
Abstract
Objectives:
To inform the development of HIV care strategies for older women with HIV infection, an understudied group, we compared the psychosocial, behavioral, and clinical characteristics of HIV-positive women aged ≥50 (older women) with those aged 18–49 (younger women).
Methods:
We examined factors among HIV-positive women in care using data from the 2009 through 2013 cycles of a nationally representative sample of HIV-positive adults in care (Medical Monitoring Project). We compared psychosocial, clinical, and behavioral factors among women aged ≥50 years at interview versus those aged <50 years. We calculated weighted frequency estimates and performed logistic regression to compute adjusted prevalence ratios (aPR) and 95% confidence intervals (CIs) for the comparison of characteristics among women aged ≥50 versus <50 years.
Results:
Of 22,145 participants, 6186 were women; 40.7% (CI 39.1–42.3) were ≥50 years, and 32.7% of older women reported being sexually active. Compared with women <50 years, women aged ≥50 years were more likely to be dose adherent (aPR = 1.19; CI 1.07–1.33), prescribed antiretroviral therapy and have sustained viral load suppression (aPR = 1.03; CI 1.00–1.18), and were less likely to report any depression (aPR = 0.92; CI 0.86–0.99), to report condomless sex with a negative or unknown partner if sexually active (aPR = 0.56; CI 0.48–0.67), and to have received HIV/sexually transmitted infection (STI) prevention counseling from a healthcare provider (aPR = 0.82; CI 0.76–0.88).
Conclusions:
These data suggest that older women in HIV care have more favorable outcomes in some clinical areas, but may warrant increased HIV/STI prevention counseling from their care providers, especially if sexually active.
Introduction
L
By the end of 2013, of all persons ≥50 years of age living with diagnosed HIV infection in the United States, women comprised 22.5%. 5 Women comprised 26.5% of all persons aged 50 years and older diagnosed with HIV in 2014. 5 For HIV-positive women taking effective ART, longer life expectancy means many women are living well into their postmenopausal years and require tailored, comprehensive medical care and treatment.
To date, several reports have described the natural history, prevalence, and treatment response of menopausal symptoms among older women living with HIV infection. 6 –9 However, little is known about general factors associated with aging among HIV-positive women compared with younger HIV-positive women, and how to tailor HIV care and support more specifically for older women. 10,11 We compared the social, behavioral, and clinical characteristics of HIV-positive women ≥50 years of age (older women) with those aged 18–49 years (younger women) from a nationally representative sample of HIV-positive persons receiving care. Understanding the differences among these women by age groups may inform the development of HIV prevention and care strategies that are relevant and effective for older women with HIV infection.
Methods
Data and study design
We analyzed matched interview and medical record abstraction data from the 2009 through 2013 data collection cycles of the Medical Monitoring Project (MMP). MMP is an HIV surveillance system that provides annual, nationally representative estimates of behavioral and clinical characteristics of HIV-positive adults receiving medical care in the United States. MMP used a probability proportionate to size sampling design; the MMP sample was selected in three stages.
During the 2009 through 2013 data cycles, U.S. states and territories were sampled, followed by providers at outpatient facilities providing HIV care, and finally by HIV-infected adults aged 18 years and older who reported at least one medical care visit in a participating facility during January through April of each data cycle. For state and territory samples, the probability of selection was proportionate to AIDS prevalence; for provider samples, the probability of selection was proportionate to the HIV-infected patient census. 12 –16 Data were collected via face to face interviews and medical record abstractions for HIV positive and age 18 years or older, and had received medical care in participating facilities between January and April in the cycle year for which they were sampled. * All sampled states and territories participated in MMP.
