subgroups, but observation of odds ratios alone does reveal possible favorable efficacy in dabigatran 150 mg BID and unfavorable efficacy in edoxaban 30 mg, but favorable safety. A comparison of the women's and men's forest plots did not reveal any trends in safety or efficacy for specific agents. NOACs should be used interchangeably in women with atrial fibrillation according to patient preferences, affordability, ease of dosing, and side-effect profile to achieve the best possible medication adherence.
Footnotes
Author Disclosure Statement
R.D. serves on the Advisory Board for Astellas Pharma and receives research funding from Astellas Pharma (not relevant to this work). A.K.J. has served as a consultant for Boehringer Ingelheim, Janssen, Medtronic, and BMS. Other authors have no conflicts to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.