Each participant's record was weighted to account for known probabilities of selection for each state or territory, by facility, and for patients from selected facilities. In addition, using information collected from sampled facilities and sampled patients, we completed an analysis to compare respondents and nonrespondents. Data were also weighted to adjust for nonresponse using predictors of patient-level response (e.g., facility size, facility type [public or private], participant race or ethnicity, time since HIV diagnosis, and age group). 13,14
The number of participating facilities ranged from 461 to 480 (median = 473) from the 2009 to 2013 data cycles. Of sampled patients, the number of patients who completed interviews and had their medical record abstracted ranged from 4217 to 5030 (median = 4503). The median facility response and patient response rates, adjusted for eligibility, ranged from 76% to 85% (median = 83%) and from 52% to 56% (median = 55%).
Analysis criteria
We combined data from the MMP 2009–2013 data collection cycles (n = 22,145); then, we restricted our analyses to women, who represented 26%–28% of all participants over the years (n = 6186). The analysis sample was stratified into two groups: women aged ≥50 years (older women) and women aged 18–49 years (younger women) at the time of interview.
Measures
Demographic, social, and behavioral variables
Sociodemographic variables collected for the MMP analyses included race/ethnicity (white non-Hispanic, black non-Hispanic, Hispanic, or other); education attainment (<high school, high school diploma, or >high school); length of time since HIV diagnosis (<5, 5–9, ≥10 years); and poverty level (at or below, above). The following social and behavioral variables were reported by respondents based on the 12 months before being interviewed: incarceration, homelessness, type of healthcare coverage, smoking, drug use (both injection and noninjection) for nonmedical purposes, any sexual activity, and any condomless sex with a negative or unknown status partner. Binge drinking in the 30 days before being interviewed was defined as four or more drinks per day for women. Any depression in the past 2 weeks, based on the eight-item Patient Health Questionnaire Depression Scale (PHQ-8), was defined as a score of ≥10. 17 The number and percentage of participants meeting current poverty guidelines were determined using the U.S. Department of Health and Human Services poverty guidelines 18 that corresponded to the calendar year about which the combined household income was asked. The HIV disease stage as per Centers for Disease Control and Prevention (CDC) criteria, Stage 1, no AIDS and nadir CD4+ T lymphocyte (CD4) ≥0.500 × 109 cells/L (or CD4% ≥29); Stage 2, no AIDS and nadir CD4 0.200–0.499 × 109 cells/L (or CD4% 14 to <29); or Stage 3, AIDS or nadir CD4 count 0–0.199 × 109 cells/L [or CD4% <14], was determined. 19
Clinical care and treatment indicators
Clinical variables were abstracted from participants' medical records for the year before the MMP interview and included the following: documented prescription of ART, geometric mean CD4 count (0–199, 200–499, or ≥500 cells/mm3), most recent HIV RNA viral load suppression (defined as most recent viral load documented as undetectable or <200 copies/mL), sustained viral suppression (defined as all viral loads in the past 12 months as undetectable or <200 copies/mL), medical record documentation of results from a Pap test, and testing for gonorrhea, chlamydia, or syphilis. Using the interview instrument, participants reported if they were currently taking ART and if they were taking ART, their ART medication taking behaviors, and if they had received HIV and sexually transmitted infection (STI) prevention counseling by a health professional in the past year. If the participant reported that they took the prescribed dose of ART medications in the 3 days before interview, they were classified as 100% dose adherent (hereafter referred to as “dose adherent”).
Data analyses
Weighted estimates of percentages and associated 95% confidence intervals (CIs) were computed to describe the characteristics of HIV-positive women aged ≥50 versus <50 years. Bivariate associations between the selected independent variables and younger and older women were tested using the Rao–Scott chi-square tests. 20
We performed logistic regression to compute unadjusted and adjusted prevalence ratios (aPR) and 95% CIs for the association between psychosocial, behavioral, and clinical factors with being aged ≥50 versus <50 years. All characteristics with a p-value <0.05 were retained in the final multivariate logistic model. We also identified and included strong social determinants in the model and assessed differences between younger and older women. For all variables in the model, we computed adjusted prevalence estimates (predicted marginal percentages) and prevalence ratios, with 95% CIs among all levels of each characteristic associated with younger and older HIV-positive women, using multiple logistic regression analysis after controlling for the selected characteristics. 21,22
All analyses were performed using SAS 9.3 (SAS Institute, Cary, NC) and SAS-callable SUDAAN 10.0.1 (RTI International, Research Triangle Park, NC), and accounted for clustering, unequal selection probabilities, and nonresponse.
Ethics statement
In accordance with guidelines for defining public health research, 23 CDC-determined MMP was public health surveillance used for disease control, program, or policy purposes. Local institutional review board approval was obtained at participating states, territory, and facilities when required. Informed consent was obtained from all interviewed participants.
Results
In 2009–2013 MMP data cycles, women represented 26.4% of the sample (Table 1). Among HIV-positive women in care, 40.7% were aged ≥50 years, 60.5% were non-Hispanic black, and 64.6% were at or below poverty level. Also, 27.2% reported any depression in the previous 2 weeks, 67.2% of participants had Stage 3 disease (clinical or immunologic AIDS), 51.5% were sexually active, 12.0% reported condomless sex with an HIV-negative or unknown HIV status partner, and 39.3% were current smokers.
Time period: in the past 12 months, unless otherwise noted. All measures are self-reported unless otherwise noted.
Weighted column percentage.
Hispanics or Latinos can be of any race.
Any depression in the past 2 weeks, based on the PHQ-8, defined as a score of ≥10.
Based on medical record abstraction data in the past 12 months before interview.
The stages are as follows: Stage 1, no AIDS and nadir CD4 ≥ 500 copies/mL or CD4% ≥ 29; Stage 2, no AIDS and nadir CD4 between 200 and 499 copies/mL or CD4% 14–29; Stage 3, AIDS or nadir CD4 between 0 and 199 copies/mL or CD4% <14%.
Dose adherent (or 100% dose adherent) refers to taking a dose or set of pills/spoonfuls/injections of ART medications as prescribed by the medical provider over the past 3 days.
Sustained viral suppression is defined as all viral loads in the last 12 months undetectable or <200 copies/mL.
Chi-square p-value based on the Rao–Scott chi-square.
ART, antiretroviral therapy; CI, confidence interval; n, unweighted sample size; PHQ-8, eight-item Patient Health Questionnaire Depression Scale; STI, sexually transmitted infection; VL, viral load.
By age group, there were significant differences (p < 0.05) in length of time since HIV diagnosis, type of health insurance coverage, poverty level, recent history of homelessness or incarceration, recent depression, sexual activity, binge drinking, any drug use, HIV disease stage, being prescribed ART, currently taking ART, dose adherence, viral suppression, mean CD4 count, having received STI prevention counseling by a healthcare professional, and having received a Pap test (Table 1).
In bivariate analysis, compared with women aged <50 years, women aged ≥50 years were significantly (p < 0.05) more likely to be dose adherent for the past 3 days, prescribed ART and be virally suppressed for the previous 12 months than not to be prescribed ART, and they were less likely to be uninsured or have Ryan White coverage only (hereafter referred to as “no insurance”). They were also less likely to be at or below household poverty level, homeless, or incarcerated. They were less likely to report symptoms consistent with depression and were less likely to have a Pap test documented in the medical chart. Detailed crude prevalence ratios are summarized in Table 2.
Time period: in the past 12 months, unless otherwise noted. All measures are self-reported unless otherwise noted.
Based on medical record abstraction data in the past 12 months before interview.
Any depression in the past 2 weeks, based on the PHQ-8, defined as a score of ≥10.
Sustained viral suppression is defined as all viral loads in the last 12 months undetectable or <200 copies/mL.
Dose adherent (or 100% dose adherent) refers to taking a dose or set of pills/spoonfuls/injections of ART medications as prescribed by the medical provider over the past 3 days.
aPR, adjusted prevalence ratio (adjusted for all other factors in the model); n, unweighted sample size; PR, unadjusted prevalence ratio.
In multivariable analyses, compared with women <50 years of age, women aged ≥50 years were more likely to have been diagnosed with HIV longer (≥10 versus <5 years ago [aPR = 1.44]) and to have been prescribed ART and have sustained viral load suppression (aPR = 1.03) than to not have been prescribed ART and to be dose adherent the past 3 days (aPR = 1.19). They were less likely to have private insurance (aPR = 0.81) or no insurance versus public insurance (aPR = 0.53), to be at or below the household poverty level (aPR = 0.84), to have a history of incarceration (aPR = 0.66), to report symptoms consistent with depression in the previous 2 weeks (aPR = 0.92), to report condomless sex with an HIV-negative or unknown partner (aPR = 0.56), to have a Pap test result documented in their medical chart (aPR = 0.87), and to have received HIV/STI prevention counseling from a healthcare provider (aPR = 0.82). Detailed aPR are summarized in Table 2.
Furthermore, three levels of ART prescription and viral suppression—prescribed ART with sustained viral suppression, prescribed ART without sustained viral suppression, and not prescribed ART, were examined. We compared the percentages for those younger than 50 years compared to those older than 50 years in each of the three levels. We found that older women were more likely to have been prescribed ART and also have sustained viral load suppression than women <50 years of age, while younger women were less likely to have been prescribed ART (Fig. 1).
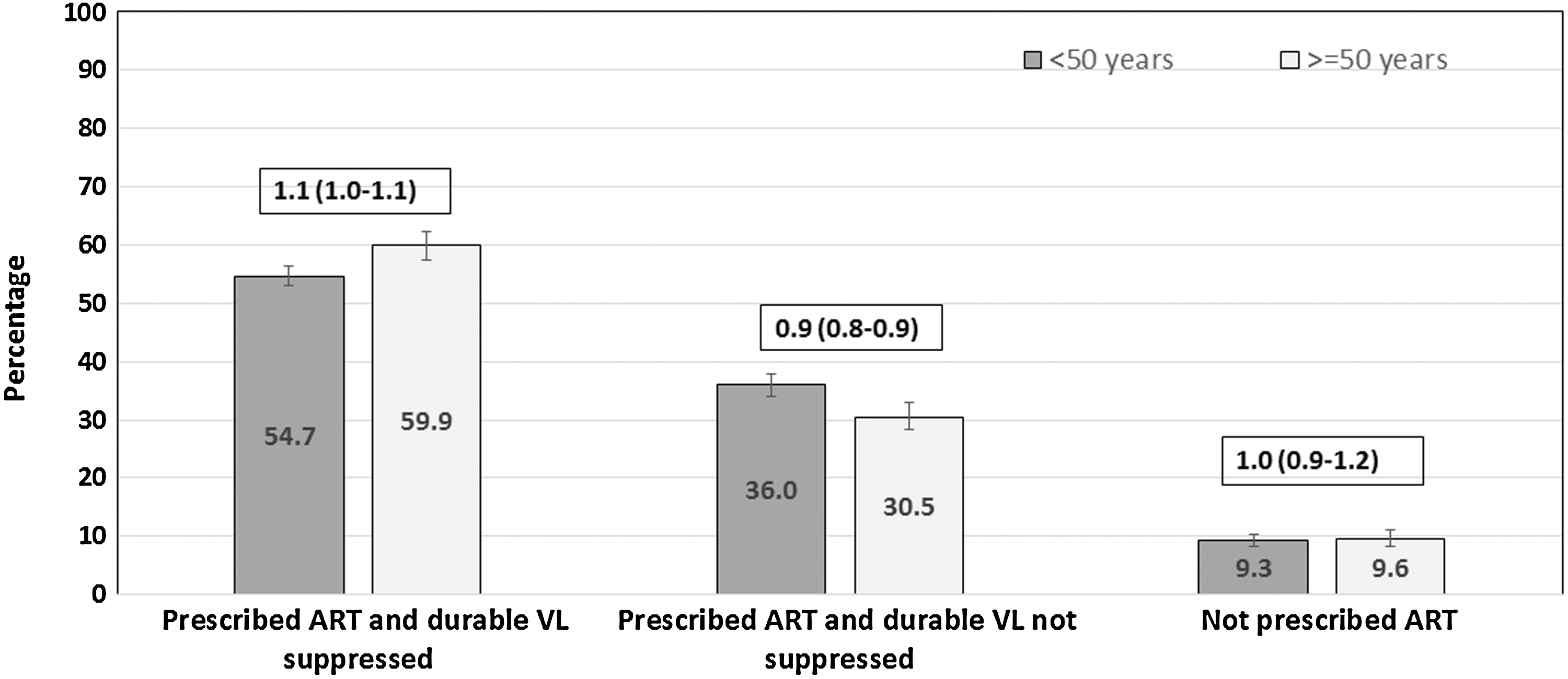
Percentage of ART prescription and durable viral suppression among older and younger women, MMP, 2009–2013. Numbers in boxes are adjusted prevalence ratios and 95% confidence intervals comparing selected characteristics between older (≥50 years) and younger (<50 years) HIV-infected women in MMP. The prevalences and prevalence ratios are based on the results from the multivariate model in Table 2. ART, antiretroviral therapy; MMP, Medical Monitoring Project; VL, viral load.
Discussion
Among HIV-positive women in care from 2009 to 2013, differences between older women and younger women suggest that older women fared better on several indicators of social determinants of health, such as having healthcare insurance and less poverty. Older women also had more favorable HIV clinical status, as they were more likely to be prescribed ART, be dose adherent, and have sustained viral suppression.
In terms of HIV sexual risk behaviors, older HIV-positive women also differed from their younger counterparts. Compared to younger women, older women were less likely to be sexually active and were less likely to report condomless sex with a male partner. However, for older women who were sexually active or engaged in risk behaviors, sexual health and behavioral issues may not always be adequately addressed. Older HIV-positive women who were sexually active were less likely than their younger counterparts to be screened for gonorrhea, chlamydia, and syphilis, and only 42% of women older than 50 years reported receiving HIV/STI prevention counseling by their healthcare providers. Previous studies have documented that providers underestimate sexual activity by older patients. 24,25 Providers may need reinforced messages regarding the continued importance of sexual risk-reduction messages for older patients living with HIV. 24,26
Reinforced messages regarding routine health screenings for HIV-positive women, in general, may also be needed. Based on our results, routine STI and Pap testing among all sexually active HIV-positive women—regardless of age—was suboptimal (<40% for Pap, gonorrhea, or chlamydia screening and <53% for syphilis screening) in outpatient HIV clinical care settings. Clinical guidelines recommend annual screening for gonorrhea, chlamydia, and syphilis among persons who are sexually active. 27 Annual Pap tests are also recommended for women who are living with HIV, although more recent evidence suggests that increasing time between Pap tests may be warranted in cases where multiple negative results are obtained. 28 HIV care interventions that strengthen routine STI clinical screenings for women by providers may be warranted.
We also found that older women were more likely than younger women to have a suppressed viral load, as measured by either most recent viral load or all viral loads over the past 12 months. In addition, a larger proportion of older women (72.9%) had Stage 3 HIV disease stage compared with 63.3% of younger women, which perhaps reflects the fact that a higher proportion of older women in our sample had lived with HIV for ≥10 years and had more time to have an AIDS-defining diagnosis at some point. Nevertheless, viral suppression among women overall appears to be suboptimal, with 71.5% of the women in our sample achieving viral suppression at their most recent viral load; this is below the national target of viral suppression for 80% of all HIV-positive persons. Lack of viral suppression is associated with increased risks for ongoing HIV transmission. Data suggest that many women living with HIV are especially affected by social and structural barriers that create challenges to care, including poverty, lack of access, and community and individual stigma. 29 –31 In addition, these findings suggest the need for increased, targeted delivery of healthcare services and HIV/STI counseling services for older women. These challenges must be addressed and considered in the development of social and structural interventions that strengthen retention in care and adherence to ART medications for women.
In addition to social and structural barriers, poor mental health, which may affect treatment adherence and health-related behaviors, is a concern among individuals living with HIV infection. 32 Our estimated prevalence of 27% for recent depression among HIV-positive women in care appears to be more than twice as high as that observed among women in the general population, 33 and is consistent with previous findings on depression among HIV-positive persons. 34 Symptoms consistent with any depression were less frequently reported by older than younger women in our study, and depression has been linked to a decreased likelihood of viral suppression. 35 Given the common occurrence of depression among HIV-infected persons, routine screening and monitoring for depression are an integral part of clinical HIV management, particularly in the context of treatment of nonadherence and unsuppressed viral load.
While some signs are positive for older women compared with younger women, the high prevalence of certain behaviors for all women warrants that public health efforts with women remain and get stronger. For example, overall, 12% of sexually active women in our sample reported condomless sex with an HIV-negative or unknown status male partner, which suggests multiple opportunities for sexual HIV transmission; stronger messages regarding use of condoms and availability of pre-exposure prophylaxis for uninfected partners 36 are warranted with both older and younger women. Another example is current smoking, which was reported by 39% of women in our sample with no differences by age group; this prevalence and the increased morbidity and mortality due to smoking among persons living with HIV 37 highlight the need to address smoking among women living with HIV. Smoking cessation remains an important public health goal to reduce both HIV and non-HIV-related morbidity and mortality, and should be discussed as a goal at each clinical encounter. 38,39
Limitations
This analysis was subject to some limitations. First, data are limited to HIV-positive women receiving care, not all HIV-positive women. Thus, the findings of this study cannot be generalized to HIV-positive women not receiving medical care. Second, there may be possible survivor bias among older women, as those available to participate may have additional behaviors that contributed to current HIV control and overall healthcare. Our data show that older women were more likely to be prescribed ART, be dose adherent, and be virally suppressed than younger women. More work is needed to better understand the differential prevalence of ART prescription and viral suppression to guide care for women by younger and older age groups. Third, for some variables, such as STI counseling, medical record documentation would provide more reliable data than patient report; future reports should strengthen medical records data abstraction for improved analyses and data interpretation. Fourth, since MMP is an observational, cross-sectional study, causality cannot be inferred. Fifth, our study had modest response rates and nonresponse bias is possible. Our sampling frame was based on a probabilistic sampling frame and allowed us to examine characteristics of sampled patients (sex, age, race, length of time since HIV diagnosis) to conduct a comparative analysis of respondents and nonrespondents. Research has shown that well-constructed samples with moderate rates have a reduced risk of bias. 40 Finally, although the average age of menopause is 51 years in the United States, and most women in our sample at or above age 50 were likely menopausal, that information was not collected as part of this data set and therefore not available to inform our analyses.
Conclusions
This multivariable analysis that compares older and younger women living with HIV by social, behavioral, and clinical factors adds to the limited research available on this topic. This report highlights the resilience of older women in some areas, but underscores the importance of continuing to deliver messages of medication adherence and sexual health with all HIV-positive women. In addition, messages for routine, clinical STI screening for all HIV-positive sexually active patients may need to be reinforced with clinical providers, along with information about reimbursement for these clinical services. By understanding more about issues across the life span for women living with HIV infection, we can better inform tailored interventions and strategies, and strengthen our ability to improve their outcomes related to HIV prevention and care, consistent with the National HIV/AIDS Strategy. 41
Footnotes
Acknowledgments
We thank participating MMP patients, facilities, project areas, and Provider and Community Advisory Board members. We also acknowledge the contributions of the Clinical Outcomes Team and Behavioral and Clinical Surveillance Branch at CDC and the MMP 2009–2013 project areas (
Author Disclosure Statement
No competing financial interests exist.